


Paula Hitomi Sakiyama; Thiago Augusto Ferrari; Raíssa Rigo Garbin; Alexandre Luiz Weber
Received on: 10/05/2020
Approved on: 04/03/2021
Financial support: None
Conflict of interest: None
Study conducted at the Dermatology Service of the Hospital Santa Casa de Curitiba, Curitiba (PR), Brazil
O queratoacantoma (QA), apesar de frequente na prática diária, é um tumor que gera questionamentos. O aspecto mais intrigante associa-se à sua posição no limite entre malignidade e benignidade. A abordagem do tumor, bem como sua classificação, é controversa. Na definição da conduta, é importante levar em conta o potencial de transformação para carcinoma espinocelular. Desse modo, a excisão cirúrgica é a terapia de escolha, sempre que possível. Algumas situações merecem atenção adicional, como a imunossupressão associada. Neste artigo, relatamos um caso de QA gigante em um paciente com síndrome da imunodeficiência adquirida tratado com cirurgia micrográfica de Mohs.
Keywords: Ceratoacantoma; Retalhos Cirúrgicos; Neoplasias Nasais; Neoplasias Cutâneas; Cirurgia de Mohs; Síndrome de Imunodeficiência Adquirida; HIV; Imunossupressão
Keratoacanthoma (KA), although common, is a tumor that still raises questions. Although described in 1888 by Sir Jonathan Hutchinson, its etiology, epidemiology, histopathological diagnostic criteria, prognosis, and treatment guidelines remain controversial until today. The most intriguing aspect is its position on the limit between benignity and malignancy, which must be considered when defining the conduct.1
Several clinical presentations are described, and solitary KA is the most common manifestation. The giant KA represents an unusual variant, characterized by a lesion larger than 2 cm in diameter, with a preference for the face, especially affecting the nose and eyelids.2
We report a case of giant KA in an immunosuppressed patient due to infection by the human immunodeficiency virus (HIV), treated with Mohs micrographic surgery (MMS).
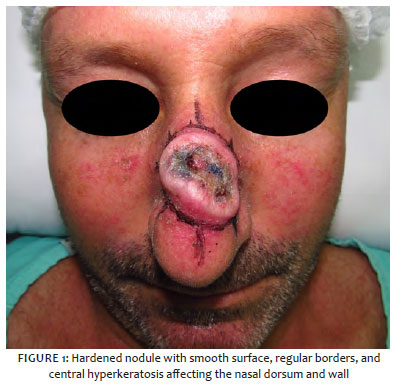
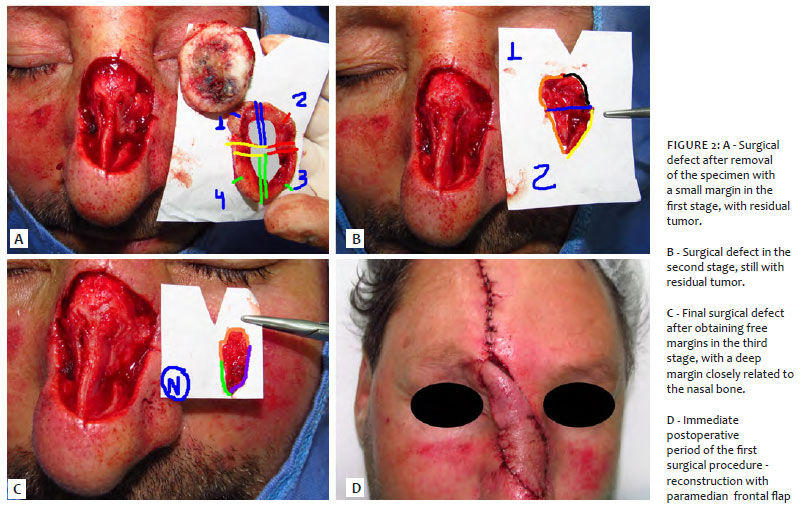
A 47-year-old man presented KA in the nasal region, relapsed after conventional surgery excision with 4 mm margins two months before. He received recent HIV diagnosis, and was in regular use of antiretroviral therapy, with undetectable viral load (CV). However, he still presented low CD4+ lymphocytes levels (138 cells/mm3), characterizing immunosuppression. The examination revealed a hardened nodule with a smooth surface, regular borders, and central hyperkeratosis, affecting the nasal dorsum and wall, measuring 4.4 x 3.8 cm, with absence of palpable lymph node enlargement (Figure 1). Additional investigation with computerized axial tomography scan and nuclear magnetic resonance revealed involvement restricted to soft tissues. New anatomopathological examination was compatible with invasive squamous cell carcinoma (SCC) type KA. Because it was a recurrent, extensive tumor, and in a high-risk location, a MMS approach was indicated. The surgical procedure was performed obtaining free margins in the third stage. The surgical defect was reconstructed using a paramedian forehead interpolated flap (Figure 2). Due to the close relationship between the deep margin and the nasal bone, identified during the intraoperative period, we chose adjuvant radiotherapy. The patient is being followed up, with good evolution and no signs of recurrence (Figure 3).
