


Manoella Freitas Santos; Ana Claudia Dal Magro; Thaís Furtat Marques; Fernando Eibs Cafrune
Received on: 08/09/2020
Approved on: 26/11/2020
Financial support: None
Conflict of interest: None
Study conducted at the Santa Casa de Misericórdia de Porto Alegre, Porto Alegre (RS), Brazil
Acknowledgments: We thank the professors, colleagues and patients who made this study possible.
INTRODUCTION: Mohs micrographic surgery (MMS) can achieve high cure rates in skin cancer treatment and remove as little healthy tissue as possible.
OBJECTIVE: This study aims to characterize patients undergoing Mohs micrographic surgery and to assess predictive factors for a higher number of surgical phases.
METHODS: Observational, cross-sectional, retrospective, and descriptive study conducted in a reference service for micrographic surgery from 2013 to 2019. The medical records of 230 patients (256 lesions) were reviewed.
RESULTS: Injuries with recurrence had significantly more stages than injuries without recurrence (1.69 stages versus 1.31 stages). Tumors greater than 2 cm had a greater number of phases than those smaller than 1 cm and between 1.1 and 2.2 cm (2.0 versus 1.08 and 1.22, respectively). When comparing the locations of the lesions with the number of phases, there was no significant difference. There was a considerable difference regarding the preoperative histological subtypes: aggressive basal cell carcinomas (BCC) required a higher number of phases than non-aggressive BCCs.
CONCLUSIONS: Our study demonstrates, corroborating data from the literature, that the risk factors described are directly related to a greater number of stages of Mohs micrographic surgery.
Keywords: Mohs Surgery; Skin Neoplasms; Carcinoma, Basal Cell; Carcinoma, Squamous Cell Surg Cosmet
Frederic Mohs developed the Mohs technique in the 1930s, initially applying zinc chloride to the tumor lesions. It fixed the tissue in vivo and allowed its subsequent analysis under a microscope to preserve the tumor morphology and histological structure.1 With the evolution of the technique, there was a change to the analysis of fresh tissue by freezing, consisting of the excision of tissue layers compromised by the neoplasm. The tissue is examined using special stains of horizontal cuts to evaluate the tumors’ peripheral and deep margins microscopically.1,2,3,4,5,6 The process of tumor removal and microscopic analysis after freezing the piece is called the surgical phase. Several stages may be necessary to remove the tumor entirely, increasing the surgery’s time and cost.2,3
In Brazil, Mohs micrographic surgery (MMS) is still underutilized due to the need for additional specialized training and the long learning curve of the method, restricting its availability to larger centers. Although many therapeutic options are currently available, conventional surgical excision (SE) is still the most common treatment for non-melanoma skin cancer (NMSC). The main difference between the two treatments is the method of examining the histological margin. The standard SE exams the surgical margins mainly in random vertical sections, the so-called “bread loaf” technique.7 Moreover, the MMS flats and cuts the sample horizontally. It offers the possibility to examine 100% of the resection margins compared to the small percentage of margin control in the SE, generally 0.01% to 1.0% of the total surgical margin.2,3,7 MMS is the method that has the highest cure rates for the treatment of NMSC and allows the preservation of maximum peritumoral healthy tissue.7.8
Mohs micrographic surgery is a great therapeutic option for treating malignant skin neoplasms such as squamous cell carcinoma (SCC) and basal cell carcinoma (BCC).6 It can achieve high cure rates in the treatment of skin cancer, preserving maximum healthy tissue, and, as a consequence, provide less functional and cosmetic damage.2,3 The main indications in the literature are recurrent neoplasms, aggressive subtypes of skin cancer, and neoplasms in anatomical sites with high recurrence rates.2,9 Mortality related to non-melanoma skin carcinomas is low due to the small percentage of metastatic disease. However, morbidity can be high due to local tissue destruction, mainly because most tumors occur in areas such as the head and neck.7
Currently, there is a trend to treat an increasing number of tumors, mainly primary SCCs and BCCs, with MMS. Indications include those primary tumors that, due to their large size or location in specific anatomical sites, present an increased risk of recurrence. It is also recommended to treat tumors in places that generate significant aesthetic damage, where it is necessary to save more healthy tissue.2,9 Likewise, neoplasms not previously treated, located in critical locations, such as the eyelid or lip, benefit from the tissue-sparing aspects of the Mohs technique.9 Since most BCCs are quite limited, most primary BCCs should be removed with MMS in the first two stages. However, there is a significant subset of primary tumors that require more steps to achieve a tumor-free plane. We studied the histological subtype of these tumors, and their depth, to determine whether we could use these resources to predict which primary BCC or SCC would be more challenging to remove with free margins in conventional surgery.8.9
The study’s main objective was to analyze preoperative characteristics of tumors treated with Mohs micrographic surgery associated with two or more surgical stages. This retrospective analysis of patient records identifies histological subtypes, size, and recurrences of skin tumors treated with MMS, and it studies their correlation with the largest number of stages during surgery. The second objective was to identify predictive factors for high-risk BCCs, eligible and treated with MMS, which have widespread subclinical tumor dissemination.
