


Lívia Arroyo Trídico1,2; Paulo Henrique Miranda Ribeiro3
Received on: 25/07/2018
Approved on: 09/02/2021
Financial support: None
Conflict of interest: None
Study conducted at the Medical School of São José do Rio Preto, São José do Rio Preto (SP), Brazil
Osteoma cutis is a rare tumor characterized by the presence of bone tissue in the dermis and/or hypodermis. We describe the case of a patient diagnosed with osteoma cutis on the scalp for approximately ten years with progressive growth and local alopecia area. The patient underwent surgical excision of the lesion using the rotation flap "S" italic technique to reconstruct the area aiming at the best possible aesthetic result.
Keywords: Nasal Surgical Procedures; Neoplasms, Basal Cell; Nose Neoplasms
Osteoma cutis is a rare lesion characterized by bone tissue in the skin, with unknown etiology.1 It manifests with the formation of bone nodules in the dermis and/or hypodermis, consisting of lamellar bone with the presence of osteocytes in the center and osteoclasts in the peripheral area, similar to the mesenchymal bones. 2,3 Although it is a benign lesion, it can lead to skin deformities in the affected areas, causing aesthetic changes and triggering psychological consequences to the patient.4
The disease affects mainly the face, scalp, chest, and extremities. The lesions are generally painless and asymptomatic, presenting as hard, irregular, and circumscribed papules, nodules, or single or multiple plaques, although they may also present as miliary lesions.5,6,7 They are usually skin-colored and, occasionally, they cause skin discoloration that becomes white or yellowish.8
We classify osteoma cutis lesions as primary or secondary. Primary osteoma cutis (POC) occurs in 15% of cases, is not associated with a local history of trauma or previous skin lesion, and can occur in isolation or in association with a metabolic dysfunction syndrome (the main associated syndromes are Albright’s hereditary osteodystrophy, progressive ossifying fibrodysplasia, progressive osseous heteroplasia, and plaque-like osteoma cutis). The secondary osteoma cutis (SOC) is the most common type. It is responsible for 85% of the cases and it is associated with previous skin lesions, such as scleroderma, pilomatricoma, nevus, dermatomyositis, basal cell carcinoma, scars, skin inflammation, trauma, and epidermal cyst, among others.4,9,10
We report a case of large primary osteoma cutis located on the scalp and its surgical treatment.
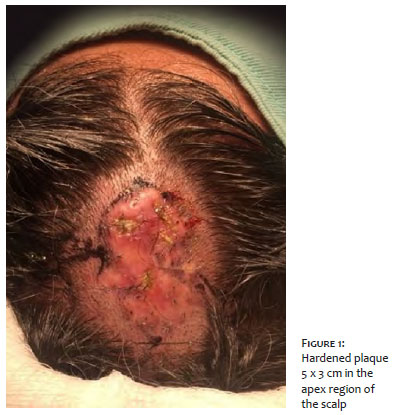
A 39-year-old man presented a lesion on the scalp for about ten years, asymptomatic and with progressive growth. A well-defined alopecia plaque with a hardened appearance and some yellowish nodules in the center characterized the lesion, which measured 5 cm x 3 cm in diameter and was located at the apex of the scalp (Figure 1). One of the nodular lesions was biopsied, and the histopathological diagnosis was osteoma cutis. The patient had no previous clinical lesion at the tumor site, and serum calcium and parathyroid hormone levels were normal. Therefore, we classified the lesion as isolated primary osteoma cutis.
We chose to perform the surgical treatment of the lesion since it presented progressive growth, leading to alopecia and consequent aesthetic impairment.
Given the lesion’s size and location, surgical treatment has become a challenge, aiming at reconstruction with the best possible functional and aesthetic result.
