


Débora Aparecida O. Modena; Renata Michelini Guidi; Ciro Dantas Soares; Everton Cazzo; Elinton Adami Chaim
Received on: 26/10/2020
Approved on: 27/11/2020
Financial support: None
Conflict of interest: Authors 1 and 2 are researchers at the company Ibramed, the device manufacturer. The researchers conducted the methodology, execution, and analysis of the results obtained without any interference from the company above
Study conducted at the Universidade Estadual de Campinas, Campinas (SP), Brazil
INTRODUCTION: Obesity is a disease that affects public health worldwide due to its comorbidities and premature death risk. Therefore, extracorporeal shock wave therapy (ESWT) technology can help treat and prevent its comorbidities.
OBJECTIVE: This study aims to assess whether ESWT can stimulate lipolysis and/or apoptosis of the fat cells of obese individuals.
METHODS: This is a comparative interventional study based on immunohistochemical analyzes of a set of subcutaneous tissue samples from women with obesity submitted to ESWT treatment. The biological material was collected at the time of bariatric surgery.
RESULTS: The survey included 14 obese women. Positivity was shown in the expression of Casp3 (p<0.0001), cCasp3 (p<0.0024), CD68+ macrophages (p<0.0001), HSL (p<0.0001), and adipophilin (p<0.0013) in the intervention sample compared to the control.
CONCLUSIONS: We conclude that ESWT stimulates apoptosis with consequent autophagic lipolysis in the adipose tissue of obese women. Thus, ESWT can be considered useful, safe, and promising adjuvant therapy for reducing adipose tissue and, consequently, for preventing and/or treating obesity.
Keywords: Dermatology; Obesity; High-Energy Shock Waves; Apoptosis
Obesity is a worldwide public health problem. It reaches pandemic levels and generates great health professionals’ concern due to its comorbidities and patients’ risk of premature death.1,2
The excessive amount of fat and its influence on fat cells characterizes obesity. The increase in body mass above cut-off values ¿¿previously established by the Body Mass Index (BMI) determines the condition, classified as Grade 1, with a BMI of 30 to 34.9; Grade 2, BMI up to 39.9; and Grade III, with BMI ≥40. Thus, BMI is proportional to body fat and is related to the risk of diseases associated with obesity.3- 6
Recent researches with experimental and clinical studies have seen great potential in electromedical resource development aiming to act in the adipose cell’s physiology to stimulate its breakdown, lipolysis, and even its death, apoptosis. It helps the weight loss process contribute to a possible decrease in risk factors for the development of comorbidities associated with obesity simultaneously with current non-invasive treatments and minimal adverse events.7,8
Extracorporeal shock wave therapy (ESWT) is one of these resources. The technology was developed based on the extracorporeal lithotripsy equipment used until now to treat kidney and urethral stones. The technological evolution allowed adaptations to the resource, and it started to be used in the rehabilitation of musculoskeletal diseases and bone consolidations. Recent studies demonstrate its ability to stimulate the proliferation of fibroblasts and the development of neocolagenesis and neoelastogenesis, improving skin tone. Some clinical investigations have been exposing that the resource can also act in the fat cell’s metabolic stimulation.7-11
Based on these studies on ESWT and the difficulty in reporting weight loss and tackling comorbidities associated with obesity, this study aims to assess whether ESWT can act to stimulate lipolysis and/or apoptosis of the adipose cell and thus contribute to reducing the risk factors in the development of comorbidities associated with obesity, validating its possible use in the conservative treatment of obesity.
The institutional ethics committee of the State University of Campinas (Unicamp) approved this clinical study under opinion No. 2.281.487.
We selected women with a weight loss of 10% of the initial weight to participate in the preoperative preparation group for bariatric surgery at the Clinics Hospital of Unicamp, with obesity with an indication for bariatric surgery. The exclusion criteria were women with metabolic diseases, skin lesions, history of deep venous thrombosis, smokers, or with an electronic device implanted as a cardiac pacemaker.
The participants received the treatment protocol established by the Thork Shock Wave® device’s manufacturer (IBRAMED- Industria Brasileira de Equipamentos Electromédicos, Amparo, São Paulo) approved by Anvisa No. 10360310036. (Figure 1). The parameters were 4,000 shots with 180 mJ of energy and 15Hz of frequency, using 15 mm stainless steel tip, and 2,000 shots with 100mJ of energy and 15Hz of frequency, using 15 mm plastic tip. For the tip slip, Neutral Thork® Lotion, RMC was used. The study held seven ESWT sessions, with an average time of seven minutes each, twice a week. The seventh session was held minutes before the bariatric surgery procedure. The therapy was performed in an area of ¿¿150 cm2 on the left side of the abdominal region following the midline. The right side of the participants’ abdomen did not receive ESWT and was termed as control.
