


Flávia Trevisan1; Dâmia Kuster Kaminski Arida2; Laila Djensa Souza dos Santos2; Paola Tamara Silva Zakszewski2; Fernanda Beatriz Moutinho Zamuner Walger2
Received on: 07/10/2019
Approved on: 09/02/2021
Financial Support: None
Conflict of Interest: None
Study conducted at the Faculdade Evangélica Mackenzie, Paraná, Curitiba (PR), Brazil
Cryosurgery is a technique widely known and used among dermatologists. Intralesional application is already used to treat keloids and has the advantage of restricting the zone of action of low temperatures of liquid nitrogen. The use of contact cryosurgery in vascular lesions is well reported in the literature, but there are no intralesional technique publications on these types of lesions. Here, we report two cases, one of port-wine stain hamartomas in a 61-year-old patient and another of a cherry angioma in a 70-year-old patient, safely and satisfactorily treated with intralesional cryosurgery.
Keywords: Cryosurgery; Cryotherapy; Hamartoma; Hemangioma; Vascular malformations
Vascular lesions are a reason for dermatological consultation for bleeding prevention or aesthetic motives. They can be congenital or acquired and are classified into tumors and malformations.1,2
The port-wine stain (PWS) is a congenital vascular lesion presented as solid stains and unilateral plaques, with segmental distribution and demarcation in the midline. They can also present as small stains in any body region, varying in size, shape, and different shades of pink, red, and violet. In some cases, epithelial or mesenchymal hamartomas may develop over PWS.1,2
Cherry angioma is a benign vascular lesion, acquired and extremely common, presenting as asymptomatic red papules, from 1 mm to 15 mm, usually on the trunk, arms, and head. They have slow growth and may be associated with advancing age, diabetes, high temperatures, exposure to chemicals, liver transplantation, graft-versus-host disease, pregnancy, and climacteric.3,4
We can mention pulsed dye laser, Nd-YAG laser, electrosurgery, surgical excision, and open probe or contact cryosurgery among vascular lesions treatments.2,5 There are no published reports of cutaneous vascular lesions treatment with intralesional cryosurgery.
Cryosurgery is a treatment modality that uses low temperatures of liquid nitrogen to achieve tissue effects. It causes cell membrane rupture because of the intracellular ice crystals formation, endothelial cell junctions damage, and blood stasis, producing microthrombi, vascular injury, and, finally, tissue necrosis.6,7 Its use in an intralesional form has been applied to hypertrophic scars and keloids.6-9 When liquid nitrogen passes through the needle, a lethal zone is created around the device inserted in the dermis. It differentiates intralesional cryotherapy from contact cryotherapy, which forms a lethal zone located mainly on the epidermis.7
This report aims to suggest intralesional cryosurgery as a therapeutic option for vascular lesions with a tumor component, reporting the method and the evolution of two cases: a hamartoma on a PWS and a cherry angioma.
We used a similar technique in both cases. The lesions were subjected to antisepsis with 0.5% chlorhexidine digluconate alcohol solution and infiltrative local anesthesia with lidocaine 2% and epinephrine 1:200,000. Then, with an 18G (40x1.2mm) gauge disposable needle, the lesion was transfixed, and the cryosurgery device was coupled. To prevent the spray jet from causing damage to the patient or applying doctor, a shield, for example, a gauze, can be placed a few centimeters from the needle’s piercing orifice. The freezing time was 30 to 60 seconds. Complete thawing was conducted, and the needle was removed. At this stage, compression for 5 to 10 minutes can easily control the bleeding.