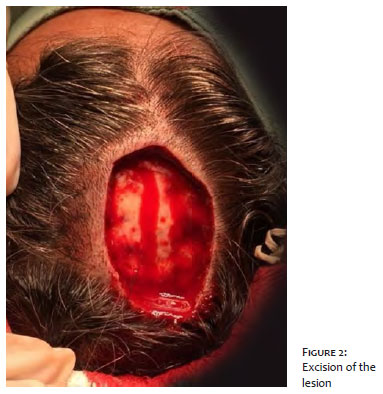
The lesion was excised with a 0.5 cm safety margin, including cutaneous and subcutaneous tissue until reaching the galea aponeurotica (Figures 2 and 3). To repair the excised area, we decided to perform the rotation flap, performing the semicircular movement of rotation of the skin segment, subcutaneous tissue, and galea aponeurotica adjacent to the lesion, to reconstruct the defect.
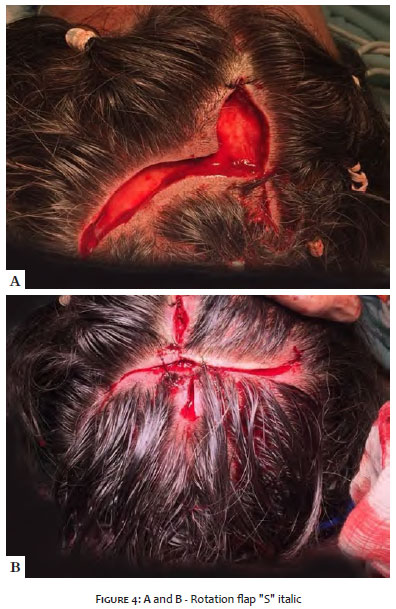
The rotation flap performed was “S” italic or pinwheel scalp flap, in which the adjacent area is detached at the level of the galea aponeurotica in an “S” shape from the lateral margins of the excised area, aiming at the best result to not compromise the hair implantation site and the forehead with a suture scar11 (Figure 4 A and B).
It was possible to close the excised area with minimal local tension and excellent aesthetic results since the entire surgical scar was located on the scalp, and there was no change in the appearance of the face (Figure 5). Also, to minimize the surgical scar, we use the trichophytic suture since, when performing simple sutures on the scalp, there is no hair growth on the suture line. Therefore, the trichophytic suture is a technique that promotes hair growth through the final scar, making it less visible. Initially, the margins are brought closer together by suturing the subcutaneous tissue with absorbable thread (Vycril 3.0) every 2 cm. Then, the epidermis and the superficial dermis of one of the edges are removed using a scissor or a scalpel (a thin epithelium strip of 1.0 mm to 1.5 mm is removed). Finally, the margins are closed with a continuous suture.
This technique places the upper edge of the lesion on the deep bottom edge. Thus, the hair follicles located below the de-epithelialized border will normally grow through the future scar, allowing its camouflage.12,13,14
Wilkins first described osteoma cutis in 1858. It corresponds to a rare and benign dermatosis, characterized by the presence of mature, compact, or spongy bone tissue in the dermis and/or hypodermis.15 It occurs at any age, sex, or race. Also, family occurrences suggest associated genetic factors.7 Pathogenesis is inconclusive. There are two theories regarding the possible tumor origin: the first and most accepted is based on local metaplasia of mesenchymal cells, from fibroblasts to osteoblasts. The second theory supports the abnormal migration of osteoblasts to the skin due to an embryological disorder.4,7,16
Osteoma cutis treatment varies according to location, clinical manifestation, and size and must be individualized in each case. Surgical excision is the treatment of choice, but other therapeutic options are described, such as punch excision, excision and curettage, dermabrasion, topical tretinoin 0.05%, Erbium: YAG laser as an epidermal ablative, CO2 laser, and trichloroacetic acid 100% on the lesions to promote transepidermal elimination of the osteoma.4,7,17,18
In the case presented, we opted for surgical excision due to the size of the lesion located on the scalp. Scalp lesions are a challenge for reconstruction due to the low mobility of the region’s skin, among other factors, making it difficult to close lesions of medium to large extent. The choice for the rotating flap “S” italic aimed to reconstruct the surgical resection defect targeting a better functional and aesthetic result with minimal morbidity to the donor area.
In addition, the suture technique used, known as trichophytic suture, to optimize the result further since it enables the hair growth through the scar, making it less visible.
