


Karina Bittencourt Medeiros1; Layla Comel Corso Perito de Bem2; Priscila Regina Orso Rebellato1; Juliana Merheb Jordão1
Received on: 13/04/2020
Approved on: 04/03/2021
Financial support: None
Conflict of interest: None
Acknowledgment: We thank the patients who constantly inspire us to seek innovation and learning
Study conducted at the Hospital Universitário Evangélico Mackenzie, Curitiba (PR), Brazil
Facial surgeries are often challenging for surgeons due to their complex anatomy, aesthetic and functional importance. Interventions in the cosmetic subunit that comprises the eyebrows can be particularly difficult. This case report aims to demonstrate the use of island flap in this region. We performed the excision of melanocytic nevus, with a good outcome and absence of postoperative complications. This technique is commonly used for facial reconstruction; however, the literature describes only a few cases using this method for eyebrow reconstruction.
Keywords: Scleroderma, Systemic; Microstomia; Lasers; Laser Therapy; Intense Pulsed Light Therapy; Combined Modality Therapy
Scleroderma is a connective tissue disorder characterized by cutaneous fibrosis, vascular abnormalities, and the presence of autoantibodies.1 It is a rare disease, with a prevalence of 8 to 30 cases/100,000 inhabitants. Also, it is more common in women,1 with a peak incidence in the third and fifth decades of life.2
The face is affected by systemic or localized sclerosis.1 Orofacial changes usually begin with the stiffness of the lingual connective tissue and facial skin, leading to a thinning of the lips and nose, and then to the appearance of deep rhytids on the face, an aspect known as mask-like facies. 2 The main oral manifestation is microstomia, present in 70% of patients, characterized by a reduction in the opening of the oral cavity due to sclerosis of the perioral soft tissues.2
Microstomia is defined as an interlabial commissure distance less than 45 mm or an interincisal distance less than 40 mm.3
Clinically, microstomia can negatively interfere with chewing, jaw movements, oral hygiene, and, consequently, quality of life.3 There is an increased incidence of dental caries, periodontal disease, and oral infections (especially by Candida sp) in these patients, at the same time that dental treatments may become impractical depending on the intensity of the oral opening limitation.1 Tongue cancer has a significantly increased frequency in scleroderma patients with a mouth opening of less than 30 mm.4
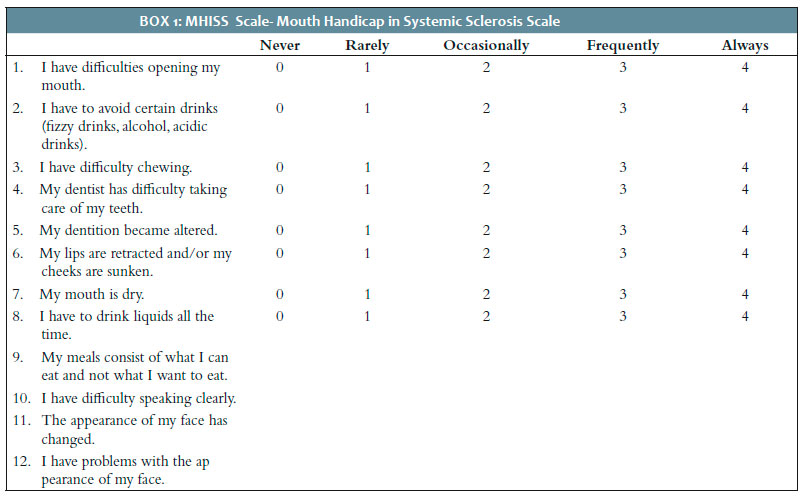
Due to the high prevalence of oral disorders in patients with scleroderma, Mouthon et al. developed the Mouth Handicap in Systemic Sclerosis Scale (MHISS), the first specific measurement instrument to assess the degree of oral disability designed for patients with systemic sclerosis. This scale considers three distinct factors: restriction of mouth opening, presence of Sicca syndrome, and aesthetic concern (mainly skin retraction and presence of telangiectasias). The scale consists of 12 questions, comprised of five answers, with final results ranging from zero to 48 points (Box 1).5
Regarding treatment, there is a consensus in the literature that patients with limited motion range and oral opening should receive guidance on reinforcing oral hygiene. Such patients can be treated with physical and occupational therapy,2 associated with lips and labial commissures lubrication with petroleum jelly.4 Removable partial dentures combined with physiotherapy for oral rehabilitation are highly recommended.4 Some patients may benefit from bilateral commissurotomy,4 skin grafts, and local flaps.6
The CO2 laser can be used to treat perioral rhytids and telangiectasias. In a preliminary study, Barete et al. demonstrated good aesthetic and functional results using CO2 laser, in addition to a significant improvement in the degree of mouth opening.7 Bennani et al. also showed good results with the use of CO2 laser: in four patients with microstomia due to systemic sclerosis, the study exhibited an increase in the interincisal distance after the first session, with an average gain of 5 mm.8 The authors also observed progress regarding lip flexibility and mouth opening, with better phonation, chewing, and dental care.8
Concerning intense pulsed light therapy (IPL), it is known that the longest wavelengths penetrate deeper into the dermis, leading to the stimulation of neocolagenesis, making the skin softer and more elastic.
