


Manoel Gomes Filho Neto; Solange Cardoso Maciel Silva
Received on: 12/03/2021
Approved on: 16/03/2021
Financial support: None
Conflict of interest: None
Study conducted at the Pedro Ernesto University Hospital of the Universidade Estadual do Rio de Janeiro, Rio de Janeiro (RJ), Brazil
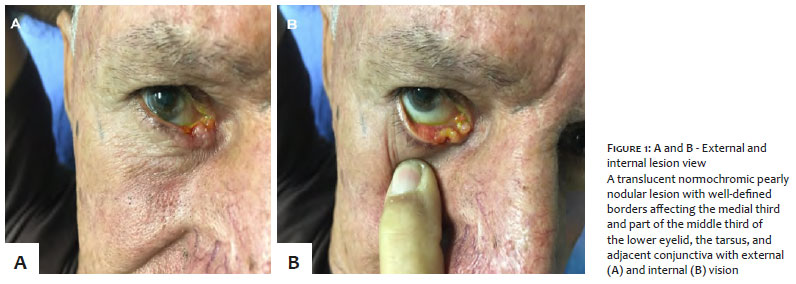
The lower eyelid is one of the sites most affected by basal cell carcinoma (BCC). We present an option of inner corner skin flap with oral mucosa graft for eyelid reconstruction after BCC excision. This tumor affects approximately 60% of the lower eyelid and shows complete lower lacrimal canaliculus involvement. The use of internal corner skin transposition flap and oral mucosa graft is safe. The technique is reproducible and with good postoperative evolution. Positioning and eyelid movement were restored, allowing tear drainage through the upper canaliculus with complete correction of the tears’ overflow (epiphora).
Keywords: Basal cell carcinoma; Skin Neoplasms; Dermatological Surgical Procedures; Surgical Flaps
Eyelids are the preferred site of involvement of 5% to 10% of all skin tumors. Basal cell carcinoma (BCC) is the most prevalent palpebral malignant tumor, followed by epidermoid cancers, sebaceous gland carcinomas, and melanomas.1 BCC primarily affects the lower eyelid, with 70% of prevalence, followed by medial corner 20%, upper eyelid 7%, and lateral corner 3%.1-2
The eyelid skin is the thinnest one of the body, with virtually no subcutaneous tissue. It has an internal conjunctiva lining, which allows eyelid movement with minimal friction. Dense bands of thick connective tissue named tarsus, whose function is to support the eyelids, reinforce them. Three lamellae constitute the lower eyelid: the anterior, consisting of skin and orbicularis muscle; the middle, composed of the orbital septum; and the posterior, comprising the tarsus, palpebral fascia, and conjunctiva. The septum originates in the marginal arc along the orbital border separating the anterior from the posterior lamellae.3-4
The eyelids hold essential functions for the integrity of ocular viability, such as cornea and eyeball mechanical protection, humidification, oxygen, and nutrients transport by tear movement, foreign substances removal, and protection against excessive light.3-4 These functional aspects should be prioritized in a palpebral reconstruction, valuing the aesthetic features. The dermatological surgeon should be aware of the anatomy and physiology of the region for adequate reconstruction programming.
We present the option of a skin flap in the inner corner with an oral mucosa graft for eyelid reconstruction after BCC excision affecting approximately 60% of the lower eyelid and showing the tumor’s complete involvement of the inferior lacrimal canaliculus.
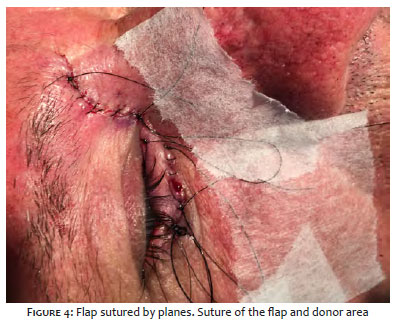
A 68-year-old man reported a lesion on the lower eyelid for about a year, with slow and progressive growth, referring to symptomatic tearing (epiphora). The examination revealed a translucent normochromic nodular lesion with well-defined borders, affecting the proximal third and part of the middle third of the lower eyelid (Figures 1A and 1B). Ophthalmologic evaluation using the Monier fluorescein eye stain test showed involvement and total destruction of the inferior canaliculus. We performed asepsis, antisepsis, lesion marking, and anesthesia with tumescent solution. An incision was made with complete removal of the lesion (with margins of 3 mm to 4 mm, creating a primary surgical defect occupying 60% to 70%) of the lower eyelid (Figure 2). We performed another incision of skin and subcutaneous cellular tissue and part of the orbicularis muscle of the inner corner of the eye to make the transposition flap. In the same operative act, the cheek mucosa was incised and sutured on the internal surface of the musculocutaneous flap. Laterality was used to fill the area of the surgical defect (Figure 3), with the flap positioned and sutured by planes (Figure 4).
