


Natacha Quezada Gaón; Maria Isabel Herane Herane; Mathias Yagnam Diaz; Marlene Waissbluth Morales
Received on: 08/11/2020
Approved on: 26/11/2020
Financial support: None
Conflict of interest: None
Study conducted at the Department of Dermatology, Pontificia Universidad Católlica de Chile, Dermatoplasty Study Group
Acknowledgment: We thank the study group
INTRODUCTION: Facial erythema is a frequent and often distressing complaint in patients with rosacea. Botulinum toxin has been proposed as a treatment of facial erythema with relatively good results.
OBJECTIVE: This study aims to assess botulinum toxin’s safety and efficacy in a split-face trial in two different administration modalities: intradermal injections on one side of the face and facial electroporation on the other side.
MATERIALS AND METHODS: The trial enrolled 20 subjects aged between 25 and 75 years with erythematotelangiectatic rosacea. Subjects received five units of Botulinum toxin through intradermal injections on the right side of the face. The same amount was introduced through electroporation technique on the left side. We conducted the evaluation using a standardized erythema grading system (System Vectra) and digital photographs at baseline, 2, 6, and 12 weeks.
RESULTS: The effectiveness in reducing the erythema of botulinum toxin with both the injection and electroporation was evident from the second week and persisted until week 12. Both techniques were effective.
CONCLUSIONS: Intradermal injection of botulinum toxin and electroporation seems both effective and safe for treating erythema related to rosacea. The mechanism of action is still controversial.
Keywords: Erythema; Mesotherapy; Botulinum Toxins, Type A
Rosacea is a chronic inflammatory condition of the face with several clinical symptoms, such as transient and persistent erythema, telangiectasias, inflammatory papules, pustules, plaques, nodules, and pimples, and may have ocular involvement.1
Four subtypes were defined based on clinical characteristics: subtype I or erythematotelangiectatic rosacea (ETR), which includes individuals prone to flushing associated with persistent erythema with frequently telangiectasias; subtype II or papulopustular rosacea (PPR), characterized by a central facial eruption of multiple erythematous papules or small pustules, isolated or in groups, and the occasional presence of plaques and nodules; subtype III or phymatous rosacea, described as thickening of the skin with irregular contours (phymas) and preference for the ears (otophyma), eyelids (blepharophyma), chin (gnatophyma), forehead (metophyma), and nose (rhinophyma). The latter form is the most common and is present mainly in men. Finally, there is subtype IV, or ocular rosacea, characterized by multiple and non-specific signs, such as itching, dry eye sensation, blepharitis, sty, and chalazion. It can occur without cutaneous manifestation or associated with other subtypes.1-3
The exact pathogenesis of rosacea is still unknown. The literature reports some factors relevant to its occurrence, such as innate immune system dysfunction, ultraviolet radiation exposure inducing increased angiogenesis, reactive oxygen species (ROS) production, vascular changes with increased expression of vascular endothelial growth factor (VEGF), epidermal barrier dysfunction, and neurogenic inflammation with release of neuromediators at the inflammation site resulting in vasodilation.
The inflammatory cell recruitment, the plasma proteins extravasation, the microbial action through the activation of toll-like 2 receptors and mast cells, and the persistent cytokines and chemokines release intensify the inflammation and increase innate immune responses. In short, it is a chronic and persistent inflammatory state.5
Several treatments have been proposed for rosacea, including oral and topical therapies in association with lasers, intense pulsed light (IPL), photodynamic therapy, etc.6 Erythema treatment is challenging. Different drugs have been used, such as oral beta-blockers, botanical products, and topical products such as ivermectin, azelaic acid, brimonidine, oxymetazoline, tranexamic acid, in addition to the use of laser, IPL, and even endoscopic thoracic surgery with sympathectomy, in general with partial results.7
Botulinum toxin (BT) has become another alternative treatment for refractory erythema and rosacea flushing.9 Dayan et al. observed that patients undergoing BT rejuvenation treatment improved skin quality as well as wrinkles and decreased duration of erythema and flushing.10 Since then, several reports of BT treatments in rosacea subtypes I or II have been published using intradermal injections in the affected regions.11 As this procedure requires an injectable technique, we present the results of a group of treated patients in a split-face study. The group received BT by intradermal injections on one side of the face and the same number of BT units by the facial electroporation technique on the contralateral side.
This study aims to observe BT type A’s efficacy in the treatment of erythema of erythematotelangiectatic rosacea.
