


Viviane Maria Maiolini1; Lissiê Lunardi Sbroglio1; Raphaella Barboza Marques1; Roberta Teixeira da Silva2; Marcella Leal Novello D’Elia1
Received on: 24/10/2020
Approved on: 09/02/2021
Financial Support: None
Conflict of Interest: None
Study conducted at the Pedro Ernesto University Hospital of the Universidade do Estado do Rio de Janeiro, Rio de Janeiro (RJ), Brazil
Earlobes deformities caused by adornments and ornaments are prevalent. The use of plugs and piercings in this topography generates a large partial cleft in the earlobes, which causes aesthetic and social damage when abandoning its use. The literature has already proposed several surgical techniques to correct defects in the earlobes. This case report describes a new, simple, and fast surgical approach, which had satisfactory aesthetic results in significant partial cleft cases: the adapted "L-plasty" technique.
Keywords: Acquired Ear Deformities; External Ear; Otologic Surgical Procedures; Ambulatory Surgical Procedures
Deformities acquired in the ear lobe through the use of piercings, extenders, trauma, surgery, or aging are much more frequent than congenital ones, observed in 1:1500 births.1 The acquired defects can be divided into partial or total cleft, when the lobe separates into two or three ends. The total cleft corrections are divided into two large groups: with or without preserving the earring orifice when a new orifice can be made after six months of healing.2
There are several techniques for reducing and correcting the earlobe, but most of them result in a scar on the anterior or inferior portion of the lobes.1 Historically, different techniques have been proposed for auricular lobuloplasty. Miller first introduced simple wedge excision to reduce the earlobe in 1925.3
In 1954, McLaren suggested a slight scarring of the gap edges and simple suturing of the margins. In 1961, Boo-chai4 proposed the excision of part of the cleft edges and suture below the original orifice. Pardue, in 1973, developed the technique of resection of the cleft edges, leaving a piece of skin on the upper portion of one side to constitute the orifice of the lobe. Despite trying to maintain the orifice, these two techniques favor the formation of a gap in the lower margin of the lobe.5
In 1975, Hamilton and La Rossa described a technique similar to Pardue’s, associated with a zetaplasty in an attempt to minimize the formation of the notch. Argamasso, in 1978, reported a similar technique that left intact skin close to the original orifice and, in each half of the lobe, created two triangular details to suture them later.5,6 Harak, in 1982, proposed excision of tissue on the anterior surface of one of the edges, followed by excision of the same amount of tissue on the posterior surface of the other edge. This technique also does not preserve the lobe orifice.5 Kalimuthu et al. proposed the “V” flap technique, in which a “V” incision was made at the end of the lobe, followed by de-epidermization at the medial edge, and another “V” incision at the end of the lateral edge to fit after the suture.7 Fatah,8 in 1985, and Fearon & Cuadros,9 in 1990, presented the “L” flap technique, which again does not preserve the lobe orifice.5 At first, techniques that do not preserve the surroundings seem safer.2
This report proposes a new surgical technique that is simple to perform: the adapted “L-plasty” technique to correct lobes with significant defects, such as those caused by gauge ear-piercing use.
A 38-year-old man with no previous comorbidities reported using an ear reamer for about ten years. He decided to abandon the ornament use and correct the defect for aesthetic and self-esteem reasons. There was no interest in using ornaments again in the short term.
After studying the defect, we noted that the lobe had a vertical elongation, requiring a reduction in this dimension for a more aesthetic result (Figure 1).
