


Elisete Isabel Crocco1,2; Ana Paula Kayo2; Renata Alves2; Bomi Hong2
Received on: 10/07/2020
Approved on: 18/10/ 2020
Financial support: Libbs Pharmaceuticals
Conflict of interest: Libbs Pharmaceuticals sponsored this study; however, the researchers conducted all the methodology, execution, and analysis of the results obtained with no interference from the pharmaceutical industry
Study conducted at the Elisete Crocco Dermatology Clinic, São Paulo (SP), Brazil
INTRODUCTION: Melasma is a recurrent and challenging dermatosis despite several clinical and interventional therapeutic approaches.
OBJECTIVE: This study aims to assess the safety and efficacy of using a bleaching cream in the period immediately after serial surface peels.
METHODS: Five women with melasma used a cream containing bleaches, moisturizers, and tranquilizers during the treatment period with serial surface peels. We assessed them in D0, D7, D30, D37, D60, D67, and D90 through photographs, record of the physician’s and patient’s opinion, description of adverse events, need to interrupt using the product, and the MELASQol questionnaire.
RESULTS: We observed improved hydration, skin quality, and bleaching, with little discomfort and a significant reduction in MELASQol scores, with statistical evidence.
CONCLUSIONS: The use of a topic cream with bleaching and tranquilizing properties is an effective and safe alternative to avoid interruption of melasma treatment during the period of serial surface peels.
Keywords: Chemexfoliation; Hyperpigmentation; Pigmentation disorders
Melasma is a chronic dermatosis that is difficult to control and affects many of the adult population. The disorder has a significant impact on the quality of life, causing social and psychological stress. Despite much research involving its etiology, pathogenesis, and treatment options, this disease remains a therapeutic challenge for dermatologists. A definitive treatment modality is still a distant reality.1
Serial superficial chemical peels are useful methods in clinical practice due to their low cost and ease of application.2 However, repeated sessions cause erythema and post-inflammatory hyperpigmentation, especially in patients with higher skin phototypes.1 In this scenario, one of the difficulties of melasma therapy is maintaining the topical use of skin bleaching products during the period of repeated sessions of this procedure. Usually, the patient keeps only the use of moisturizers and calming agents.
The proposal to use a topical bleaching product with soothing properties emerged as an alternative to avoid interruption of melasma treatment, even during the period of peels.
In this study, we report the use of a bleaching, moisturizing, and soothing cream immediately after the application of serial chemical superficial peels in patients with melasma.
This pilot, single-center, prospective, clinical study was structured according to the Declaration of Helsinki’s ethical rules. All patients signed the informed consent form.
We selected five women with mixed melasma on the face, with no history of procedures for this dermatosis in the last six months.
All patients underwent a monthly series (D0, D30, D60) of three superficial peels with Jessner’s solution applied to the whole face, followed by retinoic acid 5%, after skin cleansing with water and neutral soap and degreasing with Hoffmann’s liquor. The patients were instructed to wash their face only after six hours, using a light soap with moisturizing properties (Figure 1).
The volunteers were instructed to use the product under study (Lumixyl® - Libbs Pharmaceutical, São Paulo, Brazil) twice daily, stopping its use on the day of applying the peeling and restarting it the following day. The study product is a blend of the bleaching products decapeptide-12, phenylethyl resorcinol, and Phyllanthus emblica combined with calming agents (allantoin, aloe vera, panthenol, licorice), and moisturizers (hyaluronic acid, glycerin, sodium PCA).
The patients were assessed on seven dates: D0, D7, D30, D37, D60, D67, and D90, using photographs, records of the physician’s opinion on the skin characteristics, adverse events description, need for interrupting the use of the product or association with topical corticosteroids, as well as the volunteer’s opinion regarding skin quality and MELASQol answering.
