


Frederico Hassin Sanchez1,2
Received on: 01/03/2020
Approved on: 04/03/2021
Financial support: None
Conflict of interest: None
Study conducted at the Micrographic Surgery Center of Rio de Janeiro, Rio de Janeiro (RJ), Brazil
The tissue processing in Mohs surgery aims at histological slides that allow the analysis of 100% of the surgical margins. The embedding tissue is a critical step and prone to errors. As there is no standardization when mounting the blocks, there may be unevenness in the different samples cutting surfaces, leading to the need for continuous adjustments on the X-Y axis inside the cryostat, slowing down the process. A device was developed to solve this problem, minimizing any blocks inclination, keeping the surgical margins parallel in all samples, accelerating the process, and maintaining the histological slides high quality.
Keywords: Mohs micrographic surgery; Laboratory equipment; Histology; Tissue embedding; Innovation
Mohs micrographic surgery is a thorough technique composed of different steps, making very high-quality histological slides, favoring a great histological control of the surgical margins.
Although minor modifications aimed at optimizing tissue processing have already been described, the concept of the original Mohs technique remains the same until today.1 The surgeon needs to remove the tissue, to allow all peripheral margins to be flattened on a plane surface, making possible the histological analysis of 100% of the surgical margins.1,2 Thus, tissue excision is performed with the scalpel blade making a 45 degrees angle in relation to the skin surface, facilitating the inclination of the lateral tissue edges, allowing all margins to be relaxed and positioned in the same plane.3 After this step, the block is successively assembled for tissue embedding, microtomy, staining, histological slide assembly, and microscopic analysis.
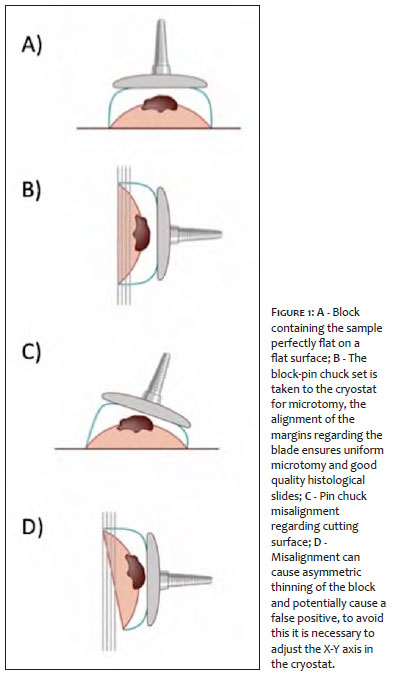
Tissue embedding is technically dependent, corresponding to tissue freezing and block assembly, which co-occur. Usually, the tissue is flattened on a glass slide, and then a freezing gel is placed on the tissue that starts to freeze. A freezing pin chuck is positioned on the set manually. The gel serves as a “glue” joining the pin chuck to the tissue. It also solidifies into a single block, providing the necessary rigidity so that the surface containing the surgical margins (cut surface) can be sectioned uniformly in the cryostat (Figure 1 AB). Tissue inclusion aims to allow the microtomy of the cut surface uniformly inside the cryostat.3
Tissue embedding is a thorough and error-prone step, with three especially critical points: 1) Ability to keep the surgical margins uniformly flat, because if part of the tissue is lifted, it will not be visualized on the histological slide; 2) Capacity to keep the cut surface parallel to the pin chuck’s surface, because when manually positioning the pin, small angles can cause misalignments and the block can be thinned asymmetrically, potentially causing a false positive (Figure 1 C, D). The correction of such misalignment requires adjustments to the X-Y axis in the cryostat, increasing the time spent on the procedure. Such a problem is critical when processing multiple samples. The lack of standardization in the assembly of the blocks requires adjustments between each processed block; 3) Capability to allow rapid freezing since slowing the freezing causes undesirable histological artifacts.2,3
To minimize histotechnical errors and optimize tissue processing, the device in question, called SmartMohs®, was developed and patented.
