


Emerson Henrique Padoveze1; Nilton Gioia Di Chiacchio2; Thais Cardoso Pinto2; Aarão Andrade Napoleão Lima2; Gabriel Lucchesi de Santana3
Received on: 24/08/2020
Approved on: 26/11/2020
Financial support: None
Conflict of interest: None
Study conducted at the Hospital do Servidor Público Municipal de São Paulo, São Paulo (SP), Brazil
Basal cell carcinoma over the tattoo region has been poorly reported in the literature, with a total of 13 cases. All cases describe the clinical aspect of the lesion and its pathogenesis but do not characterize the dermoscopy. We report two cases of basal cell carcinoma on tattoos with clinical and dermoscopy features, treated with Mohs micrographic surgery. It was challenging to establish the tumor’s clinical and dermoscopic margins due to the tattoo’s exogenous pigment.
Keywords: Carcinoma, Basal cell; Dermoscopy; Tattooing; Mohs surgery
The art of tattooing is an ancient practice that is becoming increasingly popular, both for cosmetic and therapeutic purposes. Although well-tolerated, it is not without risks.1 Several benign and malignant complications can result from the tattooing process, according to the literature.1,2,3,4,5,6 There are reports of neoplastic evolution in the form of cutaneous lymphoma, keratoacanthoma, squamous cell carcinoma (SCC), melanoma, and basal cell carcinoma (BCC).1,2,3
Basal cell carcinoma (BCC) has already been described in scars (burns and post-vaccination). However, the appearance on a tattoo is uncommon, and the pathogenesis is unclear. The literature has only reported 13 cases, most in photoexposed areas and containing black pigment.3 There is a possibility that the pigment has a direct carcinogenic effect or that the lesion is associated with trauma and sun exposure.1,3,5,6
Dermoscopy is an additional high sensitivity and specificity tool for BCC diagnosis. The most commonly described findings are arboriform telangiectasias, bright white areas, and bluish-gray ovoid nests.7 The reported cases do not describe the dermoscopic findings of the tumor on the tattoo. We report two cases with clinical and dermoscopic characteristics.
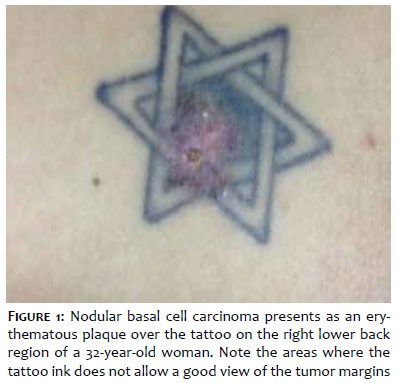
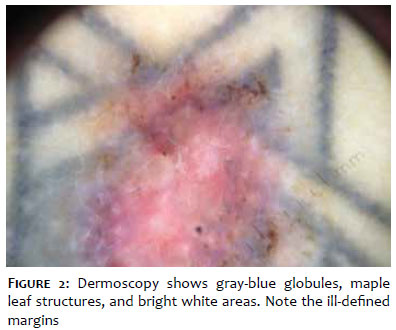
A 32-year-old woman, Caucasian, presenting a single infiltrated erythematous nodule measuring 1.4 x 2.0 cm in the right lower back region for nine years (Figure 1). The lesion was on a tattoo done 12 years ago. Dermoscopy revealed blue-gray globules, ulceration, maple leaf structures, and bright white areas (Figure 2). Histology showed dermis’ infiltration by atypical basaloid cells, forming small blocks with peripheral palisade, characteristic of BCC.
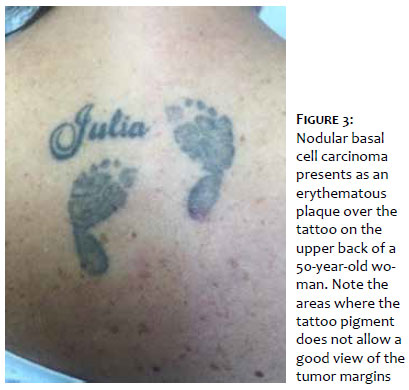
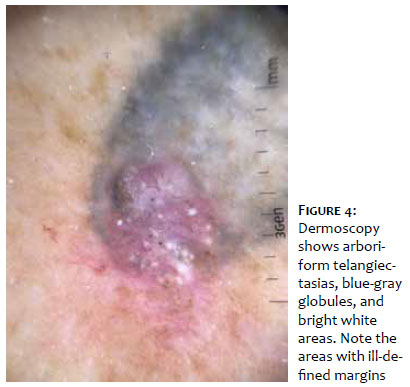
A 50-year-old woman, brown, presenting an erythematous-infiltrated plaque on the upper back measuring 1.0 x 0.8 cm, for one year, on a tattoo performed six years ago (Figure 3). Dermoscopy revealed arboriform telangiectasias, blue-gray globules, and bright white areas (Figure 4). The anatomopathological examination showed infiltration of atypical basaloid cells, forming small blocks, invading the dermis with a palisade peripheral disposition, compatible with BCC diagnosis.