The relationship between KA and SCC is widely discussed. While some authors consider the KA as a scaly proliferation with a distinct follicular base that generally follows a benign clinical course, others claim that it is a clinical variant of SCC prone to spontaneous regression, but with occasional aggressive behavior and even metastasis. The conclusion of the problem is hampered by the lack of anatomopathological criteria that differentiate the two entities. Reports of transformation of KA into SCC also suggest the possibility of dealing with different stages of the same entity.3,4,5,6,7 For this reason, some specialists prefer to use broader terms in histopathological reports, such as “SCC - KA type”, “probable KA”, or “SCC cannot be ruled out”, to define the tumor.1
The approach to solitary KA is controversial, but it is important to consider its potential to transform into invasive SCC and metastasize defines the treatment. Expectant conduct is questionable, unless clear signs of resolution are present. It can cause considerable damage in major lesions due to destruction of underlying structures or unsightly scar resulting from involution.1,2 Other therapeutic options include curettage and electrodissection, intralesional application of chemotherapeutic agents, radiotherapy, and topical agents. However, the disadvantage is that they do not allow the histopathological confirmation of the complete removal of the tumor. Thus, surgical excision is the first-line therapy, whenever possible. There is no specific determination on the margins in conventional surgery, considering the same ones recommended for non-invasive SCC (4-6 mm).1 Adjuvant radiotherapy is an option in selected situations, such as in cases of higher clinical aggressiveness or even in giant KA, such as the case presented.2,8
MMS shows the lowest recurrence rate among all modalities.8 The procedure allows intraoperative assessment of 100% of the tissue margins, different from the conventional surgical approach, where only representative sections of the tumor are examined, limited to less than 0.01% to 1% of the entire excised margin. When available, it is the method of choice for extensive lesions (larger than 2 cm) or those that affect critical areas, where tissue preservation is desired due to the advantage of minimizing the size of the surgical defect before the wound closes. MMS is also indicated in immunosuppressed patients because of the higher frequency and aggressiveness of keratinocytic carcinomas in this group.10,11,12
The increased risk of SCC in immunosuppressed individuals is well established. Regarding specifically to HIV, studies show that infected people have higher rates of SCC recurrence, even among younger individuals with well-controlled HIV, suggesting that the disease itself may represent an additional factor in immunosuppression.13,14 Moreover, concerning the development of subsequent SCCs, a relationship between an increased risk of new tumors and a lower number of CD4 and high CV was observed. It suggests that, in this context, there is an association with immunodeficiency biomarkers.14 Therefore, due to the relationship between KA and SCC, patients with HIV require special attention in determining the ideal therapy, with MMS being an excellent option.
The case reported corroborates the greater aggressiveness in this group since tumor recurrence occurred after conventional technique excision, considered a first-line method to approach KA.
Patients with KA should be monitored after treatment for the possibility of recurrence or, due to Koebner’s phenomenon, the development of a new lesion in the area previously addressed, usually between one week and eight months after the intervention.
Guidance to avoid possible triggering factors, such as prolonged and intense exposure to ultraviolet light and medical or cosmetic procedures in photodamaged skin areas, are also important.1 It is noteworthy that HIV patients require additional attention during follow-up, considering influence of the disease on the risk of SCC.13,14
Giant KA is a rapidly evolving tumor that can reach large dimensions, causing local destruction and presenting the possibility of malignancy. MMS represents a good treatment option in these cases, especially in the presence of additional risk factors, such as immunosuppression, given the possibility of a complete evaluation of margins and high cure rates, in addition to the aesthetic and functional benefits resulting from preserving healthy tissue.