The treatment performed was successful due to the complete removal of the tumor, the aesthetic results, and the recurrence absence.
Lívia Arroyo Trídico | 0000-0002-7743-4195
Preparation and writing of the manuscript; critical literature review; critical revision of the manuscript.
Paulo Henrique Miranda Ribeiro | 0000-0002-1430-5521
Active participation in research orientation; intellectual participation in propaedeutic and/or therapeutic conduct of studied cases; critical revision of the manuscript.
1. Sánchez MEG, Martínez MLM, Mena JLA, Martín LIDO. Osteoma cutis: rare painful tumor in atypical location. An Bras Dermatol. 2017;92(5 Suppl 1):113-4.
2. Mast AM, Hansen R. Multiple papules on the elbows. Congenital osteoma cutis. Arch Dermatol. 1997;133(6):777-80.
3. Moritz DL, Elewski B. Pigmented postacne osteoma cutis in a patient treated with minocycline: report and review of the literature. J Am Acad Dermatol. 1991;24(5 Pt 2):851-3.
4. Ayaviri NA, Nahas FX, Barbosa MV, Farah AB, Arimatéia Mendes J, Ferreira LM. Isolated primary osteoma cutis of the head: case report. Can J Plast Surg. 2006;14(1):33-6.
5. Boschert MT, Puckett CL. Osteoma cutis of the hand. Plast Reconstr Surg. 2000;105(3):1017-8.
6. Goldminz D, Greenberg RD. Multiple miliary osteoma cutis. J Am Acad Dermatol. 1991;24(5 Pt 2):878-81.
7. Duarte IG. Multiple injuries of osteoma skin in the face: therapeutical least invasive in patients with acne sequela - case report. An Bras Dermatol. 2010;85(5):695-8.
8. Goldminz D, Greenberg RD. Multiple miliary osteoma cútis. J Am Acad Dermatol. 1991;24(5):878-81.
9. Bowman PH, Lesher JL Jr. Primary multiple miliary osteoma cutis and exogenous ochronosis. Cutis. 2001;68(2):103-6.
10. Altman JF, Nehal KS, Busam K, Halpern AC. Treatment of primary miliary osteoma cutis incision, curettage, and primary closure. J Am Acad Dermatol. 2001;44(1):96-9.
11. Souza CD. Reconstruction of large scalp and forehead defects following tumor resection: personal strategy and experience - analysis of 25 cases. Rev Bras Cir Plást. 2012;27(2):227-37.
12. Nirmal B, Somiah S, Sacchidanand SA. A study of donor area in follicular unit hair transplantation. J Cutan Aesthet Surg. 2013;6(4):210-3.
13. Marzola M. Trichophytic closure of the donor area. Hair Transplant Forum Int. 2005;15(4):113-6.
14. Antonio AM, Soares RO. Sutura tricofítica. Revista SPDV. 2017;75(3):273-5.
15. Berbert ALCV, Mantese SAO, Hiraki KRN, Loyola AM, Queiroz NP. Multiple cutaneous miliary osteomas of the face: a case report. Surg Cosmet Dermatol 2012;4(4):360-3.
16. Burgdorf W, Nasemann T. Cutaneous osteomas: a clinical and histopathologic review. Arch Dermatol Res. 1977;260(2):121-35.
17. Wu M, Wang Y, Zhang D, Jia G, Bu W, Fang F, Zhao L. A case of giant primaryosteoma cutis successfully treated with tissue expansion and surgical excision. Indian J Dermatol Venereol. 2011;77(1):79-81.
18. Fazeli P, Harvell J, Jacobs MB. Osteoma cutis (cutaneous ossification). West J Med. 1999;171(4):243-45.
 All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773
All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773



 Read in Portuguese
Read in Portuguese
 Portuguese PDF
Portuguese PDF
 Print
Print
 Send this article by email
Send this article by email
 How to cite this article
How to cite this article
 Submit a comment
Submit a comment
 Mendeley
Mendeley
 Pocket
Pocket
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}