


Leonardo Mello Ferreira1; Frederico Hassin Sanchez2; Pamella Paola Bezerra de Oliveira3
Received on: 22/06/2020
Approved on: 04/03/2021
Financial support: None
Conflict of interest: None
Study conducted at the Skin Medicine Center (Centro de Medicina Cutânea – CEMEC), Linhares (ES), Brazil
Basosquamous carcinoma has a high potential for local recurrence and metastasis, especially when it recurs and at the periocular area. A 49-year-old man underwent Mohs micrographic surgery and subtotal reconstruction of the lower eyelid with cartilage graft from the helix of the ear associated with the Tripier flap, evolving with excellent functional and aesthetic results.
Keywords: Basosquamous carcinoma; Eyelid Neoplasms; Mohs surgery; Skin Neoplasms
The eyelids contain numerous histological elements that can be the source of benign and malignant tumors. They are composed of four layers: skin and orbicularis muscle (anterior lamella), tarsus and conjunctiva (posterior lamella). The skin is composed of epidermis, dermis, and its attachments. Among the annexes, we find the eccrine glands (sweat and accessory lacrimal glands of Wolfring and Krause), apocrine glands of Moll, and sebaceous glands (Zeiss and Meibomian). Most tumors in this location have an epidermal origin. In Caucasians, basal cell carcinoma (BCC) is responsible for about 90% of palpable cancers, followed by squamous cell (SCC) and sebaceous carcinomas, responsible for 5% of cases each.1
Basosquamous carcinoma (BSC), or metatypical, clinically indistinguishable from BCC, represents about 2% of non-melanoma skin cancers and can be more aggressive than SCC (local recurrence of up to 45% and distant metastases of 5-10%). It usually occurs in the head and neck of older white men. Histologically, typical areas of BCC and SCC are observed, in addition to a transition zone between them.2,3
Mohs micrographic surgery (MMS) allows complete removal of malignant skin tumors while maximizing the preservation of normal tissue. This technique provides the lowest recurrence rate and postoperative complications in the treatment of skin cancer. MMS success derives from obtaining circumferential intraoperative frozen sections with a complete assessment of the lateral and deep surgical margins. Eyelid tumors are at high risk for recurrence and metastasis, but MMS can minimize it. Complete resection of peri-tumoral tumors is crucial because recurrence can lead to devastating consequences, including loss of eye function, invasion of the skull base, and even death. A complete ophthalmological evaluation is recommended preoperatively. Some signs, such as adherence to deep planes, decreased ocular motility, dystrophy, eyeball displacement, eyelid ptosis and proptosis, suggest better investigation with image exams to establish compression or periorbital invasion. A retrospective study of two centers showed that the overall complication rate after repairing the periorbital defect by Mohs surgeons were equivalent, if not lower, to the complication rates in procedures performed by oculoplastic surgeons.4,5 MMS is the gold standard in BSC treatment.3 About 1/3 of the cases require more than one phase, with approximately 5% of local recurrence.6
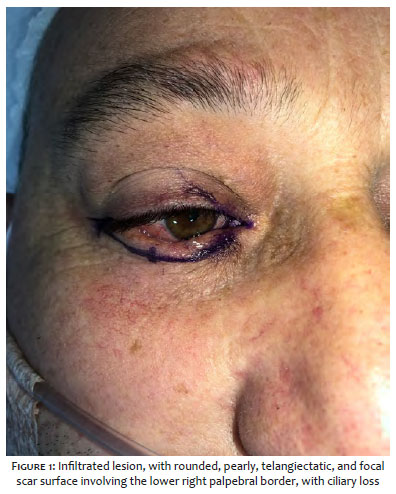
A 49-year-old man, skin phototype II, with no comorbidities, presented a lesion affecting the right lower ciliary border (from the lateral extremity to near the lower lacrimal point). Clinical and dermoscopy exams suggested basal cell carcinoma (Figure 1). The patient reported treatment (unspecified) of a minor lesion in the same site for seven years with an ophthalmologist.
The histopathological examination of a previous incisional biopsy concluded that it was a solid basal cell carcinoma. Surgical treatment using the Mohs technique was proposed, and the patient was submitted to local anesthesia and conscious intraoperative sedation in a hospital surgical center.
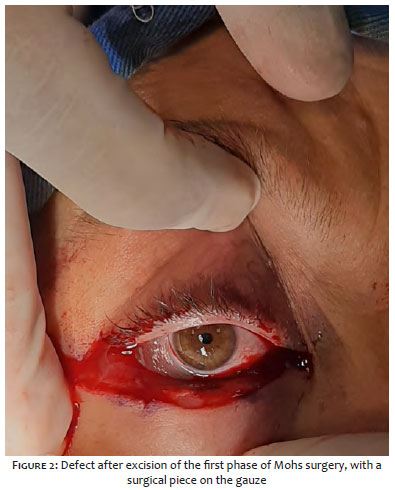
The clinically visible lesion was excised with a margin of more than 2 mm in the first phase (Figure 2). Microscopic examination revealed nodular basal cell carcinoma and poorly differentiated squamous cell carcinoma areas, significantly compromising the resection’s deep margin. The next phase obtained free margins, although with an intense inflammatory infiltrate. Though indicated, a new stage was not performed due to the coincidence of the deep margin with the fornix and the bulbar conjunctiva, making it impossible to enlarge the surgery site without damaging the eyeball (Figure 3).
