


Felipe Amado Cerqueira Gomes; Roney Gonçalves Fechine Feitosa; Flávia Modelli Vianna Waisberg; An Wan Ching; Lydia Masako Ferreira
Received on: 12/05/2020
Approved on: 04/03/2021
Financial support: None
Conflict of interest: None
Study conducted at the Escola Paulista de Medicina, Universidade Federal de São Paulo, São Paulo (SP), Brazil
The lower limbs defects reconstructions are complex and impose a challenge for the reconstructive surgeon. The use of local fasciocutaneous flaps can be helpful when dealing with these defects. We report the case of two patients who underwent calcaneal reconstruction surgery using a medial plantar artery flap after the resection of acral melanoma. This flap provides a resistant and long-lasting tissue with a neurovascular sparing technique. The preserved sensitivity contributes to good long-term outcomes. The neurovascular flaps, such as medial plantar artery flap, promote good adaptation and healing regarding foot and heel defects.
Keywords: Plastic surgery; Lower extremity; Melanoma; Surgical flaps
The reconstruction of defects in the distal third of the lower limbs using local flaps is a real challenge for the plastic surgeon. The thin skin of the neighboring region, associated with the scarcity of soft tissues and the relative immobility of the structures, restricts the therapeutic options and hinders good final results. Harrison and Morgan initially proposed the use of the medial plantar flap for the treatment of these injuries in 1981,1 and its use has become very popular with the advancement of anatomical-vascular knowledge in the region. It is based on a fasciocutaneous flap on the plantar arch and provides a very versatile tissue for covering defects of the foot, heel, and ankle.
This pedicled flap spares the neurovascular bundle and preserves the cutaneous sensory branches, transferring an innervated skin segment to the recipient area.2 Thus, it provides the flap’s long-lasting preservation and contributes to the patient’s rehabilitation.
Furthermore, because it is a local flap, it maintains the characteristics of the plantar skin with high resistance and durability, capable of withstanding high pressures and shear forces.3
This study aims to report two cases of calcaneal reconstruction after resection of acral melanoma using the innervated medial plantar fasciocutaneous flap.
This is a primary, retrospective, clinical study conducted in a single center. The Clinical Case Reporting Guideline Development (CARE) was used4 to report a series of two cases conducted by the Microsurgery Sector of Plastic Surgery Discipline at the Federal University of São Paulo (Unifesp), respecting all ethical precepts and rights, among others ensured.
A 60-year-old woman presented an irregular and painful lesion in the region of the right heel with progressive growth for three years. She reported difficulty in accessing the specialized health system, leading to a delay in diagnosis. Physical examination revealed an irregular and ulcerated melanocytic tumor in the right heel with a nodular growth component. The lesion was approximately 8 cm long, painful, and adhered to deep planes. Dorsalis pedis and posterior tibial pulse were present on palpation. There were no lymph nodes in the popliteal and inguinal regions (Figure 1).
Following the investigation, an incisional tumor biopsy was performed, showing an acral melanoma with Breslow thickness of 3.4 mm, ulceration, and eight mitoses/field. The disease was classified as locally advanced with cleavage in the calcaneus. We opted for resection with 2 cm margins and sentinel lymph node biopsy. The anatomopathological result was compatible with acral melanoma with free margins and negative sentinel lymph node (T3bN0M0 Clark V). The skin cancer treatment team performed immediate reconstruction using elastic sutures and biological dressings (Figure 2).
After two years of follow-up, the patient did not present disease evolution and was referred to the Microsurgery Sector of Plastic Surgery at Unifesp for late reconstruction. The defect extended for 9.3 cm x 8.6 cm. Thus we opted for reconstruction using an innervated medial plantar flap, as shown in the images. The patient is currently in the 6th postoperative month with good evolution, showing no difficulty walking or tumor recurrence (Figure 3).
A 32-year-old woman was referred from an external service with a diagnosis of acral melanoma in the left heel. She had already undergone an excisional biopsy, with the anatomopathological result showing Breslow thickness of 0.7 mm, without mitosis or ulceration (T1aN0M0 Clark II).
Physical examination showed a good-looking scar on the heel, presence of dorsalis pedis and posterior tibial pulse, and absence of lymph node enlargement in the popliteal and inguinal region.