The MELASQoL (Melasma Quality of Life Scale) is an instrument used to assess the quality of life of people with melasma, covering three areas: social life, recreation/leisure, and emotional well-being, generally those most affected by dermatosis.3 The use of the questionnaire in countries where English is not the official language requires a correct translation and cultural adaptation. In Brazil, it was translated into Portuguese in 2006 (MELASQoL-BP), following the standards of the World Health Organization (WHO).4,5,6
Regarding statistical studies, categorical data were summarized using the absolute (n) and relative (%) frequency of the number of patients concerning the total evaluated at each study visit.
For the assessment of MELASQoL, the data were summarized using the mean and standard deviation at each study visit. A mixed model of analysis of variance with repeated measures and Tukey’s multiple comparisons were used to verify the variation of the score at evaluation time. Statistical significance was considered for p values <0.05.
The five patients had a mean age of 48.4 years ± 10.06 years and skin phototypes I to V. They performed all scheduled visits, responded spontaneously to questionnaires, and took the required photographs.
There were no reports of serious adverse events. One patient temporarily stopped using the product at D4 and resumed use after guidance from the medical team at D8. The interruption occurred due to edema and erythema after the peeling, an unusual condition for the volunteer, who decided to stop the application for three days.
The volunteers did not need to use topical corticosteroids or moisturizers, although the medical team advised it if there was a lot of discomfort after the peeling. No patient stopped using soap and sunscreen.
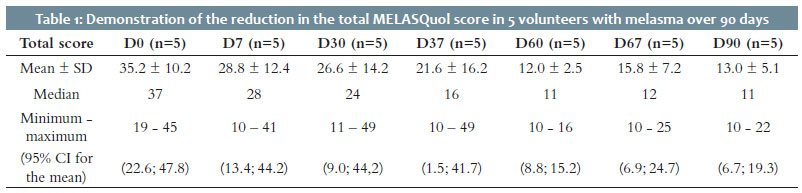
The total MELASQol score was assessed using a mixed model with repeated measures demonstrating a significant reduction in MELASQoL when comparing all visits (p=0.001) (Table 1). When evaluating graphs 1 and 2, a very similar pattern is observed between visits D0 and D30, and between D60 and D90.
The assessments conducted one week after applying the peeling followed by continuous use of the product under study showed that after the first application (D7), there was discomfort from the patients and perception of little hydration by the medical team. However, the two other post-procedure visits (D37 and D67) showed that the volunteers had a better hydration profile, skin quality, skin whitening, and little discomfort (Tables 2 and 3).
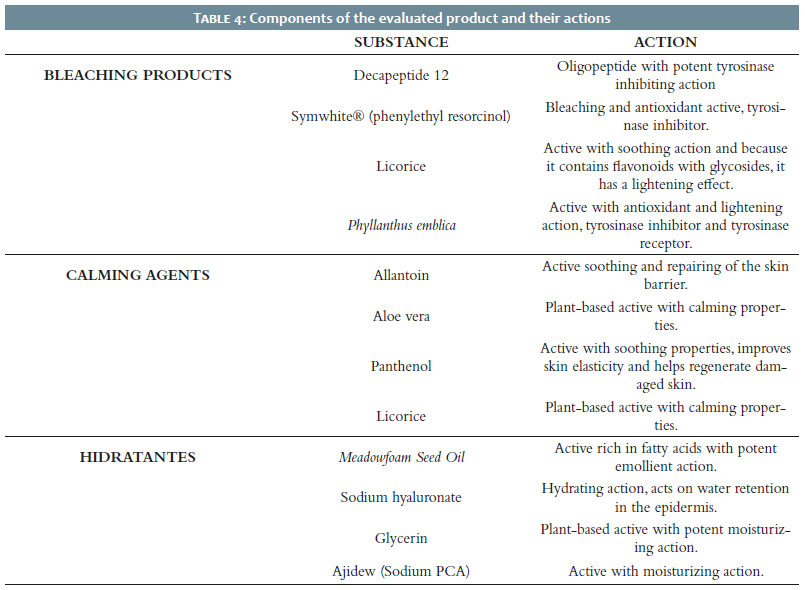
The product used in this study consists of substances with bleaching action: decapeptide 12, symwhite® (phenylethyl resorcinol), licorice, Phyllanthus emblica; in addition to substances with a calming effect: allantoin, aloe vera, panthenol, licorice; along with moisturizers substances: meadowfoam seed oil, sodium hyaluronate, glycerin, Sodium PCA (Table 4).