We collected the samples at the time of the bariatric surgery procedure. Participants were under general venous anesthesia and mechanical ventilation. At the time of the surgical incision, the doctors removed two fragments of adipose tissue with an average size of 5 cm in diameter, with one sample from the left side of the intervention and another from the right side, which was considered a control.
After collection, we stored the material in a container with 10% formaldehyde for 48 hours. Samples were processed, embedded in paraffin, and then cut with a rotating microtome in sections of 3-5 µm thickness.
Immunohistochemical reactions were performed in sections of 3 µm thickness arranged on silanized slides. We used the antibodies polyclonal anti-Caspase3 (polyclonal; ref. 9662S; Cell Signaling Technology, Danvers, MA, USA), monoclonal anti-Cleaved Caspase 3 (clone (Asp175)(5A1); dilution 1:1000; ref. 9664S; Cell Signaling Technology), monoclonal anti-CD68 (clone KP1; dilution 1:1000; ref. ab955; Abcam, Cambridge, MA, USA), monoclonal anti-Hormone-sensitive lipase – HSL – (clone G-7, dilution 1:500, ref. sc-74489, Santa Cruz Biotechnology, Dallas, TX, USA) e Adipophilin (clone 2C5A3, dilution 1:500, ref. ab181463, Abcam). After preparing the slides, we analyzed them with a DMR microscope (Leica) and took photographs at 400X magnification. We used the ImageJ® software (NIH, Bethesda, USA) to quantify the analyzes.
All reactions were performed according to the manufacturers’ protocol and standardized by the laboratory of pathological analysis at the Clinics Hospital of Unicamp. We conducted the immunostaining quantification considering the number of positive cells and the intensity, with final scores ranging from 0-300.
Data were subjected to normality tests and then analyzed by test t student since they had a regular distribution. Values ¿¿of P<0.05 were considered statistically significant.
In total, 20 women participated in the research; however, only 14 finished the treatment and underwent surgical procedure. The remaining six participants were excluded for not following the internal preoperative program’s protocol for bariatric surgery at the Clinics Hospital of Unicamp.
Participants had a mean age of 35.0 ± 8.6 years, initial weight of 110±5.2 kg, final weight of 95.2±6.3 kg, height of 1.63±0.05 cm2, body mass index (BMI) of 41.4±2.2 kg/cm2, and final BMI of 35.8±2.1 kg/cm2, considered obesity grade II and III. None of the participants had associated pathologies such as diabetes and hypertension.
Morphologically, the control group’s adipose tissue showed uniformity in the mature fat cells, with similar sizes. The treated group showed fat cells of different sizes, disorganized, often with a degeneration process. We also observed a chronic inflammatory process with fibrosis in the treated group, indicating repair and remodeling process in the deep dermis.
Fat and inflammatory cells adjacent to the adipose tissue revealed expression of Caspase 3 (Casp3) and Cleaved Caspase 3 (cCasp3) (Figure 1). The treated group presented higher scores of both markers than the control group (p<0.0001 for Casp3 and p<0.0024 for cCasp3).
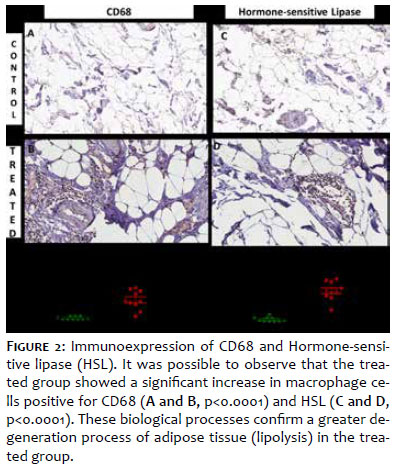
As for CD68 expression, the control sample showed an absence of macrophages and HSL-positive inflammatory cells. However, the treated group presented a moderate amount of macrophages (CD68+) and inflammatory cells positive for HSL in the region adjacent to the adipose tissue. The scores had statistically significant differences (p<0.0001 for CD68+ macrophages, p<0.0001 for HSL) (Figure 2).