This is an observational, cross-sectional, retrospective, and descriptive study. We retrospectively retrieved the medical records of 230 patients (256 lesions) treated with Mohs micrographic surgery at a referral hospital in dermatology in Porto Alegre between 2013 and 2019. The sample consisted of all patients treated during this period by the team. Data were obtained by analyzing medical records and filling in a standardized table containing sex, age, histopathological diagnoses, tumor location and size, history of previous treatments, number of surgical phases, and reconstruction type. After collection, we assessed the data to group information characterizing these patients’ clinical, epidemiological, and histopathological profiles.
Statistical data were described in frequency, percentage, average, and standard deviation. The average number of phases was analyzed using t-test or ANOVA with Tukey multiple comparison test. The analyses were performed using the SPSS version 25 software, and p<0.05 were considered significant.
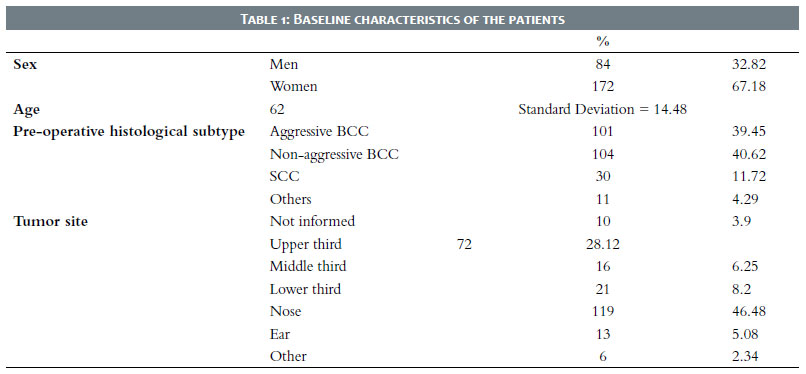
We assessed the medical records of 230 patients. A total of 256 lesions were treated with MMS. Table 1 describes the baseline characteristics of patients. The few cases with incomplete data had the missing aspect excluded from the analysis. Individuals had a mean age of 62 years, with a standard deviation of 14.48 years. Of 256 patients, 172 were women, and 84 were men.