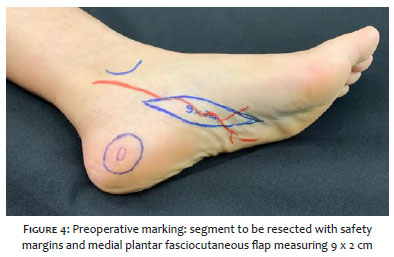
The staff decided to expand the surgical margins by 1 cm, resulting in a bloody area with 3.5 cm in diameter. We opted for reconstruction with a medial plantar fasciocutaneous flap, as shown in the figures 4 and 5.
Fasciocutaneous flaps should be considered when dealing with complex lesions or extensive defects in the distal region of the lower limbs. Among the possible options, the medial plantar flap has a prominent role in an area with the function to support weight, friction, and high shear forces.5 This flap provides a highly resistant coating with a thick epidermis, specialized subcutaneous tissue, and fascia with good adhesion to deep tissues.
The medial plantar artery is a branch of the posterior tibial artery responsible for maintaining the irrigation of this flap.6 By emitting superficial and deep branches, it irrigates the muscles of the hallux and skin of the plantar region. The possibility of transferring this flap to several surrounding locations and the viability when transferred to previously infected areas evidences this artery’s good blood flow. Adequate blood supply favors good early and late outcomes (Figure 6).
Another important characteristic for the success of the medial plantar flap is nerve preservation. The dissection of the medial plantar nerve and its branches makes it possible to maintain the sensitivity of this skin segment without impairing the innervation of the rest of the forefoot. The sensory cutaneous branches preserve the perception of stimuli, such as pressure, pain, and thermal sensitivity, contributing to the protection and preservation of the flap.7 In patients with some degree of peripheral neuropathy, this property is crucial.
The unique skin characteristic of the plantar region should be highlighted. The plantar skin is highly specialized to support the body weight, with a thick epidermis, richly keratinized, and an additional protective layer called stratum lucidum. Add to that the support of a very differentiated and resistant subcutaneous tissue permeated with fibrous septa. Because it comes from a neighboring region, the medial plantar flap maintains the “like with like” property, replacing the skin of the plantar area with another skin with the same characteristics (Figure 7).
For reconstructions of distal defects in the lower limbs, the surgeon may opt for alternative flaps. The reverse superficial sural artery flap (RSSAF), propeller flap (reverse flow axial flap), or even microsurgical flaps are good alternatives and should be considered in surgical planning.8 However, because it does not have the “like with like” characteristics, it is not usually the first option for reconstructing the plantar region.
It is worth mentioning that, although there is no transfer of the muscle layer, the medial plantar fasciocutaneous flap promotes a cushion with adequate thickness and durability. The transferred fascia adheres well to bony prominences and deep structures in the receiving area, promoting resistant anchorage and hampering shearing.9 Also, secondary contraction promotes a “mushroom effect”, which contributes to the thickening of the flap, making its thickness more similar to the original tissue (Figure 8).
This type of flap has additional value in patients with diabetic neuropathy and distal ulcerations.10, 11 Ulcers in these patients are challenging to treat and often lead to deep defects, with exposure of the muscle and bone layer. Usually, such patients have already undergone conservative treatments with little or no improvement. Although simple rotation or advancement flaps achieve good outcomes in minor defects, they are usually insufficient for complex ulcerations. In these cases, fasciocutaneous flaps show better results.
The medial plantar flap is an excellent option for reconstructing calcaneal defects due to its versatility,12 resistance, and reproducibility, with relatively constant anatomy. It allows an innervated flap without the need for nerve grafting, and it replaces a highly specialized tissue with another with similar characteristics. In line with the literature,13 our experience with such flaps encourages short and long-term outcomes and should be considered an option for this type of treatment.
Felipe Amado Cerqueira Gomes | 0000-0003-3915-582X
Statistical analysis; approval of the final version of the manuscript; study design and planning; preparation and writing of the manuscript; data collection, analysis, and interpretation; critical literature review; critical revision of the manuscript.