Comstedt et al. demonstrated good results with the use of IPL in four patients with systemic sclerosis and microstomia, with improved speech articulation, feeding, and dental hygiene care.9
We report a case of a patient with microstomia due to systemic sclerosis, treated with two sessions of IPL and seven sessions of ablative fractional laser (AFL) Erbium:YAG 2940nm. There are no studies in the literature on the treatment of microstomia with Er:YAG 2940nm laser.
A 39-year-old woman, skin phototype IV, had systemic sclerosis diagnosed in 2010. She presented pulmonary fibrosis, esophagopathy, digital ulcers, Raynaud’s phenomenon, ANA positive (1:640) with fine speckled pattern, and microstomia. The patient was using mycophenolate mofetil 1 g/day, rituximab, amlodipine, and omeprazole, with disease control.
In addition to clinical treatment, therapy was proposed to approach the microstomia. During the initial assessment, the patient’s score on the MHISS scale was 22, the inter-commissural distance was 4.7 cm, and the interincisal distance was 3.7 cm. The patient was submitted to the IPL Etherea® platform in the perioral region, with a 695 nm filter, 17 J/cm2 fluency, 40 ms pulse duration, and a second application with 580 nm filter, 16 J/cm2 fluency, 20 ms pulse duration, in two sessions.
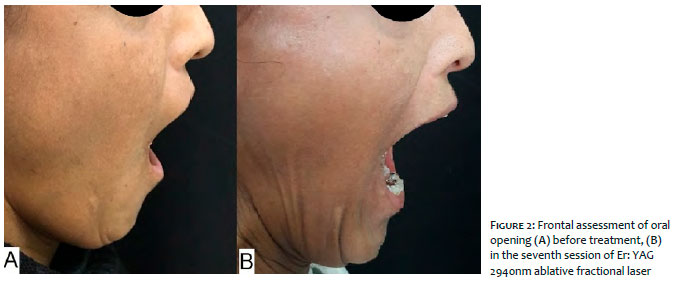
However, she evolved with dyschromia. Then, we opted for treatment with AFL Er:YAG 2940nm Etherea® platform, in the perioral region, in seven sessions, with minimum intervals of 45 days. The sessions were performed from September 2017 to December 2018, with Dual Mode, using an 8 mm tip of 100 thermal microzones. The ablation mode had fluency of 10 J/cm2 and a pulse duration of 300 ms, and the coagulation mode used a fluency of 40 J/cm2 and pulse duration of 5 ms. Throughout the treatment, the patient received oral acyclovir 200 mg, five times a day, for seven days following the session, for prophylaxis of herpes simplex labialis, as well as healing creams and sunscreen. No complications were observed during treatment. In the last session, the score on the MHISS scale was 13, the intercomissure distance was 5.3 cm, and the interincisal distance was 4.5 cm (Figures 1 and 2).
At the end of the treatment, the patient reported she was very satisfied with the result and that she will maintain sessions every six months.
We present a case of microstomia in a patient with systemic sclerosis treated with two sessions of IPL and seven sessions of AFL Erbium:YAG 2940nm.
At the end of the treatment, the patient showed significant clinical improvement with an increase of nine points on the MHISS scale, 6 mm in the intercomissure opening, and 8 mm in the interincisival opening.
In systemic sclerosis, there is an increase in the number of activated fibroblasts with disorganized collagen production, mainly I, III, and IV,10 leading to fibrosis.