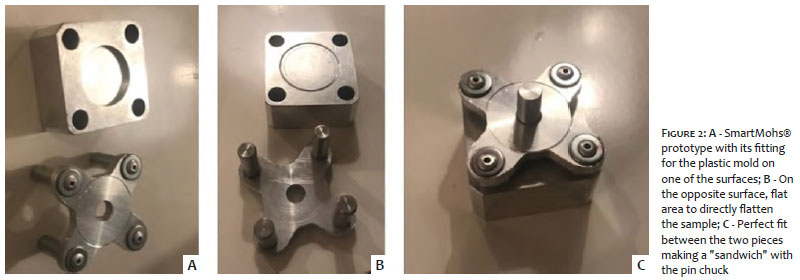
The device consists of two metal parts, a block with a flat surface and an opposite surface containing a circular depression for fitting a plastic mold. There are also four holes for the second metal part to fit perfectly with the first. There is a central hole in this second cross-shaped piece where the pin chuck fits (Figure 2 A-C). As aluminum has an excellent thermal capacity, the temperature remains low even outside the cryostat, allowing the block to be assembled outside the cryostat. The device can work in three different ways according to the operator’s preference or the characteristics of the tissue sample to be included:
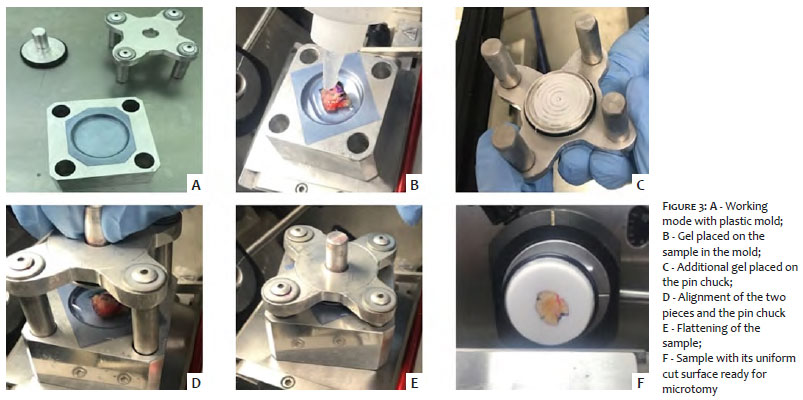
The tissue is flattened directly on the flat surface of a specific, circular, transparent plastic mold. In this technique, and in the glass slide technique, it is possible to view the bottom of the tissue, verifying if all surgical margins are placed on the flat surface of the mold. The mold is then positioned in its specific slot on the main part. The gel is placed on the tissue in the plastic mold. The secondary piece containing the pin chuck is fitted like a sandwich in the other piece. The four points of engagement between the two parts of the device allow an exact coupling, preventing any excess inclination of the pin chuck’s surface concerning the flat surface of the metal block. Thus, there is rapid tissue freezing and diminishment of any unwanted pin chuck’s inclination regarding the flat cut surface of the surgical margins. The plastic mold is then separated from the frozen block. The pin chuck containing the block is ready to be sectioned (microtomy) (Figure 3).
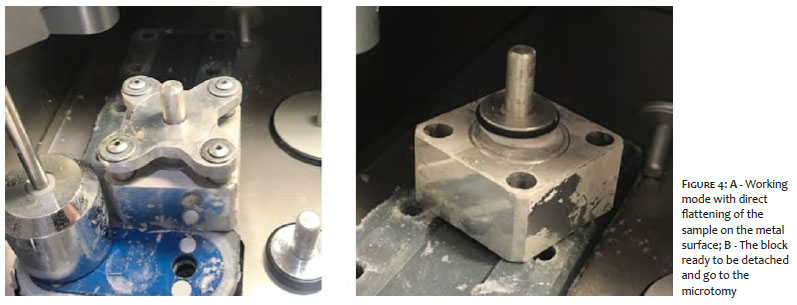
The tissue is flattened and frozen directly on the plane surface of the device. The circular groove is only used to delimit the work area. An amount of gel is placed on the sample. The secondary piece containing the pin chuck is fitted like a sandwich in the first piece. The pin chuck with the block is frozen and separated from the device, ready for microtomy (Figure 4). This working mode is ideal for tissues that are thick, difficult to relax, or that contain cartilage since the flattening directly on the metallic surface, instantly freezes the tissue, keeping the edges flat and glued to the surface of the device.