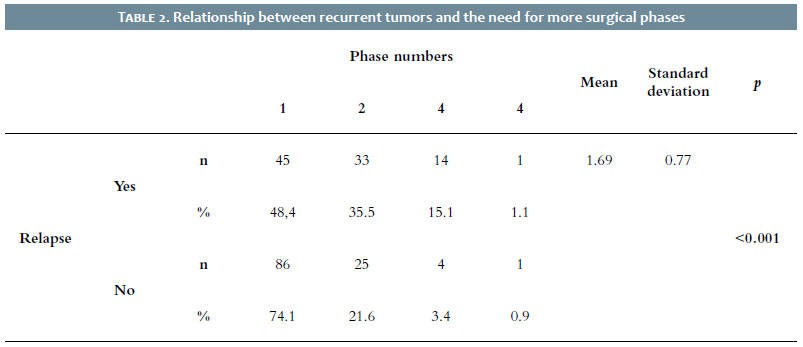
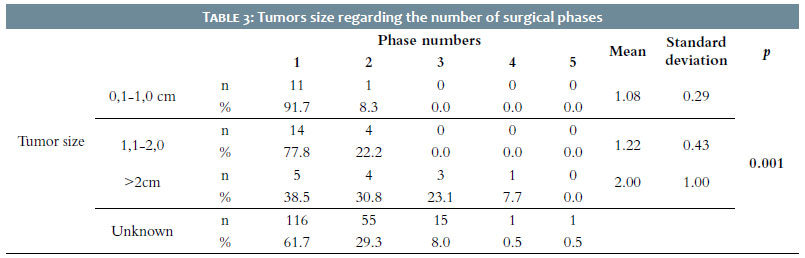
Regarding recurrence, the study categorized 93 injuries as recurrence and 116 as primary injuries. When comparing the number of surgical phases, recurrent lesions had a significantly higher number of stages than primary lesions (1.69 ± 0.77 versus 1.31 ± 0.58 phases, respectively) (Table 2). Concerning the tumor’s size, 12 lesions measured 0.1 cm to 1 cm, 18 lesions measured between 1.1 cm and 2 cm, and 13 lesions measured more than 2 cm. The medical record didn’t describe the size of 188 lesions. Of these, 116 were excised in the first phase of surgery and 55 in the second phase. Tumors over 2 cm had a significantly greater number of phases than those with a size less than 1 cm and between 1.1 and 2.20 cm (2±1 versus 1.08±0.29 and 1.22±0.43 phases, respectively), according to Table 3.
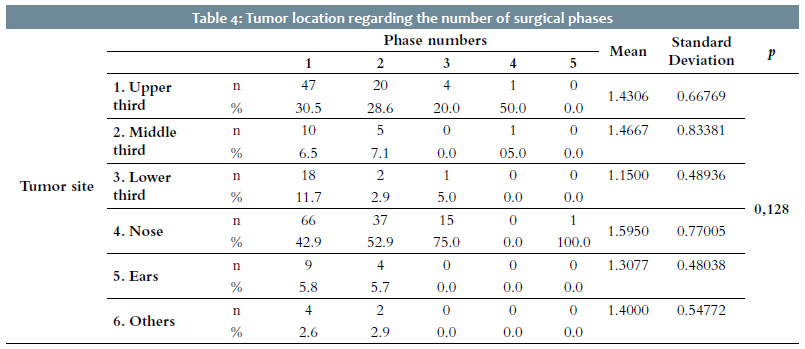
Lesion sites were divided into upper third (72 lesions), middle third (16 lesions), and lower third (21 lesions) of the face, nose (119 lesions), ears (13 lesions), and others (6 lesions), which included all other neoplasms not located on the face. When comparing the sites with the number of phases, there was no significant difference (p = 0.128) (Table 4).
Histopathological subtypes were grouped into aggressive BCC (sclerodermiform, micronodular, infiltrated, and basal squamous subtypes), non-aggressive BCC (nodular and superficial subtypes), SCC (invasive and in situ), and dermatofibrosarcoma. They were also classified according to anatomopathology, categorizing no tumor cells found after the initial biopsy as without residual tumor.