In the treatment with AFL Er:YAG 2940nm, we observed histological production of collagen types I, III, and VII, reduction of elastotic material, and elastin, with an increase of tropoelastin. These changes would be responsible for the improvement in skin texture through the healing in the procedure and oral opening.11 Probably, the mechanism of action that justifies the improvement of the patient is the reorganization of the collagen and the replacement of affected fibers with new ones of better quality.
There are few data in the literature on microstomia laser treatments, only case series and pilot studies using IPL and CO2 lasers,8,9 without studies on AFL Er:YAG 2940nm.
Treatment with AFL Er:YAG 2940nm was effective in the clinical and microstomia improvement of a patient with systemic sclerosis.
Therapeutic methods for stimulating collagen can be offered to patients with microstomia with improvement in the impact scores and, mainly, in the quality of life of these patients. AFL Er:YAG 2940nm emerges as a promising therapy in the approach to microstomia in patients with systemic sclerosis.
Karina Bittencourt Medeiros | 0000-0001-8202-6711
Preparation and writing of the manuscript; data collection, analysis, and interpretation; critical literature review; critical revision of the manuscript.
Layla Comel Corso Perito de Bem | 0000-0002-5398-9962
Approval of the final version of the manuscript; study design and planning; critical literature review.
Priscila Regina Orso Rebellato | 0000-0002-4830-2273
Study design and planning; data collection, analysis, and interpretation; intellectual participation in propaedeutic and/or therapeutic conduct of studied cases; critical literature review.
Juliana Merheb Jordão | 0000-0002-8403-2784
approval of the final version of the manuscript; study design and planning; active participation in research orientation; intellectual participation in propaedeutic and/or therapeutic conduct of studied cases; critical revision of the manuscript.
1. Crincoli V, Fatone L, Fanelli M, Rotolo RP, Chialà A, Favia G, et al. Orofacial manifestations and temporomandibular disorders of systemic scleroderma: an observational study. Int J Mol Sci. 2016;17(7):1189.
2. Albilia JB, Lam DK, Blanas N, Clokie CM, Sándor GK. Small mouths...big problems? A review of scleroderma and its oral health implications. J Can Dent Assoc. 2007;73(9):831-6.
3. Yuen HK, Marlow NM, Reed SG, Mahoney S, Summerlin LM, Leite R, et al. Effect of orofacial exercises on oral aperture in adults with systemic sclerosis. Disabil Rehabil. 2012;34(1):84-9.
4. Salem B, Rim BH, Sihem BK, Maher B. Manifestations bucco-dentaires de la sclérodermie systhémique. Pan Afr Med J. 2013;16:114.
5. Mouthon L, Rannou F, Bérezné A, Pagnoux C, Arène JP, Foïs E, et al. Development and validation of a scale for mouth handicap in systemic sclerosis: the Mouth Handicap in Systemic Sclerosis Scale. Ann Rheum Dis. 2007;66(12):1651-5.
6. Dewan SK, Arora A, Sehgal M, Khullar A. Microstomia: a treatment challenge to a prosthodontist. J Clin Diagn Res. 2015;9(4):12-3.
7. Alantar A, Cabane J, Hachulla E, Princ G, Ginisty D, Hassin M, et al. Recommendations for the care of oral involvement in patients with systemic sclerosis. Arthritis Care Res. 2011;63(8):1126-33.
8. Bennani I, Lopez R, Bonnet D, Prevot G, Constantin A, Chauveau D, et al. Improvement of microstomia in scleroderma after carbon dioxide laser treatment. Case Rep Dermatol. 2016;8(2):142-50.
9. Comstedt LR, Svensson A, Troilius A. Improvement of microstomia in scleroderma after intense pulsed light: a case series of four patients. J Cosmet Laser Ther. 2012;14(2):102.
10. Leask A. Matrix remodeling in systemic sclerosis. Semin Immunopathol. 2015;37(5):559-63.
11. El-Domyati M, Abd-El-Raheem T, Abdel-Wahab H, Medhat W, Hosam W, El-Fakahany H, et al. Fractional versus ablative erbium:yttrium-aluminum-garnet laser resurfacing for facial rejuvenation: an objective evaluation. J Am Acad Dermatol. 2013;68(1):103-12.
 All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773
All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773



 Read in Portuguese
Read in Portuguese
 Portuguese PDF
Portuguese PDF
 Print
Print
 Send this article by email
Send this article by email
 How to cite this article
How to cite this article
 Submit a comment
Submit a comment
 Mendeley
Mendeley
 Pocket
Pocket
{kind=link}
{kind=link}
{kind=link}