Paula Hitomi Sakiyama | 0000-0001-7813-8294
Approval of the final version of the manuscript; study design and planning; preparation and writing of the manuscript; data collection, analysis, and interpretation; revisão critical literature review; critical revision of the manuscript.
Thiago Augusto Ferrari | 0000-0003-4874-4837
Approval of the final version of the manuscript; data collection, analysis, and interpretation; critical literature review; critical revision of the manuscript.
Raíssa Rigo Garbin | 0000-0002-9771-1209
Statistical analysis; approval of the final version of the manuscript; study design and planning; data collection, analysis, and interpretation; active participation in research orientation; critical literature review; critical revision of the manuscript.
Alexandre Luiz Weber | 0000-0002-4862-5777
Approval of the final version of the manuscript; study design and planning; data collection, analysis, and interpretation; active participation in research orientation; intellectual participation in propaedeutic and/or therapeutic conduct of studied cases; critical literature review; critical revision of the manuscript.
1. Kwiek B, Schwartz RA. Keratoacanthoma (KA): An update and review. J Am Acad Dermatol. 2016;74(6):1220-33.
2. Bogner PN, Cheney RT, Zeitouni NC. Giant keratoacanthoma: case report and review of the English literature. Am J Dermatopathol. 2014;36(3):252-7.
3. Nagarajan P. Differentiating keratoacanthoma from squamous cell carcinoma-In quest of the holy grail. Nagarajan P. J Cutan Pathol. 2020;47(4):418-20.
4. Weedon D, Malo J, Brooks D, Williamson R. Keratoacanthoma: is it really a variant of squamous cell carcinoma? ANZ J Surg. 2010;80(3):129-30.
5. Ko CJ. Keratoacanthoma: facts and controversies. Clin Dermatol 2010;28(3):254-61.
6. Gleich T, Chiticariu E, Huber M, Hohl D. Keratoacanthoma: a distinct entity? Exp Dermatol. 2016;25(2):85-91.
7. Nassif PW, Basatazini Junior M, Mello Junior EJF, Figueiredo RBP. Carcinoma espinocelular em couro cabeludo inicialmente diagnosticado como queratoacantoma. Surg Cosmet Dermatol. 2010;2(1):63-6.
8. Garcia-Zuazaga J, Ke M, Lee P. Giant keratoacanthoma of the upper extremity treated with mohs micrographic surgery: a case report and review of current treatment modalities. J Clin Aesthet Dermatol. 2009;2(8):22-5.
9. Tran DC, Li S, Henry AS, et al. An 18-year retrospective study on the outcomes of keratoacanthomas with different treatment modalities at a single academic center. Br J Dermatol 2017;177(6):1749-51.
10. Cernea SS, Gontijo G, Pimentel ERA, Tarlé RG, Tassara G, Ferreira JASLB, et al. Diretrizes de indicações de cirurgia micrográfica de Mohs nos tumores da pele. An Bras Dermatol. 2016;91(5):621-7.
11. Wong, E., Axibal, E., & Brown, M. Mohs Micrographic Surgery. Facial Plastic Surgery Clinics of North America. 2019;27(1):15-34.
12. Ad Hoc Task Force, Connolly SM, Baker DR, Coldiron BM, Fazio MJ, Storrs PA, et al. AAD/ACMS/ASDSA/ASMS 2012 appropriate use criteria for Mohs micrographic surgery: a report of the American Academy of Dermatology, American College of Mohs Surgery, American Society for Dermatologic Surgery Association, and the American Society for Mohs Surgery. J Am Acad Dermatol. 2012;67(4):531-50.
13. Asgari MM, Ray GT, Quesenberry CP Jr, Katz KA, Silverberg MJ. Association of multiple primary skin cancers with human immunodeficiency virus infection, CD4 count, and viral load. JAMA Dermatol. 2017;153(9):892-96.
14. Hausauer AK, Maurer T, Leslie KS, Parvataneni R, Stuart SE, Chren MM. Recurrence after treatment of cutaneous basal cell and squamous cell carcinomas in patients infected with human immunodeficiency virus. JAMA Dermatol. 2013;149(2):239-41.
 All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773
All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773



 Read in Portuguese
Read in Portuguese
 Portuguese PDF
Portuguese PDF
 Print
Print
 Send this article by email
Send this article by email
 How to cite this article
How to cite this article
 Submit a comment
Submit a comment
 Mendeley
Mendeley
 Pocket
Pocket
{kind=link}
{kind=link}
{kind=link}