Currently, melasma dyschromia is considered a multifactorial dermatosis, a disease of photoaging.7 The difficulty in improving the pigmentation in keratinocytes and the decrease in melanin production justifies the approach of multiple substances and treatment strategies.
This technique aimed to early introduce bleaching actives after the epidermal loss and renewal procedure that occurs in serial superficial peels combining Jessner’s solution and retinoic acid, availing from the loss of the skin barrier and creating a “drug-delivery-like” situation. The presence of calming agents amid bleaching actives allowed the protocol’s conduction without sensitization or serious adverse events in these reported cases.
The volunteers used a product that allowed bleaching and improved skin quality, assessed through MELASQol.
Melasma remains a difficult-to-control dermatosis, in which some interventions often worsen the condition with hyperpigmentation. We demonstrated the possibility of using a bleaching active to enhance the action of serial superficial peels with Jessner’s solution and retinoic acid safely in patients with melasma.
Elisete Isabel Crocco | 0000-0002-8844-2887
Approval of the final version of the manuscript; study design and planning; preparation and writing of the manuscript; data collection, analysis, and interpretation; active participation in research orientation; intellectual participation in propaedeutic and/or therapeutic conduct of studied cases; critical literature review; critical revision of the manuscript.
Ana Paula Kayo | 0000-0001-6357-4835
Data collection, analysis, and interpretation.
Renata Alves | 0000-0001-6441-4091
Data collection, analysis, and interpretation.
Bomi Hong | 0000-0003-1656-601X
Data collection, analysis, and interpretation.
1. Sarkar R, Bansal S, Garg VK. Chemical peels for melasma in dark skinned patients. J Cutan Aesthet Surg.2012;5(4):247-53.
2. Wiest L. Current peeling methods. Hautarzt. 2003;29:21-6.
3. Costa A, Pereira MO, Moisés TA, Cordero T, Silva ARD, Amazonas FTP, et al. Avaliação da melhoria na qualidade de vida de portadoras de melasma após uso de combinação botânica à base de Bellis perennis, Glycyrrhiza glabra e Phyllanthus emblica comparado ao da hidroquinona, medido pelo MELASQol. Surg Cosmet Dermatol. 2011;3(3):207-12.
4. Freitag FM, Cestari TF, Leopoldo LR, Paludo P, Boza JC. Effect of melasma on quality of life in a sample of women living in southern Brazil. J Eur Acad Dermatol Venereol. 2008;22(6):655-62.
5. Cestari TF, Balkrishann R, Weber MB, Prati C, Menegon DB, Mazzzotti NG, et al. Translation and cultural adaptation to Portuguese of a quality of life questionnaire for patients with melasma. Med Cut Iber Lat Am. 2006;34(6):270-4.
6. Cestari TF, Hexsel D, Viegas ML, Azulay L, Hassun K, Almeida ART, et al. Validation of a melasma quality of life questionnaire for Brazilian Portuguese language: the MelasQoL-BP study and improvement of QoL of melasma patients after triple combination therapy. Br J Dermatol. 2006;156(Suppl 1):13-20.
7. Passeron T, Picardo M. Melasma, a photoaging disorder. Pigment Cell Melanoma Res. 2018;31(4):461-65.
 All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773
All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773



 Read in Portuguese
Read in Portuguese
 Portuguese PDF
Portuguese PDF
 Print
Print
 Send this article by email
Send this article by email
 How to cite this article
How to cite this article
 Submit a comment
Submit a comment
 Mendeley
Mendeley
 Pocket
Pocket
{kind=link}
{kind=link}
{kind=link}