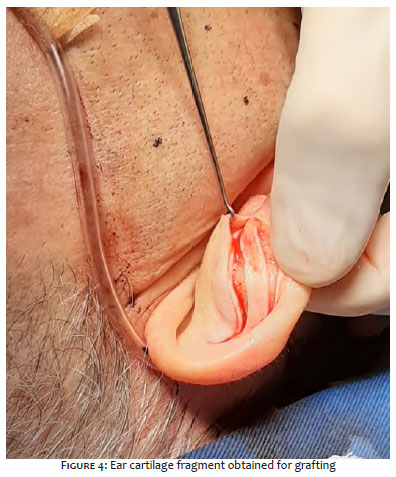
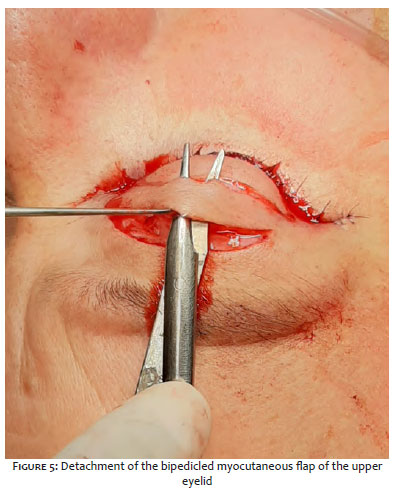
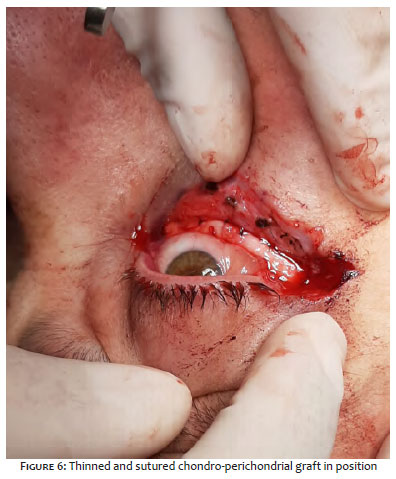
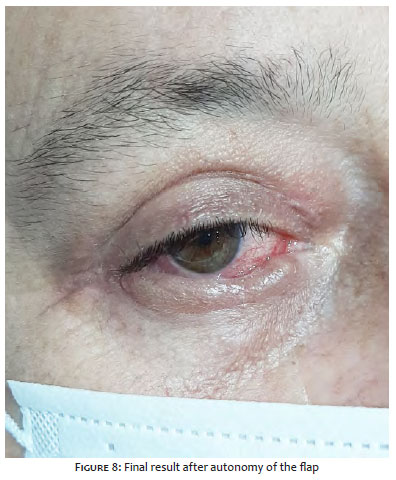
We chose a chondro-perichondrial graft of the ear helix (Figure 4) and a bipedicled myocutaneous flap (Tripier) - from the upper eyelid to the anterior lamella - to reconstruct the posterior lamella, promoting vascular support to the graft (Figure 5). After lateral canthotomy, the graft was sutured in the periosteum of the lateral corner (with 5-0 nylon), in the remnant of the medial tarsus, and the lower eyelid retractor muscle (with 7-0 polypropylene) (Figure 6). The flap was sutured on the upper edge of the graft (with 7-0 polypropylene) and the remaining anterior lamella (with 6.0 nylon, in two layers). The donor area was sutured with 6-0 nylon (Figure 7). After 30 days, the flap reached autonomization (Figure 8).
The conventional paraffin histopathological examination of the residual surgical specimen confirmed the diagnosis of basosquamous or metatypical carcinoma. The patient had an excellent aesthetic and functional result on the reconstructed eyelid, with no complications or abnormal healing of the graft donor area. The patient is undergoing dermatological and ophthalmological follow-up.
The histological criteria and terminology of BSC are still controversial in the literature from a prognostic point of view. However, it is essential to differentiate it from the keratotic basal cell carcinoma, an indolent subtype of BCC that does not present squamous differentiation, only formation of horny cysts surrounded by paraceratotic cells within the atypical basaloid cell blocks.7 The present case reinforces the importance of the Mohs surgeon’s full histopathological knowledge since the previous incisional biopsy showed only a solid BCC.
About 10% of BSCs involve the eyelid region,8 and ocular invasion is reported.9 The dense inflammatory infiltrate present under the microscope of the second phase of MMS raises doubts about the complete removal of the tumor in this case. On the other hand, an additional phase could have meant an unnecessary orbital exenteration. Rapid immunohistochemistry could have helped differentiate between inflammatory and neoplastic infiltrate, but unfortunately, it was not available.10 Clinical and radiological follow-up of the patient is indispensable in this case.
Primary closure can reconstruct full-thickness defects of the lower eyelid when it involves up to 25% of the length of the ciliary border. Between 25% and 50%, lateral canthotomy, lower cantholysis, and even a temporal flap can be associated.