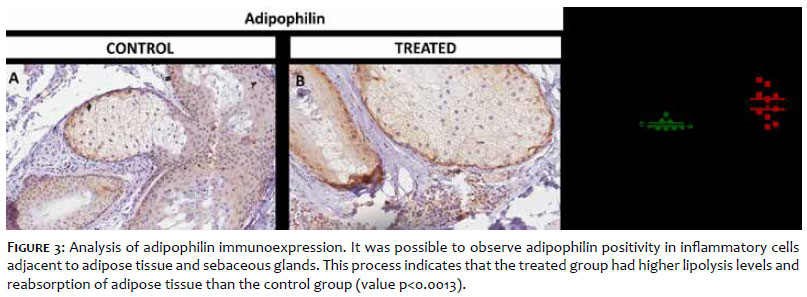
Adipophilin demonstrated immunopositivity in sebaceous glands, macrophages, and inflammatory cells present in the dermis. After quantification, it was possible to observe a significant increase in the number of adipophilin-positive cells in the treated group compared to the control group (p <0.0013) (Figure 3).
The most common adverse events reports were presented by 14.28% of the participants: presence of erythema, formation of petechiae, and mild edema in the treatment region. All of them were resolved after the end of treatment. None of the participants claimed painful discomfort during treatment.
The present study results demonstrate that treatment with ESWT was able to alter the fat cell’s metabolism with consequent stimulation of autophagic lipolysis through the apoptotic pathway, increasing the number of apoptotic cells, as well as inducing chronic inflammation and expression of adipophilin and HSL in macrophages. Together, these results may indicate a possible benefit of ESWT in the conservative treatment of obesity and its comorbidities, stimulating the lipolysis process through the apoptotic pathway.
The rapid increase in the global prevalence of obesity is a worrying fact and a serious public health problem. The molecular changes in the obese individual result in glucose and lipid metabolism deregulation and other metabolic diseases development, including insulin resistance, hyperglycemia, fatty liver, dyslipidemia, and chronic inflammation. In short, the main consequences of obesity are an increase in the prevalence and severity of Type II Diabetes and chronic heart disease, diseases that generate comorbidities and are involved in the process of premature death of these individuals.12-16
Lipolysis is a complex biological process mediated by several molecular pathways. Among them, the apoptotic pathway directly associates with decreased adipose tissue. Apoptosis can be considered crucial for maintaining homeostasis in various tissues, regulating programmed cell death, and avoiding energy imbalance. Several endogenous stimuli can lead to apoptosis, and each cell responds according to the energy and intensity of that stimulus, leading to the activation of proteases called “caspases”. Depending on the stimulus intensity, the cell may even suffer necrosis. After apoptosis or necrosis, macrophages phagocyte and digest cell debris, reducing the number of cells. 16-19
Aware of the endogenous and routine physiological events in our organism and the growing advance of obesity in an alarming way, big electromedical equipment companies started to invest in science and technology to develop equipment that could stimulate fat cell lipolysis and/or apoptosis. They used extracorporeal resources to help in weight loss and reduction of comorbidities associated with the disease. 19-21
According to Loap and Lathe, 2018, cryotherapy was one of the first resources to be investigated for obesity treatment because adipocytes are more sensitive to cold. When in contact with low temperatures (-5ºC), lipids undergo crystallization and consequent inflammatory reaction, generating cell death via apoptosis and even necrosis. It leads to a decrease in subcutaneous tissue for weeks to months without damaging the skin and metabolism. Thus, the first cryolipolysis equipment appeared, allowing adipose tissue cooling by extracting temperature and stimulating the adipocyte death process. 20-21
Such as cryolipolysis, several other resources, such as focused ultrasound and radiofrequency, have scientific evidence proving their effects on the extracorporeal stimulus of fat cell lipolysis and/or apoptosis without damaging the metabolism. Therefore, ESWT technology has also been adapted for the same therapeutic purpose. 21-23
ESWT produces high-intensity mechanical energy that leads to the activation of mechanotransduction signal and cellular mobilization. It responds to cavitation’s indirect effect, a phenomenon known for forming gaseous microbubbles in a fluid medium. There are two types of cavitation: stable, where these microbubbles are formed and do not undergo implosion; and unstable, where microbubbles implosion occurs. Each cavitation type has an intensity of physiological action. The stable cavitation can stimulate the lipolysis process, while the unstable cavitation can cause cell death. The present study showed that its physiological stimulus could occur through the biological process of apoptotic lipolysis. 7, 24-26
We demonstrated that ESWT-treated tissue showed a significant increase in Caspase-3 and Cleaved Caspase-3 positive fat cells. Both extrinsic (mediated by cellular receptors) and intrinsic pathways (mitochondrial) activate Caspase-3 in the apoptotic cell.24 Thus, the expression of caspase-3 in adipose tissue indicates that ESWT can activate apoptotic pathways and, consequently, stimulate the lipolysis process. These results agree with previously published studies. 27-30
