


Thais Feres Moreira Lima; Mariana das Neves Melo; Lisa Gava Baeninger; Antonio Gomes Neto; André Luiz Simião
Received on: 29/09/2020
Approved on: 04/03/2021
Financial support: None
Conflict of interest: None
Study conducted at the PUC Campinas (SP) Hospital, Brazil
Nevus sebaceous of Jadassohn is a congenital skin hamartoma often located on the face and scalp. A small percentage of these tumors evolve into malignant lesions, including basal cell carcinoma. We report a case of an elderly patient with nevus sebaceous since early childhood that evolved with a malignant transformation from the lesion to basal cell carcinoma. The treatment performed was surgical excision using Mohs surgery.
Keywords: Nevus, Sebaceous of Jadassohn; Carcinoma, Basal Cell; Mohs Surgery
Nevus sebaceous is a benign skin tumor composed of numerous malformed sebaceous glands, degenerated hair follicles, and ectopic apocrine glands. It is located mainly on the scalp and face. Two-thirds of lesions are present since birth, and one-third develop in early childhood.1 The most common complication of nevus sebaceous is its transformation into other tumors, benign or malignant. Among the malignant ones, the most common is basal cell carcinoma, which occurs in less than 1% of cases.2 This is a case report of nevus sebaceous with malignant transformation to basal cell carcinoma, treated with Mohs micrographic surgery.
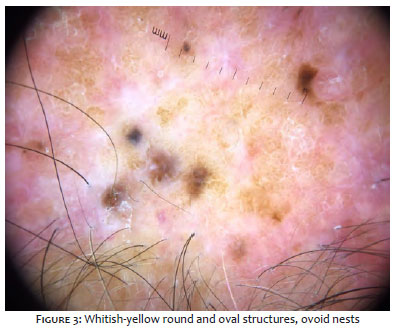
A 68-year-old man, Caucasian, presented a brownish-yellow plaque of approximately 5 cm on the scalp, with a warty appearance (Figure 1). The patient reported having the lesion since childhood but that it had been growing and changing texture over the years. Dermoscopy revealed round and yellow-white oval structures in cobblestones (Figures 2 and 3), ovoid nests, maple leaf-like areas, and diffuse erythema. An incisional biopsy of the lesion, guided by dermoscopy, was performed at three points for suspected malignancy.
Anatomopathology showed two fragments compatible with solid extensive basal cell carcinoma and one with solid infiltrative basal cell carcinoma. Mohs micrographic surgery was indicated to excise the lesion. The surgical margins of the first stage were considered free of neoplasia, with nine lateral and three deep fragments (Figures 4 and 5). We opted for the primary closure of the lesion (Figures 6 and 7).
The lesion’s rapid growth and ulceration may indicate it.
In histology, the presence of immature hair follicles is characteristic. The sebaceous glands are few and underdeveloped in childhood. After puberty, acanthosis and papillomatosis are observed in varying degrees, in addition to abundant hyperplastic sebaceous glands. Furthermore, several lesions have ectopic apocrine glands.5 The diagnosis is clinical-histopathological.
The most common complication of sebaceous nevus is its transformation into other tumors, benign or malignant. Among benign tumors, the most frequent are syringocystadenoma papilliferum and trichoblastoma.4,5 Among the malignant ones, the most commonly associated with nevus sebaceous is basal cell carcinoma, being observed in less than 1% of cases.2 The risk of malignant transformation increases with age, but the literature reports cases in children.6 The etiology of basal cell carcinoma in nevus sebaceous is not yet well established. Studies suggest a link to the human papillomavirus (HPV). This virus would cause a modification in cell proteins, changing their function and expression.7 Another risk factor associated with basal cell carcinoma development in organoid nevus is light skin phototypes (Fitzpatrick I and II).
The rapid lesion growth and the appearance of pigmentation or ulceration areas should raise the suspicion of malignant transformation. Most malignant tumors developed from a sebaceous nevus are not very aggressive.8 Reports of higher aggressiveness are associated with squamous cell carcinoma.9 The definitive treatment for nevus sebaceous is surgical excision. Some authors indicate the lesion removal in childhood, as it prevents its malignant transformation.10 However, surgery in children sometimes requires general anesthesia, which can have essential complications due to the age group.11 Other authors recommend periodic observation of the lesion and suggest surgery if malignancy is suspected or, for aesthetic purposes, after puberty.12 Injuries on the scalp can be challenging to follow clinically due to the location. Alternatives to surgery are photodynamic therapy, dermabrasion, and laser.13 However, these treatments do not completely remove the lesion, and the risk of secondary neoplasia and recurrence remains.
