


Isadora Olenscki Gilli; Karina Bittencourt Medeiros; Juliana Merheb Jordão
Received on: 24/08/2020
Approved on: 19/03/2021
Financial support: None
Conflict of interest: None
Acknowledgments: We thank the employees who provided, directly or indirectly, the conditions for conducting this study and the preceptors for their valuable contributions to this project, for sharing scientific knowledge, professionalism, and stimulating research
Study conducted at the Hospital Universitário Evangélico Mackenzie, Curitiba (PR), Brazil
Solar lentigo is present in 90% of the population over 50 years of age andcharacterizes as hyperchromic spots in photoexposed regions. It increases with aging and is more frequent in light skin. There are several therapeutic modalities, which achieve better results whenassociated. We describe the case of a 62-year-old man with Fitzpatrick skinphototype II, complaining of brownish macules in nasal dorsum for eight years. The patient underwent a skin biopsy, and the histological study confirmed solar lentigo. The patient was treated with six sessions of Intense Pulsed Light associated with Erbium-Yag2940 nm Laser with a good clinical result.
Keywords: Skin aging; Lentigo; Melanosis; Low Intensity Laser Therapy; Intense Pulsed Light Therapy
Solar lentigos (SL) are associated with chronic exposure to ultraviolet radiation (UV). They usually present as hyperchromic macules of different shades of brown, preferably in photoexposed areas, in individuals with low skin phototypes, between the fourth and sixth decades of life.1,2
Histologically, epidermal hyperplasia is associated with hyperpigmentation and actinic damage of the dermis, in addition to an irregular elongation of the grooves with hyperpigmentation predominantly at the tips of the epidermal crests.3 Structural studies reveal that melanocytes show signs of changes in their function, with increased epidermal growth concomitant with melanocytic proliferation, corroborated by a large number of melanosomes in complexes and by ultrastructural melanosomes.3
Therapy for solar lentigos can be divided into two major categories: physical and topical treatment. Currently, several topical therapies are in use, including hydroquinone, tretinoin, adapalene, and, more recently, a stable fixed combination of mequinol and tretinoin. Although topical therapies present satisfactory aesthetic results, they usually require a longer time and are not so effective. In addition to active therapy, patients are generally advised to use sunscreens as a preventive treatment to maintain treatment success.
Physical modalities include Intense Pulsed Light (IPL), lasers, chemical peelings, ultrasonic depigmentation, microdermabrasion, among other options. These are often used with excellent clinical success rates. However, this type of therapy should be balanced with the associated adverse events and recurrence rates of lesions. These resources, associated or not, act superficially, such as depigmenting therapy, bleaching, and cell renewal, providing effective results in the short and medium-term. Studies suggest that these combined therapies with preventive maintenance with photoprotection and lighteners can provide effective and satisfactory results.4,5 Among them, it is worth mentioning that the combination of Intense Pulsed Light and laser can be a good option, with very satisfactory aesthetic results.5
Literature has demonstrated that therapy with Intense Pulsed Light (IPL) alone combined with other types of treatment can be equally effective or even superior to ablative laser systems with melanin affinity.5-7
Studies have demonstrated that the treatment with ablative laser Erbium-YAG for solar lentigos management is effective by vaporizing the pigment-containing epidermis. However, there are adverse events such as post-inflammatory hyperpigmentation.7,8
Conceptually, the combination of technologies can potentially increase treatment effectiveness and reduce the risk of adverse events. It is expected that, once two different but complementary mechanisms are combined, the duration of treatment can also be reduced.
A 62-year-old man was referred to the Dermatology Service of the Mackenzie Evangelical University Hospital in 2017 to investigate the appearance of asymptomatic brownish stains on the nasal dorsum nine years ago. The examination revealed a well-defined brownish stain on the nasal dorsum and bilateral cheek. Biopsy was performed in the nasal region to rule out an association with pigmented actinic keratosis and lentigo maligna. Histological examination of the skin showed epidermal hyperplasia without atypia, hyperkeratosis, and solar elastosis, compatible with solar lentigo (Figure 1).
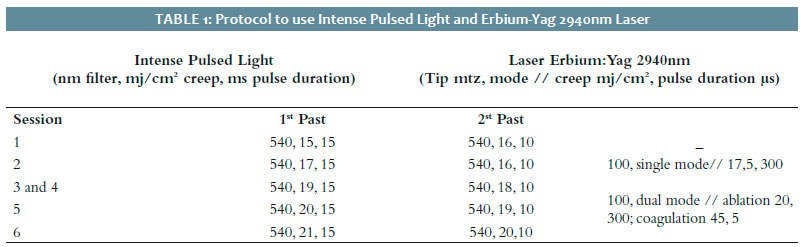
The patient started treatment with IPL (Etherea®Platform) with a 540 nm filter in two passes (Table 1). After the session, a multi-purpose soothing repairing balm (Cicaplast®) was prescribed, associated with a sun protection factor.
One month after this first IPL session, we performed five further IPL sessions in association with Erbium-YAG 2940nm Laser (100MTZ tip) with one-month intervals between them (Table 1).
A subsequent evaluation showed significant improvement of the nasal spots (Figure 1).