The present study also showed that, in tissues treated with ESWT, there was an increase in CD68+ macrophages, mainly in adipose tissue adjacent areas. Macrophages play a central role in the lipolysis process. Their presence indicates inflammation during autophagic lipolysis, that is, during the mechanism of cell self-destruction via apoptosis, a well-recognized and scientifically established process. 31- 33
This evidence shows that ESWT can stimulate fat cell death and consequent lipolysis. Such ability correlates with the energy dose used during the procedure. Our study used a dose of 180 mJ with a stainless steel tip of 15 mm, generating a high concentration of mechanical energy in the treatment area and promoting unstable cavitation. Thus, the damage is more significant, leading to cell morphological changes, cell membrane rupture, and consequent fat cell apoptosis and lipolysis.34,35
It is important to note that other biological processes are also associated with autophagic lipolysis, such as necrosis and autophagy due to other mechanisms. Thus, it is essential to study different processes to clarify the exact action of EWST during apoptosis and lipolysis. 31-33
Another interesting finding that confirms the presence of autophagic lipolysis is the presence of positive cells for HSL and adipophilin in adjacent adipose tissue areas. HSL is an enzyme present in adipocyte metabolism, which breaks down triacylglycerides (TAG) when activated. This positive marker in adipose tissue indicates when there is a lipolysis process. Thus, we can say that ESWT stimulates lipolysis of the fat cell in the apoptotic pathway. 36,37
Adipophilin is one of the main proteins induced in the early stages of adipocyte differentiation. Also, this protein plays a vital role in the metabolism of fatty acids, cholesterol, and neutral lipids storage. Both markers, mainly expressed in inflammatory cells adjacent to the ESWT intervention group’s fatty tissue, demonstrate a phagocytosis process of the lipid droplets confirming the process of autophagic lipolysis. 31
Assuming that ESWT can perform unstable cavitation and before this phenomenon, we have stable cavitation in a liquid medium, we can infer that ESWT stimulates apoptosis through unstable cavitation in a concentrated area. Consequently, the mechanical wave is dissipated to a lesser extent around the area that received the treatment. These regions receive the stable cavitation stimulus that generates the lipolysis process.7,10
Our result corroborates with clinical studies, which showed that ESWT could reduce adipose tissue thickness and, consequently, decrease the body circumference of regions that have undergone treatment. The studies reported that an average of 6 to 12 therapy sessions with high energies (150 mJ to 200 mJ) was necessary to validate the results. However, the authors did not demonstrate which were the pathways of physiological stimulation of ESWT. Thus, this is the first study that confirms the real physiological effect of the therapy on the fat cell.
Obesity is a chronic low-level inflammatory condition. Such phenotype is a risk factor in the etiology of cardiovascular diseases, type 2 diabetes mellitus, cancers, and associated metabolic diseases. However, the inflammatory process observed in individuals with obesity differs from the classic inflammatory response in other circumstances, as it is a systemic inflammatory process.4,6 The present study shows it because it did not present inflammatory infiltrates and positivity of the evaluated markers in the control sample’s adipose tissue analysis, as they are not specific markers in obesity disease.
Altogether, data from the present study demonstrate that ESWT treatment favors fat cell death and breakdown. One hypothesis would be that the therapy could also lead to the prevention or reduction of systemic inflammation caused by obesity since it leads to a decreased number of fat cells. Consequently, we would have less risk in the development of comorbidities such as insulin resistance. Because of the clinical evidence about ESWT, researchers report that this is a safe therapy, as supported in the present study, once we reported minimal adverse events and that resolved right after the first treatment sessions.
Given the evidence present in this study, ESWT can be safely used to reduce adipose tissue in individuals with obesity. It can stimulate cell metabolism, generating apoptosis in the area of ¿¿energy concentration and fat cells autophagic lipolysis. This finding in the immunohistochemical analysis proves the results of clinical studies of adipose tissue reduction. Thus, this therapy aims at assisting the conservative and even preventive obesity treatment.