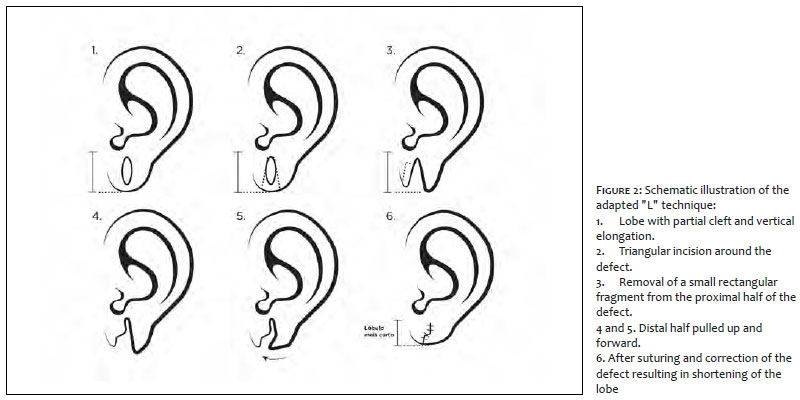
We performed the procedure on an outpatient basis using local anesthesia with infiltration of lidocaine 2% without vasoconstrictor in the ear lobes. An incision was made with a scalpel blade number 11, simultaneously in the anterior and posterior part of the lobe (Figure 2). The incision had a triangular shape around the defect caused by the gauge ear piercing, dividing the lobe into two halves (Figure 2). Then, we excised a fragment from the lower border of the proximal lobe half. The other intact half underwent a rotation of approximately 90º so that it would fit correctly in the space left by removing the quadrangular fragment (Figures 2 and 3). The suture was performed with 5-0 mononylon (Figure 4). Micropore tape was used for the primary dressing applied directly to the wound and secondary dressing with gauze fixed with micropore tape for replacement.
The primary dressing remained for seven days. The patient was reviewed on the 14th and 60th day after the operation (Figure 5).
As a final result, we observed a shortening of the lobes compared to the preoperative period, a small central scar, no gap in the area corresponding to the suture in the lower region of the lobe, a round shape, and a final natural appearance. The patient was satisfied with the outcome.
The earlobe is a crucial structure of the face, with several causes and/or changes requiring surgical correction.
Auricular lobuloplasty is performed to correct clefts in the earlobe, congenital deformities, aging, keloid formation, or auricular tumors.10 The satisfaction rate related to the results of lobuloplasty is about 92% to 100%.11,12 Good local vascularization allows the surgeon greater freedom in manipulating local tissues for making flaps and overlapping them, if necessary.13 The rate of postoperative complications is low, around 0 to 33.3%. The reported complications were hypertrophic scar, depressed scar, wide scars, recurrence of the cleft, and surgical wound infections.14,15
The use of ornaments and jewels in this topography has been traditional throughout the centuries and cultures. Currently, this trend continues. Also, a study showed that individuals with gauge ear-piercing deformities in the earlobes are more prone to negative image effects. These findings corroborate patients’ motivation to seek correction for these conditions.16
Consequently, there is a high demand for specialized treatments for aesthetic earlobe correction.5
Many techniques have already been described, including direct suture, zetaplasty, lobe correction rhytidoplasty, “V” flaps, “L” flaps, and others that use combined techniques or a variation of these, as in the case reported, which describes the adapted “L” technique.5
The lobe size and the cleft type should be considered when choosing the best surgical option: partial, typically bilateral and associated with the prolonged use of heavy ornaments, as in the case shown; and complete, usually unilateral, and occurs when the adornment is pulled abruptly.2,3 Given the existing surgical possibilities, the choice is generally for the technique that makes the lobe more similar to the original, with a rounded shape, no indentations or unevenness. If the orifice is performed, it must be centered.2
In the case presented, we reported a modified technique for reducing and remodeling the earlobe. The L-plasty8 divides the lobe into two parts by an “L” incision in both the distal and proximal halves.
In the adapted “L” technique, the lobe was divided by a triangular incision around the defect, dividing it into two halves. A small quadrangular fragment was excised from the lower border of the proximal lobe half, and the other half remained intact. It was pulled upwards and forwards (Figure 2), resulting in a fit in the space left by removing the quadrangular fragment. This maneuver reduces the vertical dimension of the previously elongated lobe.