The study recruited men and women with facial erythema associated with mild to moderate erythematous rosacea and some cases with few papules and pustules recruited the authors’ private clinic.
The inclusion criteria were patients aged 25 to 75 years old, with Fitzpatrick skin phototype I to IV, non-smokers in the last two years, with erythematotelangiectatic or papulopustular rosacea (up to two-four inflammatory lesions), bilateral involvement in the cheeks, and availability to meet all follow-up requirements.
We excluded individuals with any other dermatological disease on the face, human immunodeficiency virus, and hepatitis; with immunological suppression, myopathies, or neurodegenerative diseases; pregnancy, lactation, oral treatment with vasoconstrictors, vasodilators, or isotretinoin in the last 12 months; allergy to cow protein, known hypersensitivity to BT or any of its ingredients, or even if they had received BT applications on the face up to 12 months before. Individuals with electrical devices, such as cardiac pacemakers, and patients who worked more than four hours a day outdoors were also excluded.
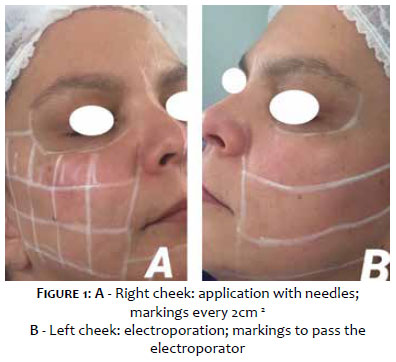
The study was conducted according to the Helsinki declaration’s ethical principles, and all subjects signed an informed consent form and authorization to be photographed. The dilution was 10 BT units per ml, obtained with 10 ml of saline in a 100U bottle of onabotulinumtoxin (Botox® Allergan, Santiago, Chile). The face’s right side was treated with intradermal injections of 0.5 ml (5U) BT at every 2 cm2. The left side was treated with 0.5 ml (5U) of BT delivered uniformly to the predetermined area by facial electroporation, using the Ecleris® electroporator (Buenos Aires, Argentina) (Figure 1).
Facial electroporation is a cosmetic technique based on exposing the skin to a light electric field, which reduces the cell wall’s resistance to make it more porous. The objective is to allow the transfer of topically applied solutions into the skin cells. It is painless and has no adverse events.
Each patient received a micellar cleansing lotion, moisturizing cream, and SPF 50 + sunscreen of the same brand to avoid contact reactions between patients.
We monitored patients before treatment and at weeks two, six, and 12. We assessed the clinical response and adverse events in each control and took digital photographs on the Vectra® system (Canfield, Wentworth Point, Australia) with vascular programming.
The Vectra is a machine made up of eight cameras that take photos simultaneously, building 3D images. With its use, the degree of erythema can be detected and compared, among other functions.
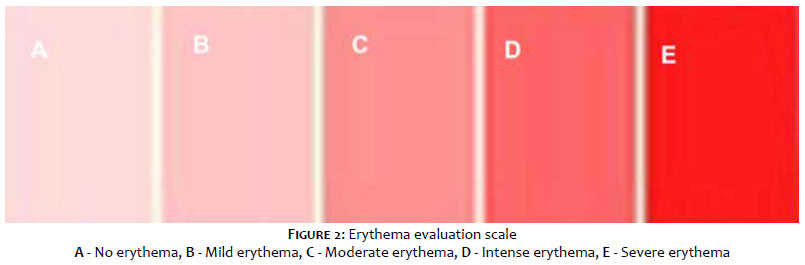
We assessed the erythema using a red colorimetric scale, considering each tone a degree of intensity. Light pink means absence of erythema, intermediate shades correspond to moderate erythema, and intense red correspond to severe erythema (Figure 2).
Clinical responses and adverse events, such as headache, erythema or pain at the injection site, muscle weakness, dysphagia, dry mouth, fatigue, vision changes, or dysphonia, were assessed using a questionnaire. On the final visit, we conducted a quality of life questionnaire to assess satisfaction and reveal which side of the face showed the best results.
We selected 20 patients, but two did not complete the study. Thus, we assessed 18 patients (17 women and one man) with a mean age of 41 years (range: 24 years - 68 years). Of these, 27.78% were skin phototype II (n=5); 66.67% were skin phototype III (n=12); and 5.56% were skin phototype IV (n=1). At the beginning of the study, 94.44% of patients presented erythematotelangiectatic rosacea (n=17), and 5.56% had papulopustular rosacea (n=1).
