


Miguel Vieira Paschoal1; Nadjila Gabriela Santana Sidani2; Renato Santos de Oliveira Filho3; Heitor Francisco Carvalho Gomes3; Gisele Gargantini Rezze4; Francisco Macedo Paschoal4
Received on: 31/08/2020
Approved on: 04/03/2021
Financial support: None
Conflict of interest: None
Acknowledgments: thank my father, friend and now publishing partner, Dr. Francisco Macedo Paschoal, for the support and the opportunity to write this case report with me
Study conducted at the Dermaimage Médicos Associados, São Paulo (SP), Brazil
The recurrent squamous cell carcinoma (SCC) needs an appropriate approach to decrease the risk of recurrences. We report the case of a man diagnosed with SCC on the left temporal region treated by conventional surgery, with infiltration and erythema in the scar area. Reflectance confocal microscopy suggested the diagnosis of recurrent SCC confirmed by histopathology. New surgery and traditional intraoperative frozen section were performed. After two months, the patient had a new relapse, finally treated with Micrographic surgery without new involvement. This article highlights the importance of micrographic surgery in treating SCC, aiming to decrease new recurrences.
Keywords: Skin Neoplasms; Mohs Surgery; Carcinoma, Squamous Cell
Squamous cell carcinoma (SCC) is a keratinocytic neoplasm, which is part of the group of non-melanoma skin cancer. It represents about 20% of cutaneous malignancies, has an invasive character, and can produce metastases. It arises mainly in regions exposed to the sun and can originate from precursor lesions.1
The estimated incidence of non-melanoma skin cancer in Brazil in 2016 was 81.66 cases in men and 91.98 cases in women per 100 thousand inhabitants.2 Among the risk factors for the development of the disease stand out exposure to sunlight, age, fair skin, in addition to family and personal history of skin cancer.3
The lesions can manifest as shallow ulcers, papules and/or nodules, scaly, itchy macules, or wounds that have not healed for more than four weeks. The limits of the lesion may be indistinguishable from the skin surrounding the actinic damage.2, 4
SCC diagnosis is histopathological, made from tumor samples obtained by biopsy. Needle aspiration is indicated in regional lymph nodes if they are palpable. Contrast-enhanced magnetic resonance imaging should be used when there is a suspicion of bone, lymphatic, perineural, or vascular tissue involvement.3
Treatment is conducted according to the characteristics of the primary lesion. Curettage and electrocoagulation in non-hairy areas, excision of the tumor with margins of 4 mm to 6 mm, and radiotherapy in patients with surgical contraindication are indicated in cases of low-risk SCC. For high-risk SCC, excision with wide margins and reconstruction, Mohs micrographic surgery or methods of peripheral analysis of surgical margins, and radiotherapy for patients with surgical contraindication are recommended. The persistence of tumor residues after the indicated treatments or the impossibility of reaching free margins during micrographic surgery leads to the indication of a multidisciplinary approach, such as chemotherapy or immunotherapy. Sentinel lymph node biopsy should also be considered. Follow-up should be performed every three to 12 months for two years, every six to 12 months for three years, and then once a year.3
Considering the increasing incidence and implications of SCC, its appropriate approach is essential, valuing a therapeutic choice that allows the maximum eradication of the tumor and minimizes the risk of recurrence.
In this scenario, the authors report the case of a patient with squamous cell carcinoma with two relapses treated with micrographic surgery.