Solar lentigos (SL) are also known as solar melanosis and actinic lentigos. The potential negative social impact of this condition should be considered, given that these lesions appear in highly visible parts of the body, such as the face, neck, hands, and forearms. The hyperchromic macules can be considered the first signs of the photoaging process, which can also significantly impact patients’ quality of life. The incidence of SL increases with age, affecting more than 90% of white people over 50 years of age.4
In the differential diagnosis, SL should be differentiated from ephelides, pigmented actinic keratosis, flat seborrheic keratosis, melanocytic neoplasia, and malignant melanoma. They can be distinguished based on clinical aspects and, if not possible, histopathological differentiation may be necessary.7 In general, skin pigmented lesions are frequent targets of combined laser treatment and IPL.6
In the case of solar lentiginous lesions, the main target of treatment with IPL is the melanosome.6 The effect of the treatment is cumulative, and a few sessions are necessary, usually from three to six, every three to four weeks.
Combined with this therapy, the use of ablative lasers can be an effective alternative to treat benign pigmented lesions, as in our case. This may be a good option especially when there is keratinocyte hyperplasia, once ablation leads to better quality epidermis renewal.
Regarding the association of these techniques, we initially opted for using the IPL alone, seeking the lesion whitening. As the response obtained was less than expected, we decided to associate Laser Erbium-YAG 2940nm in its ablative mode to IPL in the second session to renew the epidermis, thus promoting a more accentuated whitening. After achieving this result and now aiming at improving the skin texture, the Laser parameter was modified from the third session onwards to include the coagulation mode. This way, the dermis and epidermis were treated. Raising IPL parameters at each session but maintaining the pulse duration at 15ms and 10ms had the main objective of reaching different skin depths.
Although the literature reports numerous cosmetic applications using the laser Erbium-YAG, they have been used more frequently in the facial rejuvenation of photodamaged skin, including dyschromias.6
IPL is a highly versatile, safe, and effective modality to treat benign pigmented lesions. The association of ablative lasers offers the additional benefit of promoting the ablation of hyperplastic portions of the epidermis, directing skin homogenization. Once SL is an injury with melanic and hyperkeratotic components, the combined therapies targeting these two elements are more effective. Many publications corroborate the effectiveness of the phototherapy technique of Intense Pulsed Light associated with ablative Laser in the depigmentation of skin spots, in particular senile. It can be used as a resource in the process of whitening hyperchromic spots from photoaging.5-7 Combining technologies made possible an effective treatment with faster and better results than monotherapy would probably have.
Isadora Olenscki Gilli | 0000-0002-2795-5427
Approval of the final version of the manuscript; study design and planning; preparation and writing of the manuscript; data collection, analysis, and interpretation; active participation in research orientation; intellectual participation in propaedeutic and/or therapeutic conduct of studied cases; critical literature review.
Karina Bittencourt Medeiros | 0000-0001-8202-6711
Approval of the final version of the manuscript; study design and planning; preparation and writing of the manuscript; data collection, analysis, and interpretation; active participation in research orientation; intellectual participation in propaedeutic and/or therapeutic conduct of studied cases; critical literature review.
Juliana Merheb Jordão | 0000-0002-8403-2784
Approval of the final version of the manuscript; study design and planning; preparation and writing of the manuscript; data collection, analysis, and interpretation; active participation in research orientation; intellectual participation in propaedeutic and/or therapeutic conduct of studied cases; critical literature review.
1. Vimercati L, De Maria L, Caputi A, Cannone ESS, Mansi F, Cavone D, et al. Non-melanoma skin cancer in outdoor workers: a study on actinic keratosis in italian vavy personnel. Int J Environ Res Public Health. 2020;17(7):2321.
2. Navarrete-Dechent C, Scope A, Tsao H, Marghoob NG, Sober AJ, Marghoob AA. Acquired precursor lesions and phenotypic markers of increased risk for cutaneous melanoma. In. Balch CM, Atkins MB, Garbe C, Gershenwald JE, Halpern AC, Kirkwood JM, et al., editors. Cutaneous Melanoma. Cham: Springer International Publishing; 2020. p. 501-24.
3. Maeda K. Large melanosome complex is increased in keratinocytes of solar lentigo. Cosmetics. 2017;4(4):49.
4. Ortonne J-P, Pandya AG, Lui H, Hexsel D. Treatment of solar lentigines. J Am Acad Dermatol. 2006;54(5):S262-71.
5. Feng H, Kauvar ANB. Lentigines and dyschromia. In: Alam M, editors. Evidence-based procedural dermatology. Cham: Springer International Publishing; 2019. p. 917-31.
6. Alster T, Husain Z. The role of lasers and intense pulsed light technology in dermatology. Clin Cosmet Investig Dermatol. 2016;9:29-40.
7. Passeron T, Genedy R, Salah L, Fusade T, Kositratna G, Laubach H -J., et al. Laser treatment of hyperpigmented lesions: position statement of the European Society of Laser in Dermatology. J Eur Acad Dermatol Venereol. 2019;33(6):987-1005.
8. Tian BCA. Novel low fluence combination laser treatment of solar lentigines in type III Asian skin. J Cutan Aesthet Surg. 2015;8(4):230.
 All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773
All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773



 Read in Portuguese
Read in Portuguese
 Portuguese PDF
Portuguese PDF
 Print
Print
 Send this article by email
Send this article by email
 How to cite this article
How to cite this article
 Submit a comment
Submit a comment
 Mendeley
Mendeley
 Pocket
Pocket
{kind=link}
{kind=link}