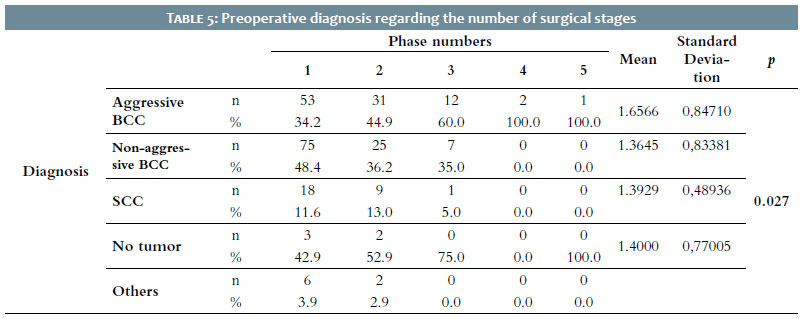
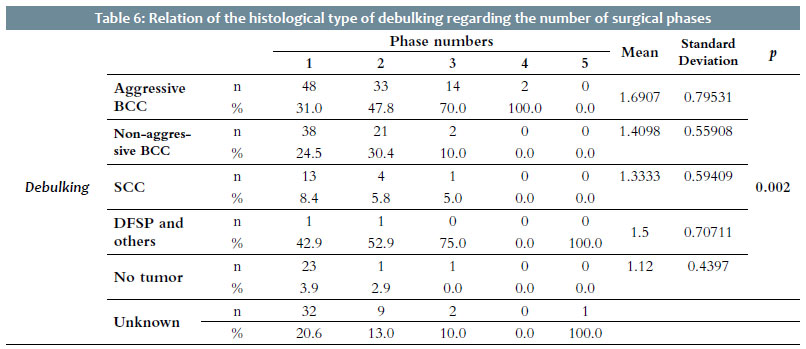
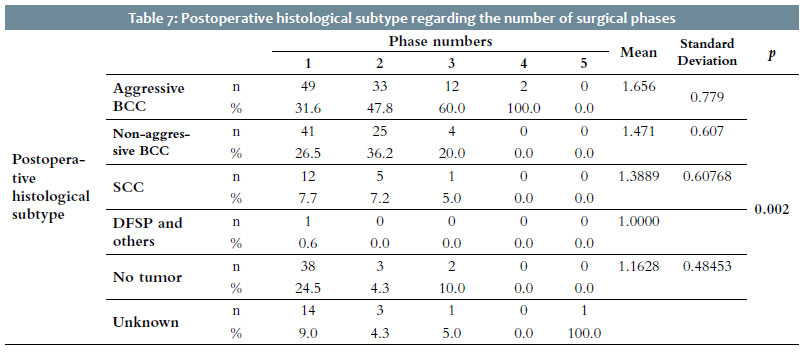
The preoperative diagnoses analysis compared to the number of phases showed a significant difference: the aggressive BCC had more phases than the non-aggressive BCC (p=0.027) (Table 5). Among the injuries analyzed, 99 were diagnosed with aggressive BCC, 107 were non-aggressive BCC, and 28 were SCCs. The assessment of the histological subtypes of debulking compared to the number of phases demonstrated a significant difference: the aggressive BCC (n=97) had more stages than those without residual tumor (n=25; p=0.002) (Table 6). Furthermore, the evaluation of the postoperative histological subtypes compared to the number of phases presented a significant difference: aggressive BCC (n=96) had more stages than those without tumor (n=43; p=0.002) (Table 7).
Aggressive subtypes, grouped in this study as infiltrative, sclerodermiform, basal-squamous, and micronodular, were found more frequently when more than one Mohs stage was needed, with statistical significance. The most aggressive subtypes of BCC require more MMS stages to obtain tumor-free margins, which is consistent with the concept that these subtypes generally require more aggressive treatment from the start. Weinstein et al.10 also corroborated these findings, concluding that tumors with aggressive subtypes commonly present a subclinical extension that is challenging to evaluate properly. It hampers the analysis of margins in the conventional technique.11
We believe that the anatomopathological exams “without tumor” when debulking MMS are predominantly non-aggressive tumors, as we didn’t find them in the postoperative sample. Also, we believe that in these cases, they could be small, well-defined tumors in which the initial biopsy may have been sufficient to obtain tumor-free margins.
Incisional punch biopsies are commonly used to confirm the clinical diagnosis of NMSC and determine the histopathological subtype before surgical excision. Preoperative biopsies can also coincide with the scar site or previously treated area without establishing an accurate diagnosis. The sample variations in preoperative biopsies could lead to a different interpretation of the histological subtype.15 There is significant variability in the literature regarding the percentage of concordance between the histological diagnosis of incisional biopsies and the histological diagnosis found with complete excision of the tumor.15 Previous studies have shown a moderate agreement ranging from 51.1% to 82% between the NMSC subtype in incisional biopsies and subsequent surgical excision. (15.16)
As for the histological type of the studied tumors, BCCs represented 67.2% of the sample and SCC, 7.89%. Data from the literature7,10,14 indicate BCC as the more common type of skin cancer. Also, aggressive BCCs, relapsed and in high-risk areas, constitute one of the main indications for MMS, thus justifying their high prevalence in this series.