Roney Gonçalves Fechine Feitosa | 0000-0001-6000-743X
Statistical analysis; approval of the final version of the manuscript; study design and planning; preparation and writing of the manuscript; data collection, analysis, and interpretation; active participation in research orientation; intellectual participation in propaedeutic and/or therapeutic conduct of studied cases; critical literature review; critical revision of the manuscript.
Flávia Modelli Vianna Waisberg | 0000-0002-8336-5026
Approval of the final version of the manuscript; study design and planning; intellectual participation in propaedeutic and/or therapeutic conduct of studied cases; critical revision of the manuscript.
An Wan Ching | 0000-0002-9205-9899
Approval of the final version of the manuscript; study design and planning; intellectual participation in propaedeutic and/or therapeutic conduct of studied cases; critical revision of the manuscript.
Lydia Masako Ferreira | 0000-0001-6661-1830
Approval of the final version of the manuscript; study design and planning; intellectual participation in propaedeutic and/or therapeutic conduct of studied cases; critical revision of the manuscript.
1. Website n.d. Harrison DH, Morgan BD. The instep island flap to resurface plantar defects. Br J Plast Surg. 1981;34(3):315-8. PMID: 7272570 DOI: http://dx.doi.org/10.1016/0007-1226(81)90019-9 (accessed May 3, 2020).
2. Khan FH, Beg MSA, Obaid-Ur-Rahman. Medial Plantar Artery Perforator Flap: Experience with Soft-tissue Coverage of Heel. Plast Reconstr Surg Glob Open 2018;6:e1991.
3. Zelken JA, Lin C-H. An Algorithm for Forefoot Reconstruction With the Innervated Free Medial Plantar Flap. Ann Plast Surg 2016;76:221-6.
4. Gagnier JJ, Kienle G, Altman DG, Moher D, Sox H, Riley D, et al. The CARE Guidelines: Consensus-based Clinical Case Reporting Guideline Development. Glob Adv Health Med 2013;2:38-43.
5. Haug MD, Valderrabano V, Rieger UM, Pierer G, Schaefer DJ. [Anatomically and biomechanically based treatment algorithm for foot and ankle soft tissue reconstruction]. Handchir Mikrochir Plast Chir 2008;40:377-85.
6. Blanton C, Kercado M, Nordquist T, Masadeh S, Rodriguez P, Rodriguez-Collazo E. Medial Plantar Artery Common Origin to Determine Incision Placement for the Fasciocutaneous Flap: A Cadaveric Study. J Foot Ankle Surg 2020;59:462-4.
7. Trevatt AEJ, Filobbos G, Ul Haq A, Khan U. Long-term sensation in the medial plantar flap: a two-centre study. Foot Ankle Surg 2014;20:166-9.
8. Koshima I, Narushima M, Mihara M, Nakai I, Akazawa S, Fukuda N, et al. Island medial plantar artery perforator flap for reconstruction of plantar defects. Ann Plast Surg 2007;59:558-62.
9. Kim SW, Hong JP, Chung YK, Tark KC. Sensate sole-to-sole reconstruction using the combined medial plantar and medialis pedis free flap. Ann Plast Surg 2001;47:461-4.
10. Cohen BK, Zabel DD, Newton ED, Catanzariti AR. Soft-tissue reconstruction for recalcitrant diabetic foot wounds. J Foot Ankle Surg 1999;38:388-93.
11. Houlind K. Surgical revascularization and reconstruction procedures in diabetic foot ulceration. Diabetes Metab Res Rev 2020;36 Suppl 1:e3256.
12. Bonte A, Bertheuil N, Menez T, Grolleau J-L, Herlin C, Chaput B. Distally Based Medial Plantar Flap: A Classification of the Surgical Techniques. J Foot Ankle Surg 2018;57:1230-7.
13. Park JS, Lee JH, Lee JS, Baek JH. Medialis pedis flap for reconstruction of weight bearing heel. Microsurgery 2017;37:780-5.
 All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773
All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773



 Read in Portuguese
Read in Portuguese
 Portuguese PDF
Portuguese PDF
 Print
Print
 Send this article by email
Send this article by email
 How to cite this article
How to cite this article
 Submit a comment
Submit a comment
 Mendeley
Mendeley
 Pocket
Pocket
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}