It is possible to conclude from our results that ESWT causes adipose tissue apoptosis with consequent autophagic lipolysis in obese individuals. Thus, ESWST can be considered a useful, safe, and promising adjuvant therapy for reducing adipose tissue and, consequently, preventing and/or treating obesity.
Débora Aparecida Oliveira Modena | 0000-0002-2800-3620
Statistical analysis; approval of the final version of the manuscript; study design and planning; preparation and writing of the manuscript; data collection, analysis, and interpretation; active participation in research orientation; intellectual participation in propaedeutic and/or therapeutic conduct of studied cases; critical literature review; critical revision of the manuscript.
Renata Michelini Guidi | 0000-0002-2800-3620
Critical literature review; critical revision of the manuscript.
Ciro Dantas Soares | 0000-0002-6861-6640
Statistical analysis; data collection, analysis, and interpretation; critical literature review.
Everton Cazzo | 0000-0002-5804-1580
Statistical analysis; approval of the final version of the manuscript; study design and planning; preparation and writing of the manuscript; data collection, analysis, and interpretation; active participation in research orientation; intellectual participation in propaedeutic and/or therapeutic conduct of studied cases; critical literature review; critical revision of the manuscript.
Elinton Adami Chaim | 0000-0003-4627-0631
Statistical analysis; approval of the final version of the manuscript; study design and planning; preparation and writing of the manuscript; data collection, analysis, and interpretation; active participation in research orientation; intellectual participation in propaedeutic and/or therapeutic conduct of studied cases; critical literature review; critical revision of the manuscript.
1. Arroyo-Johnson C, Mincey KD. Obesity Epidemiology Worldwide. Gastroenterol Clin North Am. 2016;45(4):571-9.
2. Blüher M. Obesity: global epidemiology and pathogenesis. Nat Rev Endocrinol. 2019;15(5):288-98.
3. Shah R, Gayat E, Januzzi JL Jr, Sato N, Cohen-Solal A, diSomma S, et al. Body mass index and mortality in acutely decompensated heart failure across the world: a global obesity paradox. J Am Coll Cardiol. 2014;63(8):778-85.
4. Cazzo E, Ramos AC, Chaim EA. Bariatric surgery offer in Brazil: a macroeconomic analysis of the health system's inequalities. Obes Surg. 2019;29(6):1874-80.
5. Hofmann B. Obesity as a socially defined disease: philosophical considerations and implications for policy and care. Health Care Anal. 2016;24(1):86-100.
6. Jimenez LS, Mendonça Chaim FH, Mendonça Chaim FD, Utrini MP, Gestic MA, Chaim EA, et al. Impact of weight regain on the evolution of non-alcoholic fatty liver disease after roux-en-Y gastric bypass: a 3-year follow-up. Obes Surg. 2018 ;28(10):3131-5.
7. Modena D, Silva CN, Grecco C, Guidi RM, Moreira RG. Coelho AA, et al. Extracorporeal shockwave: mechanisms of action and physiological aspects for cellulite, body shaping, and localized fat Systematic review. J Cosmet Laser Ther. 2017;19(6):314-9.
8. Knobloch K, Kraemer R. Extracorporeal shock wave therapy (ESWT) for the treatment of cellulite. A current metaanalysis. Int J Surg. 2015;24:210-7.
9. Modena D, Silva CN, Delinocente PCT, Araujo BT, Carvalho MT, Grecco CM. Shock wave therapy associated with radio frequency in the treatment of abdominal skin flaccidity. J Dermat Cosmetol. 2019;3(3):69-73.
10. Hexsel D, Camozzato FO, Silva AF, Siega C, Camozzato FO. Acoustic wave therapy for cellulite, body shaping and fat reduction. J Cosmet Laser Ther. 2017;19(3): 165-73.
11. Morigny P, Houssier M, Mouisel E, Langin D. Adipocyte lipolysis and insulin resistance. Biochimie. 2016;125:259-66.
12. Ross SM. Obesity and metabolic syndrome: a complementary and integrative health approach. Holist Nurs Pract 2017;31:348-352; Engin A. The definition and prevalence of obesity and metabolic syndrome. Adv Exp Med Biol 2017;960:1-17.