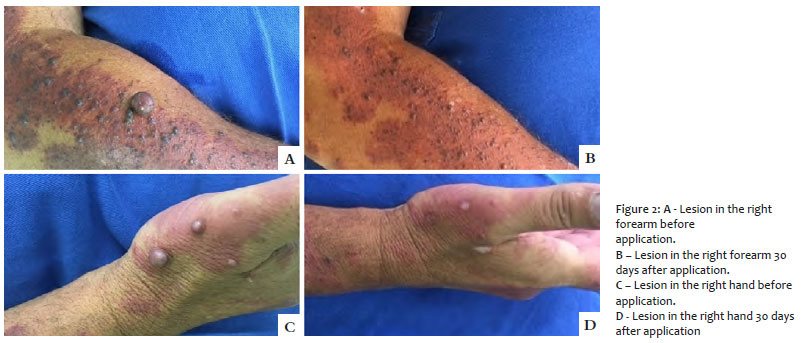
The first patient was a 61-year-old man, smoker, who presented PWS in his right arm and forearm since birth. Approximately five years ago, asymptomatic tumors and erythematous-purple nodules of up to 1.3 cm appeared on the stain, causing discomfort with the friction of the clothes on the lesions. We selected three lesions for treatment with intralesional cryosurgery and submitted each one separately to a continuous freeze cycle of 30 seconds, awaiting the complete thawing of the lesion to remove the needle (60 to 70 seconds). An occlusive dressing, maintained for 24 hours, completed the procedure.
The second patient was a 70-year-old man, ex-smoker for 22 years, with controlled hypertension, who presented an erythematous-violaceous nodule of 1 cm in the right temporal region for four years. The lesion had slow growth and was asymptomatic but had a history of repeated trauma when combing the hair. After antisepsis and anesthesia, the lesion was transfixed, and then the cryosurgery device was attached. A continuous freeze cycle of 60 seconds was performed, and complete thawing of the lesion was awaited to remove the needle (190 seconds). After thawing, there was local bleeding, contained with compression for 5 minutes. An occlusive dressing, maintained for 24 hours, completed the procedure.
In the first patient, the lesions evolved with necrosis (Figure 1) and detachment approximately ten days after the procedure. The sites showed no pain or secondary infection. There was slight and minor residual hypochromia after complete healing (Figures 2A, B, C, and D).
In the second case, the lesion evolved with the formation of a slight crust after ten days and total healing in 20 days, with only a small residual hypochromic stain remaining on the site.
Cryosurgery is a simple, safe, inexpensive procedure that produces aesthetically acceptable results. It can be used to treat several benign, pre-malignant lesions and well-defined malignant tumors.5 Cold intolerance, Raynauld’s disease or phenomenon, cold urticaria, cryoglobulinemia, pyoderma gangrenosum, autoimmune disorders, and active infections at the site are absolute contraindications for cryotherapy.5
Vascular lesions are susceptible to destruction by cryosurgery. The low temperature promotes vasoconstriction and stasis. From -15 oC to -40 oC, it can cause endothelial damage. With thawing, microthrombi formation, edema, erythema, and tissue necrosis occur. The mechanism of cell necrosis occurs by direct damage, through lower temperatures observed in the center of the lesion, and by indirect damage, through damage to blood vessels.5
The intralesional form of cryosurgery has already been described for keloid therapy, squamous cell carcinoma, and basal cell carcinoma.6-10 With this method, freezing is initiated at the core of the lesion and spreads to its surface. It contrasts with the contact or spray cryosurgery mechanism, which freezes the lesion from the skin surface. In the first weeks after treatment, there may be edema, mild to moderate local pain, blistering, and superficial necrosis.9
The advantage of this procedure is its speed, the possibility of conducting it under local anesthesia, excellent cost/benefit, easy care for the surgical wound, quick learning by the doctor, and great tolerability by the patient.7,10 Another advantage is the smaller scar area and less hypopigmentation generated with the intralesional method than contact cryotherapy.7,9,10
As a disadvantage, the technique prevents histological confirmation in doubtful cases or those requiring verification of the surgical margin.9
In this report, we successfully applied intralesional cryosurgery to treat two types of vascular lesions: hamartomas on PWS and cherry angioma. After the procedures, there was edema and a halo of erythema in the first 48 hours, evolving with necrosis and darkening in the next seven to ten days. The detachment of the lesions occurred around the tenth day, with total healing between 20 and 30 days. Hypo or achromia and mild atrophy at the site were perceived sequelae.