The treatment goal of malignant tumors is complete surgical excision of the tumor. Surgical reconstruction of large eyelid defects is a complex process that relies on the extent of tissue loss, location, and experience of the surgeon. Full-thickness eyelid defects are divided into small (margin involvement less than one-third of the eyelid size); moderate (involvement between one-third and one-half of the eyelid); and large (margin involvement more extensive than half of the eyelid size). The direct primary closure of the eyelid is a possible option in defects of total thickness up to one-third of its horizontal extension. However, major defects require the reconstruction with cutaneous flaps associated or not with grafts. The literature describes several options: advancement; Transposition; Mustardé and Mcgregor; Fricke,2 Landolt-Hughes, Dutupuys-DutempsHughes, and interpolation (utilizes skin and mucosa from the upper eyelid); Abbe.5
The cartilage graft is usually indicated for defects occupying more than 50% of the lower eyelid or total palpebral resections. However, in our case, we believe that an exact musculocutaneous flap for the filled region with perfect coaptation of the palpebral margins would be sufficient for the ideal functioning of the superior lacrimal duct. It would also correct the epiphora presented by the patient. The graft of the oral mucosa has the function of replacing the posterior lamellae in the palpebral reconstruction. In this case, we chose the cheek over the palate mucosa because it is easier to access and has a lower complication rate when compared to a palate graft, whose hemorrhage and oronasal fistulas are feared complications.4
Surgical excision is considered the most effective therapy for basal cell carcinomas, with cure rates ranging between 95% and 98%. In our case, the tumor was well delimited, which facilitated the surgical removal. The material was sent to histopathology, confirming the complete removal of the tumor.6 Also, removing the lesion in a block and assessing the lateral margins eased the pathology.
Using skin transposition flap from the inner corner and oral mucosa graft is safe, with little morbidity in the donor area, resulting in maintenance of functionality and preservation of the aesthetic aspect, with rapid postoperative recovery. We present a reproducible technique capable of restoring the eyelid anatomy (Figure 5), with good postoperative evolution, with no ectropion, retraction, or anatomical distortions. Eyelid positioning and movement were restored, as well as the perfect occlusion of the eyelid cleft, allowing the drainage of the tear through the superior canaliculus with complete correction of tearing (epiphora).
Manoel Gomes Filho Neto | 0000-0003-1278-8758
Approval of the final version of the manuscript; study design and planning; preparation and writing of the manuscript; data collection, analysis, and interpretation; active participation in research orientation; intellectual participation in propaedeutic and/or therapeutic conduct of studied cases; critical literature review; critical revision of the manuscript.
Solange Cardoso Maciel Silva | 0000-0003-0812-908X
Intellectual participation in propaedeutic and/or therapeutic conduct of studied cases.
1. Cook Jr BE, Bartley GB. Epidemiologic characteristics and clinical course of patients with malignant eyelid tumors in an incidence cohort in Olmsted County, Min Ophthalmol. 1999;106(4):746-50.
2. Herzog Neto G, Sebastiá R, Viana GAP, Machado F. Reconstrução palpebral com retalho de Fricke: relato de dois casos. Arq. Bras. Oftalmol. 2006;69(1):123-6.
3. Chedid R, Borges KS, Santos P, Sbalchiero JC, Dibe MA, Leal PR, et al. Perfil das reconstruções de palpebral inferior no Instituto Nacional do Câncer: estudo retrospectivo de 137 casos. Rev. Bras. Cir. Plást. 2010;25(3):22.
4. Fernandes JB, Dias V, Nunes TP, Matayoshi S, Moura E. Enxerto de mucosa do palato duro: complicações na área doadora - Relato de casos. Arq. Bras. Oftalmol. 2003;66(6):884-6.
5. Benez MDV, Sforza D, Mann D, Silva SCM. Reconstrução de pálpebra inferior com retalho cutâneo e enxerto de mucosa oral. Surg Cosm Dermatol. 2014;6(2):178-82.
6. Arias SJC, Abreu PFA, Ortiz SM, Despaigne DJ, Matienzo VSC. Reconstrucción palpebral inferior después de la escisión de tumores malignos. MediSan. 2013;17(07):2053-8.
 All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773
All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773



 Read in Portuguese
Read in Portuguese
 Portuguese PDF
Portuguese PDF
 Print
Print
 Send this article by email
Send this article by email
 How to cite this article
How to cite this article
 Submit a comment
Submit a comment
 Mendeley
Mendeley
 Pocket
Pocket
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}