Mohs micrographic surgery avoids unnecessary excision of uninvolved tissue, allowing better preservation of function and cosmetics. Compared with other treatment modalities, it has the highest cure rates in five years, ranging from 94% to 99% for primary BCCs and from 90% to 96% for recurrent BCCs.11 Previous studies (with different excision margins and indication criteria) found that between 28% and 45% of BCCs treated with MMS were excised entirely in the first stage, suggesting that the use of MMS eligibility criteria could be worthy.11
According to a study by Van Loo et al.7, the accumulated probability of recurrence in 10 years for both recurrent or primary BCCs ranges from 3.9-4.4% after MMS to 12.2-13.5% after conventional surgery. Of all recurrences, 44.0% were recorded in the first five years after treatment, 40.0% between five and ten years after treatment, and 16.0% after ten years of follow-up. It demonstrates that even in long-term follow-up, neoplasms excised by the Mohs technique have fewer recurrences.
Due to the absence of tumor size description in the medical record of most cases in this study, only 43 lesions were analyzed by tumor size. It is a common bias in retrospective, observational studies. Despite this, we found that tumor sizes >2 cm had a significantly higher number of phases than lesions <1.0 cm and 1.1-2.0 cm (2.0±1 versus 1.08±0.29 and 1.22±0.43 phases, respectively), which is compatible with the finding in the literature.2.3
As demonstrated in this study, skin neoplasms larger than 2 cm present a higher risk of recurrence if not adequately addressed. Therefore, MMS could be indicated in these cases, especially in tumors with aggressive histological subtypes or high-risk locations.
The aggressive BCC subtypes found in this study needed more stages for tumor clearance with statistical significance (p=0.002). It also agreed with the findings of other studies.2,9,11
When comparing the anatomical sites with the number of phases, our study showed no significant difference, differing from other studies. Alam et al. demonstrated in their case series that lesions in the nose and ear required more surgical stages than tumors in other extra-facial locations. Flohil et al.11 described that BCCs located in the H zone of the face were 51% more likely to require several MMS stages than BCCs in other locations. We believe that we found no statistical difference for the anatomical site due to the predominance of nasal lesions and our sample size.
According to data from the international literature, men are predominant. In our sample, we obtained a predominance of women in 66.79% of the cases. We emphasize that our study assessed patients who underwent MMS in a particular scope. Also, the sample was non-random and with a limited number of patients (n=230), not representing all the population. The average age found was 61.54 years (24 to 94 years).
The study categorized 93 injuries as recurrent (40.4%) and 116 as primary (50.43%). When comparing the number of surgical phases, lesions with recurrence had significantly more numbers than lesions without recurrence (1.69 versus 1.31, respectively). Such data also agree with previous studies,2,7,8,11 including MMS indication as another standard for recurrent tumors.
When analyzing the preoperative, debulking, and postoperative diagnosis compared to the number of stages, there was a significant difference. More surgical phases were necessary for aggressive BCC treatment in all analyses than for non-aggressive BCCs or samples without tumors (p<0.05).
Aggressive BCC subtypes often required more than one Mohs stage to obtain free margins. Our study demonstrated, confirming the literature data, that tumor size, recurrence, and histological subtype are related to a higher number of stages in Mohs surgery. It concluded that the risk factors described are directly associated with a more significant number of Mohs micrographic surgery stages, that is, higher subclinical growth of tumors. These data are relevant in the patient’s initial assessment and can help decide the appropriate conduct for each case.
Manoella Freitas Santos | 0000-0002-5024-5976
Statistical analysis; approval of the final version of the manuscript; study design and planning; preparation and writing of the manuscript; data collection, analysis, and interpretation; active participation in research orientation; intellectual participation in propaedeutic and/or therapeutic conduct of studied cases; critical literature review; critical revision of the manuscript.
Ana Claudia Dal Magro | 0000-0001-5472-4539
Approval of the final version of the manuscript; study design and planning; preparation and writing of the manuscript; data collection, analysis, and interpretation; critical literature review; critical revision of the manuscript.
Thaís Furtat Marques | 0000-0001-6676-5872
Study design and planning; preparation and writing of the manuscript; data collection, analysis, and interpretation; critical literature review; critical revision of the manuscript.