The intralesional cryosurgery technique for vascular lesions treatment, such as those reported here, in addition to being simple, fast, and inexpensive, has good resolution, low risk, few scar sequelae, and aesthetically satisfactory results.
Flávia Trevisan | 0000-0001-5855-3685
Approval of the final version of the manuscript; study design and planning; preparation and writing of the manuscript; data collection, analysis, and interpretation; active participation in research orientation; intellectual participation in propaedeutic and/or therapeutic conduct of studied cases; critical literature review; critical revision of the manuscript.
Dâmia Kuster Kaminski Arida | 0000-0002-6350-245X
Preparation and writing of the manuscript; data collection, analysis, and interpretation; intellectual participation in propaedeutic and/or therapeutic conduct of studied cases.
Laila Djensa Souza dos Santos | 0000-0002-5263-4094
Preparation and writing of the manuscript; data collection, analysis, and interpretation; intellectual participation in propaedeutic and/or therapeutic conduct of studied cases; critical literature review.
Paola Tamara Silva Zakszewski | 0000-0002-5970-3320
Preparation and writing of the manuscript; data collection, analysis, and interpretation; intellectual participation in propaedeutic and/or therapeutic conduct of studied cases.
Fernanda Beatriz Moutinho Zamuner Walger | 0000-0003-0500-1072
Preparation and writing of the manuscript; data collection, analysis, and interpretation; intellectual participation in propaedeutic and/or therapeutic conduct of studied cases; critical literature review.
1. Rozas-Muñoz E, Frieden IJ, Roé E, Puig L, Baselga E. Vascular stains: proposal for a clinical classification to improve diagnosis and management. Pediatr Dermatol. 2016;33(6):570-84.
2. Gontijo B, Pereira LB, Silva CMR. Malformações vasculares. An Bras Dermatol. 2004;79(1):7-25.
3. Pereira, JM. Hemangioma rubi no couro cabeludo. An Bras Dermatol. 2004;79(1):83-9.
4. Kim J, Park H, Ahn SK. Cherry hemangioma on the scalp. Case Rep Dermatol. 2009;1(1):82-6.
5. Zanini M, Machado CAS, Brandão JA, Timoner F. Criocirurgia na malformação venosa labial. Relato de Caso. Med Cutan Iber Lat Am. 2005;33(2):73-5.
6. Mourad B, Elfar N, Elsheikh S. Spray versus intralesional cryotherapy for keloids. J Dermatolog Treat. 2016;27(3):264-9.
7. Abdel-Meguid AM , Weshahy AH , Sayed DS , Refay AE , Awad SM. Intralesional vs. contact cryosurgery in treatment of keloids: a clinical and immunohistochemical study. Int J Dermatol. 2015;54(4):468-75.
8. Goldenberg G; Luber AJ. Use of intralesional cryosurgery as an innovative therapy for keloid scars and a review of current treatments. J Clin Aesthet Dermatol. 2013;6(7):23-6.
9. Leeuwen MCE, Bulstra AEJ, Ket JCF, Ritt MJPF, Leeuwen PAM, Niessen, FB. Intralesional cryotherapy for the treatment of keloid scars: evaluating effectiveness. Plast Reconstr Surg Glob Open. 2015;3(6):437.
10. Har-Shai Y, Sommer A, Gil T, Krausz J, Gl-ou N, Mettanes EU, et al. Criocirurgia intralesional para o tratamento do carcinoma basocelular dos membros inferiores em idosos: um estudo de viabilidade. Int J Dermatol. 2016;55(3):342-50.
 All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773
All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773



 Read in Portuguese
Read in Portuguese
 Portuguese PDF
Portuguese PDF
 Print
Print
 Send this article by email
Send this article by email
 How to cite this article
How to cite this article
 Submit a comment
Submit a comment
 Mendeley
Mendeley
 Pocket
Pocket
{kind=link}
{kind=link}