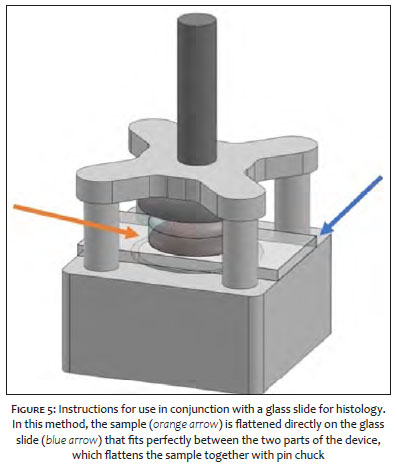
This method is similar to the traditional one, but it allows better alignment and standardization in making the blocks. The tissue is flattened directly on the surface of a glass slide for histology. It allows the cut surface to be viewed due to the transparency of the glass, making it possible to check the occurrence of bubbles and if the margins are perfectly flat. Then the blade containing the tissue is placed on the frozen surface of the main piece. The circular groove serves only as a guide for positioning the tissue within the limits of this circle. An amount of gel is placed on the sample. The secondary piece containing the pin chuck fits like a sandwich. The glass slide is detached from the frozen block, and the pin chuck containing it is separated from the device, being ready for the microtomy (Figure 5).
Due to the remarkable performance of SmartMohs® compared to conventional tissue embedding methods, the author has adopted as a standard the use of this device, having treated 72 cases with the technique so far. Despite the limitation that there are no comparative studies, it is possible to notice advantages over other techniques immediately. With each of its three working modes, some benefits can be pointed out regarding the usual method of tissue embedding: (1) Maintenance of a pattern in the inclination of the blocks, minimizing the need for adjustments in the cryostat between each processed sample, (2) Alignment of the cut surface, minimizing irregular thinning of the block, thus avoiding possible false positives (3) Time optimization, providing faster freezing and assembly of the block.
Although there are still no comparative studies of this method with other techniques of tissue embedding in Mohs surgery, the use of SmartMohs® can be an excellent option to optimize the histological processing, providing faster speed, maintaining the high-quality of the histological sections
Frederico Hassin Sanchez | 0000-0001-5856-216X
Approval of the final version of the manuscript; study design and planning; preparation and writing of the manuscript; active participation in research orientation; intellectual participation in propaedeutic and/or therapeutic conduct of studied cases; critical literature review; critical revision of the manuscript.
1. Sanchez FH, Filho JR, Nouri K, Rizzo LA. Description of a simple method to optimize the process of freezing and embedding tissue in Mohs surgery. Dermatol Surg. 2014;40(4):472-4.
2. Sanchez FH, Ribeiro J Filho, Russo AC. Validation of a new technique to freezing and embedding tissue in Mohs surgery, using an animal model. Acta Cir Bras. 2016;31(8):533-41.
3. Sanchez FH. Técnicas de inclusão tecidual. In: Sanchez FH, Marques HS, editors. Cirurgia micrográfica de Mohs: manual prático e atlas. Rio de Janeiro: Dilivros; 2019. p. 91-103.
 All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773
All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773



 Read in Portuguese
Read in Portuguese
 Portuguese PDF
Portuguese PDF
 Print
Print
 Send this article by email
Send this article by email
 How to cite this article
How to cite this article
 Submit a comment
Submit a comment
 Mendeley
Mendeley
 Pocket
Pocket
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}