Defects above 50% need reconstruction of the posterior lamella: a periosteal flap can be used for defects involving the lateral third, while the Hughes tarsoconjunctival flap is the best option for central defects.11
An option to reconstruct defects larger than 2/3 of the length of the lower eyelid is combining a graft to restructure the posterior lamella with a flap to restore the anterior lamella. The graft can be harvested from the nasal septum, oral mucosa, or auricular cartilage.12 Matsuo initially described the chondro-perichondrial graft of the ear in 1987, using the auricle (pinna) as the donor area for reconstruction of the posterior lamella. However, Sanchez and Lerner, in 2013, proposed the use of the ear helix as a donor area due to its smaller thickness, the greater malleability of the cartilage, and, consequently, the better adaptation to the eyeball concerning the shell cartilage.13
The Tripier bipedicled upper eyelid flap is indicated to reconstruct defects in the lower eyelid, especially in the middle third. This technique requires a second surgical time to section the lateral pedicles.14 Although other local flaps can be used,15 the Tripier flap, because it is myocutaneous, allows better nutrition of the underlying graft, and provides a superior aesthetic result by using skin from the eyelid region.
MMS is the gold standard to treat malignancies in the eyelid region, including more aggressive tumors such as basosquamous carcinoma. The reconstruction of extensive full-thickness defects of the lower eyelid with the association of chondro-perichondrial graft of the ear helix with the Tripier bipedicled myocutaneous flap presents as a practical and safe option with good functional and aesthetic results.
Leonardo Mello Ferreira | 0000-0002-3427-032X
Study design and planning; preparation and writing of the manuscript; critical literature review.
Frederico Hassin Sanchez | 0000-0001-5856-216X
Intellectual participation in propaedeutic and/or therapeutic conduct of studied cases; critical revision of the manuscript.
Pamella Paola Bezerra de Oliveira | 0000-0002-3429-032X
Data collection, analysis, and interpretation.
1. Pe'er J. Pathology of eyelid tumors. Indian J Ophthalmol. 2016;64(3):177-90.
2. Shukla S, Khachemoune A. Reappraising basosquamous carcinoma: a summary of histologic features, diagnosis, and treatment. Arch Dermatol Res. 2020;312:605-9.
3. Oldbury JW, Wain RAJ, Abas S, Dobson CM, Iyer SS. Basosquamous carcinoma: a single centre clinicopathological evaluation and proposal of an evidence-based protocol. J Skin Cancer. 2018:1-7.
4. Mori WS, Demer AM, Mattox AR, Maher IA. Mohs micrographic surgery at challenging anatomical sites. Dermatol Surg. 2019;45(Suppl 2):S142-S154.
5. Sanchez FH, Lerner E. Manejo dos tumores perioculares com cirurgia micrográfica de Mohs. Surg Cosmet Dermatol. 2014;6(4):330-6.
6. Allen KJ, Capell MA, Killian JM, Brewer JD. Basosquamous carcinoma and metatypical basal cell carcinoma: a review of treatment with Mohs micrographic Surgery. Int J Dermatol. 2014;53:1395-403.
7. Tan CZ, Rieger KE, Sarin KY. Basosquamous carcinoma: controversy, advances, and future directions. Dermatologic Surg. 2017;43(1):23-31.
8. Wermker K, Roknic N, Goessling K, Klein M, Schulze H, Hallermann C. Basosquamous carcinoma of the head and neck: clinical and histologic characteristics and their impact on disease progression. Neoplasia. 2015;17: 301-5.
9. Papadopoulos GO, Charitonidi E, Filippou N, Fanidou D, Filippou D, Scandalakis P. Primary basosquamous carcinoma of the lower eyelid with ocular invasion. A case report. Ann ital Chir. 2018;7: S2239253X18028268
10. Sanchez FH, Marques HS, editors. Cirurgia micrográfica de Mohs. Manual prático e atlas. Rio de Janeiro: Di Livros; 2019.
11. Ozgur O, Rostami S. Lower eyelid reconstruction. [Updated 2020 Feb 11]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2020.
12. Vieira R, Goulão J. Algoritmos para reparo das pálpebras. Surg Cosmet Dermatol. 2019;11(2):91-6.
13. Sanchez FH, Lerner E. Reconstrução palpebral com enxerto condropericondral de hélice de orelha. Experiência de um centro de referência em cirurgia micrográfica de Mohs. Surg Cosmet Dermatol.2013;5(4):324-8.
14. Bickle K, Bennett RG. Tripier flap for medial lower eyelid reconstruction. Dermatol Surg. 2008;34:1545-8.
15. Subramanian N. Reconstructions of eyelid defects. Indian J Plast Surg. 2011;44(1):5-13.
 All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773
All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773



 Read in Portuguese
Read in Portuguese
 Portuguese PDF
Portuguese PDF
 Print
Print
 Send this article by email
Send this article by email
 How to cite this article
How to cite this article
 Submit a comment
Submit a comment
 Mendeley
Mendeley
 Pocket
Pocket
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}