Nevus sebaceous, also known as sebaceous nevus of Jadassohn’s and organoid nevus, is a congenital skin hamartoma. Its incidence is estimated in 0.3% of live births, with no preference for sex.1,2 Its etiology is not very well defined; some recent studies have found an association with a mosaic mutation in the HRAS and KRAS genes.3
Nevus sebaceous is a benign tumor that includes sebaceous, follicular, and apocrine elements. It is most commonly located on the scalp and face. On the scalp, it is usually associated with local alopecia. It appears as a flat yellow-orange lesion that can be oval, round, or in a linear plaque in childhood. In puberty, under hormonal influence, the lesion tends to develop a warty or nodular surface. There is also a trend towards linearity. Over the years, some lesions may evolve with the appearance of tumors and/or with malignancy under the original nevus.4
Scalp surgery, regardless of age, is challenging because of the convex surface of the skull, the presence of hair, and the little looseness of the tissue. Mohs micrographic surgery is a surgical technique that removes the lesion and conducts the histological evaluation concurrently.14 The fragments are removed and assessed. Finding neoplastic cells in any component leads to a new phase of resection until the margins are free. Thus, this technique removes the least amount of healthy skin possible and is an excellent tool for scalp injuries.15 In the reported case, the primary closure of the lesion was possible, with aesthetically satisfactory results (Figure 7). Although the risk of malignancy is higher in adulthood, we believe that strict clinical follow-up in childhood and adolescence and early surgical excision are beneficial in the management of nevus sebaceous.
Thais Feres Moreira Lima | 0000-0002-3170-9034
Approval of the final version of the manuscript; study design and planning; preparation and writing of the manuscript; data collection, analysis, and interpretation; critical literature review; critical revision of the manuscript.
Mariana das Neves Melo | 0000-0003-1746-9828
Approval of the final version of the manuscript; study design and planning; intellectual participation in propaedeutic and/or therapeutic conduct of studied cases; critical revision of the manuscript.
Lisa Gava Baeninger | 0000-0002-3930-5827
Approval of the final version of the manuscript; study design and planning; intellectual participation in propaedeutic and/or therapeutic conduct of studied cases; critical revision of the manuscript.
Antonio Gomes Neto | 0000-0003-2349-1351
Approval of the final version of the manuscript; study design and planning; active participation in research orientation; intellectual participation in propaedeutic and/or therapeutic conduct of studied cases; critical revision of the manuscript.
André Luiz Simião | 0000-0002-0246-2001
Approval of the final version of the manuscript; study design and planning; preparation and writing of the manuscript; active participation in research orientation; intellectual participation in propaedeutic and/or therapeutic conduct of studied cases; critical revision of the manuscript.
1. Constant E, Davis DG. The premalignant nature of the sebaceous nevus of Jadassohn. Plast reconstr surg. 1972;50(3)257-9.
2. Cribier B, Scrivener Y, Grosshans E. Tumors arising in nevus sebaceous: a study of 596 cases. J Am Acad Dermatol. 2000;42:263.
3. Groesser L, Herschberger E, Ruetten A, et al. Postzygotic HRAS and KRAS mutations cause nevus sebaceous and Schimmelpenning syndrome. Nat Genet. 2012;44:783.
4. Moody MN, Landau JM, Goldberg LH. Nevus sebaceous revisited. Ped Dermatol. 2012;29(1):15-23.
5. Simi CM, Rajalakshmi T, Correa M. Clinicopathologic analysis of 21 cases of nevus sebaceus: a retrospective study. Indian J Dermatol Venereol Leprol. 2008;74:625.
6. Goldstein GD, Whitaker DC, Argenyi ZB, Bardach J. Basal cell carcinoma arising in a sebaceous nevus during childhood. J Am Acad Dermatol.1988;18:429-30.
7. Paninson B, Trope BM, Moschini JC, Jeunon-Sousa MA, Ramos-e-Silva M. Basal cell carcinoma on a nevus sebaceous of Jadassohn: a case report. J Clin Aesthet Dermatol. 2019;12(3):40-3.
8. Rosen H, Schmidt B, Lam HP, Meara JG, Labow BI. Management of nevus sebaceous and the risk of basal cell carcinoma: na 18-year review. Ped Dermatol. 2009;26(6):676-81.
9. Arshad AR, Azman WS, Kreetharan A. Solitary sebaceous nevus of Jadassohn complicated by squamous cell carcinoma and basal cell carcinoma.Head Neck. 2008;30(4):544-8.
10. Kong SH, Han SH, Kim JH, et al. Optimal timing for surgical exccision of nevus sebaceous on the scalp: a single-center experience. Dermatol Surg. 2020;46:20.
11. Cunningham BB, Gigler V, Wang L, et al. General anestesia for pediatric dermatologic procedures: risks and complications. Arch Dermatol. 2005;141:573-6.
12. Sanchez ABA, Leal FZ, Vergara RFC, Osuna AKP. Nevo sebáceo de Jadassohn asociado con carcinoma basocelular. Dermatol ver mex. 2014;58:295-9.
13. Rodrigues TNA, Galvão LEG, Gonçalves HS, Pontes MAA. Basal cell carcinoma growth over a nevus sebaceous: treatment of the field cancerization with photodynamic therapy. Surg Cosmet Dermatol. 2017;9(1):100-3.
14. Swanson NA, Grekin RC, Baker SR. Mohs surgery: techniques, indications, and applications in head and neck surgery. Head Neck. 1983;6(2):683-92.
15. Leibovitch I, Huilgol SC, Richards S, Paver R, Franzco DS. Scalp tumors treated with Mohs micrographic surgery: clinical features and surgical outcome. Dermatol Surg. 2006;32(11):1369-74.
 All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773
All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773



 Read in Portuguese
Read in Portuguese
 Portuguese PDF
Portuguese PDF
 Print
Print
 Send this article by email
Send this article by email
 How to cite this article
How to cite this article
 Submit a comment
Submit a comment
 Mendeley
Mendeley
 Pocket
Pocket
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}