13. Cohen P, Spiegelman BM. Cell biology of fat storage. Mol Biol Cell. 2016;27(16):2523-7.
14. Bolsoni-Lopes A, Alonso-Vale MI. Lipolysis and lipases in white adipose tissue - An update. Arch Endocrinol Metab. 2015;59(4):335-42.
15. Braun K, Oeckl J, Westermeier J, Li Y, Klingenspor M. Non-adrenergic control of lipolysis and thermogenesis in adipose tissues. J Exp Biol. 2018;221(Pt Suppl 1):jeb165381.
16. Hersoug LG, Møller P, Loft S. Role of microbiota-derived lipopolysaccharide in adipose tissue inflammation, adipocyte size and pyroptosis during obesity. Nutr Res Rev. 2018;31(2):153-63.
17. Elmore S. Apoptosis: a review of programmed cell death. Toxicol Pathol. 2007;35(4):495-516.
18. REF Adipose cell apoptosis: death in the energy depot, Int J Obes Relat Metab Disord 2000;24(Suppl 4):S3-7.
19. D'Arcy MS. Cell death: a review of the major forms of apoptosis, necrosis and autophagy. Cell Biol Int. 2019;43(6):582-92.
20. Loap S, Lathe R. Mechanism underlying tissue cryotherapy to combat obesity/overweight: triggering thermogenesis. J Obes. Epub 2018 May 2.
21. Peterson JD, Goldman MP. "Laser, light, and energy devices for cellulite and lipodystrophy," Clin Plast Surg. 2011;38(3):463-74.
22. Blondin DP, Labbe SM, Tingelstad HC, et al. "Increased ´ brown adipose tissue oxidative capacity in cold-acclimated humans," J Clin Endocrinol Metabol. 2014;99(3):E438-46.
23. Notarnicola A, Moretti B. The biological effects of extracorporeal shock wave therapy (eswt) on tendon tissue. Muscles Ligam Tendons J. 2012;2(1):33-7.
24. Wang C. Extracorporeal shockwave therapy in musculoskeletal disorders. J Orthop Surg Res. 2012;7(1):7-11.
25. Schlaudraff KU, Kiessling MC, Császár NBM, Schmitz C. Predictability of the individual clinical outcome of extracorporeal shock wave therapy for cellulite. Clin Cosmet Invest Dermatol. 2014;7:171-82.
26. Adipose cell apoptosis: death in the energy depot, Int J Obes Relat Metab Disord 2000;24(Suppl 4):S3-7.
27. Prins JB, O'Rahilly S. Regulation of adipose cell number in man. Clin Sci 1997; 92:3-11.
28. Crowley LC, Waterhouse NJ. Detecting cleaved caspase-3 in apoptotic cells by flow cytometry. Cold Spring Harb Protoc. Epub 2016 Nov.
29. Cingolani F, Czaja MJ. Regulation and functions of autophagic lipolysis. Trends Endocrinol Metab. 2016;27(10):696-705.
30. Kim SJ, Feng D, Guillot A, et al. Adipocyte death preferentially induces liver injury and inflammation through the activation of chemokine (C-C Motif) Receptor 2-positive macrophages and lipolysis. Hepatology. 2019;69(5):1965-82.
31. Huang SC, Everts B, Ivanova Y, et al. Cell-intrinsic lysosomal lipolysis is essential for alternative activation of macrophages. Nat Immunol. 2014;15(9):846-55.
32. Steinbach P, Hofstaedter F, Nicolai H, Roessler W, Wieland W. Determination of the energy-dependent extent of vascular damage caused by high-energy shock waves in an umbilical cord model. Urol Res. 1993;21:279-82.
33. Kuhn C. Impact of extracorporeal shock waves on the human skin with cellulite: A case study of an unique instance. Clin Interv Aging. 2008;3(1):201-10.
34. Steinberg D, Khoo JC. Hormone-sensitive lipase of adipose tissue. Fed Proc.1977;36(7):1986-90.
35. Haemmerle G, Zimmermann R, Zechner R. Letting lipids go: hormone-sensitive lipase. Curr Opin Lipidol. 2003;14(3):289-97.
 All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773
All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773



 Read in Portuguese
Read in Portuguese
 Portuguese PDF
Portuguese PDF
 Print
Print
 Send this article by email
Send this article by email
 How to cite this article
How to cite this article
 Submit a comment
Submit a comment
 Mendeley
Mendeley
 Pocket
Pocket
{kind=link}
{kind=link}
{kind=link}