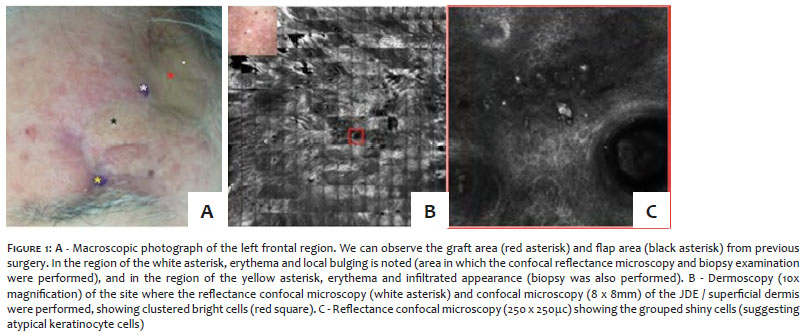
A 67-year-old white man presented an infiltrated plaque with imprecise limits located in the left frontal region close to the surgical scar. The patient presented a history of surgical excision in the left forehead region four months ago, preceded by biopsy. The anatomopathology revealed SCC grade 3, poorly differentiated, with edges larger than 4 mm, infiltrating the fat tissue. After four months, he noticed a bulging in the scar region and sought specialized care to perform confocal microscopy. Physical examination showed left forehead with a graft area and a 1 cm diameter bulging in the middle of the surgical scar, hardened and adhered to deep planes (Figure 1), and an area of intense erythema, adhered to deep planes in the left suprapalpebral region (Figure 1). Confocal microscopy revealed the presence of an atypical honeycomb pattern throughout the epidermis and suprabasal region, and large shiny round cells at the dermal-epidermal junction (DEJ) and papillary dermis. Large and grouped round brilliant cells, thick collagen, and great vessels were also present, suggesting a diagnosis of atypical keratinocytes lesion and probable recurrence of squamous cell carcinoma (Figure 1).
Two incisional biopsies were performed in the areas described. The anatomopathological result showed infiltration of moderately differentiated squamous cell carcinoma in the skin of the left frontal region and dermal fibrosis on the scarring skin of the left supraorbital area. Before the first surgery, magnetic resonance imaging was performed, ruling out the hypothesis of perineural and skullcap infiltration. The patient underwent surgical removal with conventional intraoperative freezing, with free margins. After two months, the patient presented a new suspicious area, and a new incisional biopsy was performed. The anatomopathological result was poorly differentiated carcinoma infiltrating subcutaneous tissue and surgical margins coinciding with the neoplasm. Giving the new relapse, we chose treatment with micrographic surgery. The excision was performed at 90º to check the lateral edges with higher accuracy.
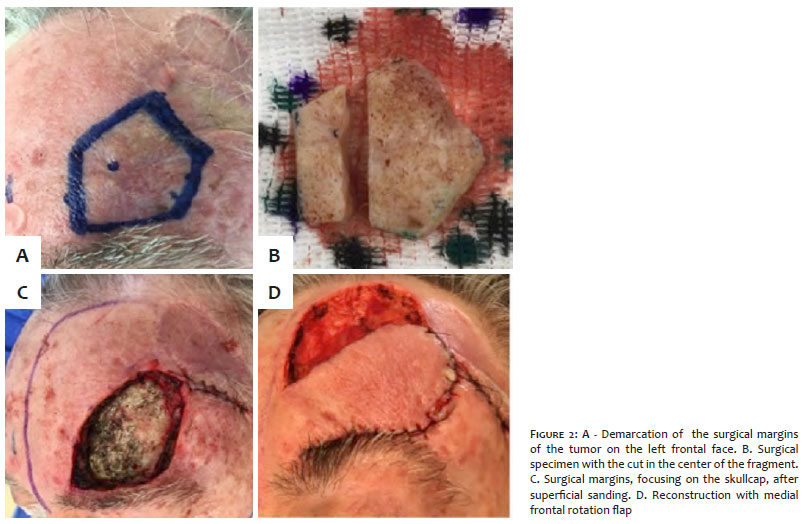
A central fragment of the surgical specimen was cut through the tumor to assess the involvement of the deep margin. It evidenced the presence of tumor infiltration up to the periosteum. The peripheral surgical margins (superficial and deep) were free of neoplasia. Due to the periosteum involvement, we conducted the superficial abrasion of the skullcap to ensure better safety regarding the deep margins, removing possible remaining tumor foci. We performed the reconstruction using a median frontal rotation flap, nourished by the supratrochlear artery (Figure 2), with the donor area healing by secondary intention (Figure 2). The surgical oncology team is still following the patient, who hasn’t show any recurrence (Figure 3). No radiotherapy was performed.