Both patients underwent Mohs micrographic surgery and are undergoing clinical follow-up for four and three years, respectively, with no lesion recurrence.
The art of tattooing has been practiced for millennia for aesthetic and therapeutic purposes. The literature reported numerous medical complications related to tattoos, including lichenoid dermatitis, pseudolymphoma, tetanus, cancer, syphilis, molluscum contagiosum, warts, HIV, hepatitis, granulomas, mycoses, and hypersensitivity reactions. It has also described malignant lesions after tattooing, although rare, such as dermatofibrosarcoma protuberans, keratoacanthoma, leiomyosarcoma, melanoma, and squamous cell carcinoma (SCC).1,2,3
Bashir described the first BCC report on the tattoo region in 1976, reporting two cases.4 Since then, the literature has depicted only 11 more patients. None of them described the dermoscopic characteristics.
The pathogenesis is still uncertain. The trauma hypothesis is considered a possible factor related to its carcinogenesis. It generates greater sensitivity to sun exposure due to the low vascularization and elasticity of the injured tissue. Such changes, consequently, could result in localized nutritional deficiency, chronic irritation, and prolonged release of toxins, leading to cell mutation.1,5,6
The dermoscopic features most commonly seen in BCC are the arboriform vessels (59%), bright white structures (49%), and large blue-gray ovoid nests (34%).7 In our cases, we observed bright white areas, blue-gray globules, and arboriform vessels in only one of them.
It is essential to establish safe tumor margins, both clinically and with the aid of dermoscopy, for its complete removal. In our cases, it was difficult to accurately establish tumor margins due to pigment, both clinically and with Dermoscopy. It resulted in performing the Mohs surgery in a larger number of phases.
Although our cases are the first described with dermoscopic characteristics, we can conclude that dermoscopy did not contribute to a good delimitation of the tumor margins.
Emerson Henrique Padoveze | 0000-0003-1106-0992
Approval of the final version of the manuscript; preparation and writing of the manuscript; critical literature review; critical revision of the manuscript.
Nilton Gioia Di Chiacchio | 0000-0001-5944-7737
Approval of the final version of the manuscript; preparation and writing of the manuscript; critical literature review; critical revision of the manuscript.
Thais Cardoso Pinto | 0000-0001-9907-6141
Preparation and writing of the manuscript; critical literature review; critical revision of the manuscript.
Aarão Andrade Napoleão Lima | 0000-0003-0648-6884
Preparation and writing of the manuscript; critical literature review; critical revision of the manuscript.
Gabriel Lucchesi de Santana | 0000-0001-6406-2831
Preparation and writing of the manuscript; critical literature review.
1. Lee JS, Park J, Kim SM, Yun SK, Kim HU. Basal cell carcinoma arising in a tattooed eyebrow. Ann Dermatol. 2009;21(3):281-4.
2. Goldstein IV. Complications from tattoos. J Dermatol Surg Oncol 1979;5(11):869-78.
3. Doumat F, Kaise W, Barbaud A, Schmutz JL. Basal cell carcinoma in a tattoo. Dermatology. 2004;208(2):181-2.
4. Bashir AH. Basal cell carcinoma in tattoos: report of two cases. Br J Plast Surg. 1976;29(4):288-90.
5. Wiener DA, Scher RK. Basal cell carcinoma arising in a tattoo. Cutis 1987;39(2):125-6.
6. Paprottka FJ, Krezdorn N, Narwan M, et al. Trendy tattoos maybe a serious health risk? Aesthet Plast Surg. 2018;42(1):310-21.
7. Reiter O, Mimouni I, Dusza S, Halpern AC, Leshem YA, Marghoob AA. Dermoscopic features of basal cell carcinoma and its subtypes: a systematic review. J Am Acad Dermatol. Epub 2019 Nov 7.
 All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773
All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773



 Read in Portuguese
Read in Portuguese
 Portuguese PDF
Portuguese PDF
 Print
Print
 Send this article by email
Send this article by email
 How to cite this article
How to cite this article
 Submit a comment
Submit a comment
 Mendeley
Mendeley
 Pocket
Pocket
{kind=link}
{kind=link}
{kind=link}
{kind=link}