In conclusion, we chose the adapted “L” technique due to the type of cleft presented (vertical lobe elongation). Also, it is a simple technique that presents less chance of recurrence, provides rapid correction of the primary defect, has discrete scarring, and a high probability of patient satisfaction.
Viviane Maria Maiolini | 0000-0001-5565-4886
Study design and planning; preparation and writing of the manuscript; data collection, analysis, and interpretation; critical literature review; critical revision of the manuscript.
Lissiê Lunardi Sbroglio | 0000-0002-0888-9065
Preparation and writing of the manuscript; critical literature review; critical revision of the manuscript.
Raphaella Barboza Marques | 0000-0002-9281-2166
Critical literature review; critical revision of the manuscript.
Roberta Teixeira da Silva | 0000-0002-1874-584X
Study design and planning; intellectual participation in propaedeutic and/or therapeutic conduct of studied cases.
Marcella Leal Novello D’Elia | 0000-0002-3575-5732
approval of the final version of the manuscript; study design and planning; preparation and writing of the manuscript; intellectual participation in propaedeutic and/or therapeutic conduct of studied cases; critical literature review; critical revision of the manuscript.
1. Tatar S, Sezgin B. Aesthetic earlobe reduction: a practical geometric modification with natural contour preservation. Facial Plast Surg 2019; 35:294-8.
2. Ribeiro AA, et al. Reparo do lóbulo da orelha partido: revisão da literatura e proposta de nova técnica. Surg Cosm Dermatol 2009;1(3):141-4.
3. Arasaratnam RBS, et al. Repair of large holes in stretched earlobes. Clin Otolaryngol. 2011;36:588-98.
4. Boo-Chai K. The cleft earlobe. Plast Reconstr Surg 1961;28:681-8.
5. Patrocínio LG, Morais RM, Pereira JE, Patrocínio JA. Earlobe cleft reconstructive surgery. Rev Bras Otorrinolaringol. 2006;72(4):447-51.
6. Venkatramani H. A new technique in closure of wide clefts of earlobule. Plast Reconstr Surg. 1999;104(1):296-7.
7. Kalimuthu R, Larson BJ, Lewis N. Earlobe repair: a new technique. J Dermatol Surg Oncol. 1982;8:187-91.
8. Fatah MF. L-plasty technique in the repair of split earlobe. Br J Plast Surg 1985;38:410-4.
9. Fearon J, Cuadros CL. Cleft earlobe repair. Ann Plast Surg. 1990;24(3):252-7.
10. Altıntaş A, Çelik M, Yeğin Y, Kayabaşoğlu G. Auricular lobuloplasty. Turk Arch Otorhinolaryngol 2017;55:172-6.
11. Miller TR, Eisbach KJ. Repair of enlarged pierced-ear openings. Ear Nose Throat J 2005;84:276-7.
12. Reiter D, Alford EL. Torn earlobe: a new approach to manage-ment with a review of 68 cases. Ann Otol Rhinol Laryngol 1994;103:879-84.
13. Pereira AA, Tien SLK, Silva GB, Bessa CMC, Awad M. Reconstrução de lóbulo após alargador de orelha. Rev. Bras. Cir. Plást. 2011;26(3):38.
14. Ribeiro AA, Lourenço L, Matsuda TMHB, Ferrari NM. Split earlobe repair: literature review and new technique proposal. Surg Cosmet Dermatol 2009;1:141-4.
15. Sharma R, Krishna S, Kumar S, Verma M. Rotation flap lobuloplasty: technique and experience with 24 partially torn earlobes. Int J Oral Maxillofac Surg 2014;43: 1206-10.
16. Fung N, et al. Stretched earlobe piercings negatively impact casual observer perceptions. Facial Plast Surg. 2019;35:299-305.
 All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773
All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773



 Read in Portuguese
Read in Portuguese
 Portuguese PDF
Portuguese PDF
 Print
Print
 Send this article by email
Send this article by email
 How to cite this article
How to cite this article
 Submit a comment
Submit a comment
 Mendeley
Mendeley
 Pocket
Pocket
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}