Risk factors for tumor recurrence are location, size, immunosuppression, tumor differentiation degree, tumor depth, and/or perineural, lymphatic, or vascular involvement, making the appropriate therapeutic choice essential.3
Micrographic surgery is one of the first lines therapies to treat recurrent and high-risk tumors. It is also recommended for any tumor in more exposed areas. Its implementation allows intraoperative evaluation of the compromised margins, reducing the risk of recurrence to 3.1% in the treatment of the primary tumors, and to 5.9% in recurrences.3
The micrographic surgery technique can be summarized in five parts: the first is the topographic marking of the tumor and its margins, followed by excision in the shape of a basin at 45º. Then, three dimensions slides are made to recognize the lateral, deep, and superficial margins of the lesion, analyzing whether these margins are compromised or not. If the margins are compromised, the tumor is further excised until the margins are free.5
The diagnosis is based on the history of the lesion development, clinical examination, and histopathological analysis. Reflectance confocal microscopy (RCM) is an essential tool, helping with clinical diagnosis. Possible differential diagnoses are basal cell carcinoma, keratoacanthomas, and actinic keratosis, which must be ruled out through biopsy in the presence of a clinical lesion indicative of SCC.1,2, 3
The main advantage of the chosen treatment is the reduced risk of recurrences and metastases. The fact that they are invasive approaches is the main disadvantage, both in the diagnostic and therapeutic methods.
This report highlights the importance of performing a peripheral analysis of the surgical margins (Mohs micrographic surgery or other methods) in the first local recurrence and in patients with high-risk carcinomas, thus decreasing the number of surgeries.
Micrographic surgery has a high success rate and minimizes the risk of tumor recurrence, allowing most patients to undergo a single surgery. It reduces or eliminates the costs of more complex surgeries and mitigates the psychological impact in treating the disease.
Miguel Vieira Paschoal | 0000-0002-6834-1245
Statistical analysis; approval of the final version of the manuscript; study design and planning; preparation and writing of the manuscript; data collection, analysis, and interpretation; active participation in research orientation; intellectual participation in propaedeutic and/or therapeutic conduct of studied cases; critical literature review; critical revision of the manuscript.
Nadjila Gabriela Santana Sidani | 0000-0002-3431-5356
Statistical analysis; approval of the final version of the manuscript; study design and planning; preparation and writing of the manuscript; data collection, analysis, and interpretation; active participation in research orientation; intellectual participation in propaedeutic and/or therapeutic conduct of studied cases; critical literature review; critical revision of the manuscript.
Renato Santos de Oliveira Filho | 0000-0002-7464-973X
Data collection, analysis, and interpretation; intellectual participation in propaedeutic and/or therapeutic conduct of studied cases.
Heitor Francisco Carvalho Gomes | 0000-0002-1464-673X
Data collection, analysis, and interpretation; intellectual participation in propaedeutic and/or therapeutic conduct of studied cases.
Gisele Gargantini Rezze | 0000-0001-90844634
Data collection, analysis, and interpretation; active participation in research orientation; intellectual participation in propaedeutic and/or therapeutic conduct of studied cases.
Francisco Macedo Paschoal | 0000-0002-6264-1538
Approval of the final version of the manuscript; study design and planning; preparation and writing of the manuscript; active participation in research orientation; intellectual participation in propaedeutic and/or therapeutic conduct of studied cases; critical revision of the manuscript.
1. Dornelas MT, Rodrigues MF, Machado DC, Gollner AM, Ferreira AP. Expressão de marcadores de proliferação celular e apoptose no carcinoma espinocelular de pele e ceratose actínica. An Bras Dermatol. 2009;84(5):469-75.
2. Inca. Monitoramento das ações de controle do câncer pele. Available from: http://www1.inca.gov.br/inca/Arquivos/inform.deteccaoprecoce.pdf - Accessed 18/04/2020.
3. Nccn. Squamous cell skin cancer Version 1. 2016. Available from: https://www.nlm.nih.gov/medlineplus/ency/article/000829.htm - Accessed 18/04/2020.
4. LeBoit PE, Burg G, Weedon D, et al. World Health Organization classification of tumors: pathology and genetics of skin tumors. 3rd ed. Lyon: IARC Press; 2006.
5. Moehrle M, Breuninger H, Röcken MA. Confusing world: what to call histology of three-dimensional tumour margins? J Eur Acad Dermatol Venereol. 2007;21(5):591-5.
 All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773
All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773



 Read in Portuguese
Read in Portuguese
 Portuguese PDF
Portuguese PDF
 Print
Print
 Send this article by email
Send this article by email
 How to cite this article
How to cite this article
 Submit a comment
Submit a comment
 Mendeley
Mendeley
 Pocket
Pocket
{kind=link}
{kind=link}
{kind=link}