Fernando Eibs Cafrune | 0000-0002-6645-0122
Approval of the final version of the manuscript; study design and planning; preparation and writing of the manuscript; data collection, analysis, and interpretation; active participation in research orientation; intellectual participation in propaedeutic and/or therapeutic conduct of studied cases; critical literature review; critical revision of the manuscript.
1. Mohs FE. Chemosurgical treatment of cancer of the ear: a microscopically controlled method of excision. Surgery. 1947;21(5):605-22.
2. Chagas FSC, Silva BS. Cirurgia micrográfica de Mohs: estudo de 83 casos. An Bras Dermatol. 2012;87(2):204-10.
3. Wong E, Axibal E, Brown M. Mohs micrographic surgery. Facial Plast Surg Clin. 2019,27(1):15-34.
4. Mariwalla K, Aasi SZ, Glusac EJ, Leffell DJ. Mohs micrographic surgery histopathology concordance. J Am Acad Dermatol. 2009;60(1):94-8.
5. Semkova K, Mallipeddi R, Robson A, Palamaras I. Mohs micrographic surgery concordance between Mohs surgeons and dermatopathologists. Dermatol Surg. 2013;39(11):1648-52.
6. Bobotsis R, Guenther L. How mohs surgery transformed into a first-line treatment of skin cancer. J Cutan Med Surg. 2017;21(1):40-1.
7. Van Loo E, Mosterd K, Krekels GA, Roozeboom MH, Ostertag JU, Dirksen CD, et al. Surgical excision versus Mohs' micrographic surgery for basal cell carcinoma of the face: a randomised clinical trial with 10 year follow-up. Eur J Cancer. 2014;50(17): 3011-20.
8. Terzian LR, Festa Neto C, Pimentel ERA. Fatores preditivos do maior número de estádios na cirurgia micrográfica de Mohs para o tratamento do carcinoma espinocelular da cabeça. An Bras Dermatol. 2008;83(3):221-6.
9. Orengo IE, Salasche SJ, Fewkes J, et al. Correlation of hystologic types of primary basal cell carcinoma and number of Mohs stages required to achieve a tumor-free plane. J Am Acad Dermatol 1997;37:395-7.
10. Weinstein MC, Brodell RT, Bordeaux J, Honda, K. The art and science of surgical margins for the dermatopathologist. Am J Dermatopathol. 2012;34(7):737-45.
11. Flohil SC, van Dorst AMJM, Nijsten T, Martino Neumann HÁ, Munte K. Mohs micrographic surgery for basal cell carcinomas: appropriateness of 'Rotterdam' criteria and predictive factors for three or more stages. J Eur Am Dermatol Venereol. 2013;27: 1228-35.
12. Alam M, Berg D, Bhatia A, Cohen JL, Hale EK, Herman AR, et al. Association between number of stages in Mohs micrographic surgery and surgeon-, patient-, and tumor-specific features: A cross-sectional study of practice patterns of 20 early- and mid-career Mohs surgeons. Dermatol Surg. 2010;36(12):1915-20.
13. Zabielinski M, Leithauser L, Godsey T, Gloster Jr HM. Laboratory errors leading to nonmelanoma skin cancer recurrence after Mohs micrographic surgery. Dermatol Surg. 2015;41(8):913-16.
14. Samarasinghe V, Madan V. Nonmelanoma skin cancer. J cutan aesthet surg. 2012; 5(1):3.
15. Cortés-Peralta E.C, Ocampo-Candiani J, Vázquez-Martínez OT, Gutiérrez-Villarreal IM, Miranda-Maldonado I, Garza-Rodríguez V. Correlation between incisional biopsy histological subtype and a Mohs surgery specimen for nonmelanoma skin cancer. Actas Dermo-Sifiliográficas (English Edition). 2018;109(1):47-51.
16. Izikson L, Seyler M, Zeitouni NC. Prevalence of underdiagnosed aggressive non-melanoma skin cancers treated with Mohs micrographic surgery: analysis of 513 cases. Dermatol surg. 2010;36(11):1769-72.
 All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773
All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773



 Read in Portuguese
Read in Portuguese
 Portuguese PDF
Portuguese PDF
 Print
Print
 Send this article by email
Send this article by email
 How to cite this article
How to cite this article
 Submit a comment
Submit a comment
 Mendeley
Mendeley
 Pocket
Pocket
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}