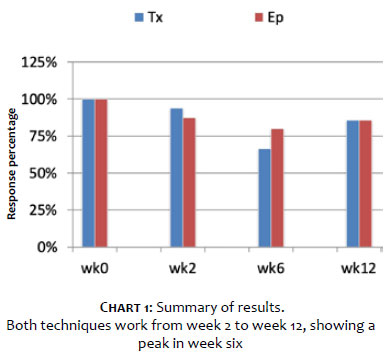
The assessment of the difference in erythema at baseline and two weeks after the electroporation therapy showed the following results: no changes (12.5%); erythema improvement by one degree (56,25%); erythema improvement by two degrees (12.5%); and erythema improvement by three degrees (18.75%). Mean: improvement of 1.375 (standard deviation: 0.96). In short, 87.5% improvement by one to three degrees.
The assessment of the difference in erythema at baseline and two weeks after the needle or mesotherapy therapy showed the following results: no changes (6.25%); erythema improvement by one degree (43.75%); erythema improvement by two degrees (43.75%); and erythema improvement by three degrees (6.25%). Mean: improvement of 1.5 (standard deviation: 0.73). In short, 93.75% improvement by one to three degrees.
The assessment of the difference in erythema at baseline and six weeks after the electroporation therapy showed the following results: erythema worsening by one degree (6.67%); no changes (13.33%); erythema improvement by one degree (26.67%); erythema improvement by two degrees (40%); and erythema improvement by three degrees (13.33%). Mean: improvement of 1.4 (standard deviation: 1.12). In short, 80% improvement by one to three degrees.
The assessment of the difference in erythema at baseline and 12 weeks after the needle therapy showed the following results: erythema worsening by one degree (7.14%); no changes (7.14%); erythema improvement by one degree (35,71%); erythema improvement by two degrees (35.71%); and erythema improvement by three degrees (14.29%). Mean: improvement of 1.43 (standard deviation: 1.09). In short, 85.71% improvement by one to three degrees (Chart 1).
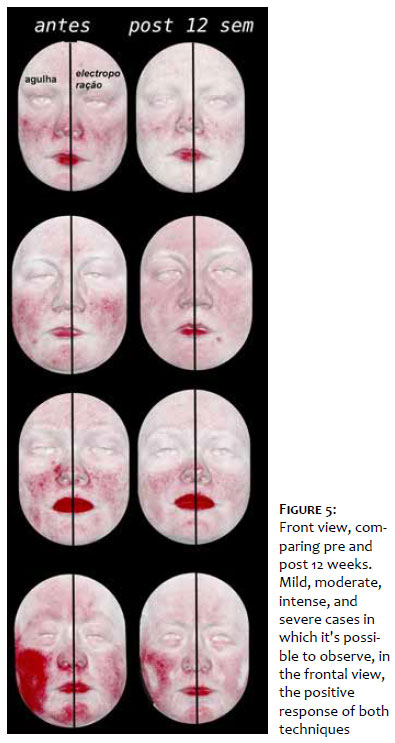
We observed BT’s effectiveness in reducing erythema, which has been evident since the second week, using both the needle and the electroporation technique. This effect persisted until week 12. It is interesting to point out that both therapies were effective, showing a peak at week six (Figures 3, 4, and 5).
Patients described the following adverse events: three cases of ecchymosis, three cases of temporary erythema after application, one case of pain, and one case of tingling at the application site.
BT is a potent neurotoxin. It inhibits the release of acetylcholine (Ach) in the presynaptic vesicle 11. Also, it modulates several other neuropeptides, such as substance P (SP), calcitonin gene-related peptide (CGRP), and vasoactive intestinal peptide (VIP).12 Note that Ach and VIP are the primary mediators of vasodilation and flushing; its inhibition could be the mechanism of action for BT in rosacea.12
Recently, mast cells (Mcs) have emerged in importance in rosacea’s pathogenesis,13 since they are cathelicidin LL-37 activators, which induces skin inflammation, chemotaxis, degranulation, and release of pro-inflammatory cytokines. It is a fact that Mcs-deficient mice do not develop characteristics similar to rosacea after LL-37 injection. On the other hand, the Mcs’ stabilization with sodium cromoglycate reduced the skin’s inflammation in humans and mice. It emphasizes its importance in the cathelicidin inflammation and potential target in rosacea treatment.
It has also been shown that human’s and mouse’s Mcs express proteins SNARE (soluble N-ethylmaleimide sensitive fusion protein receptor), Snap-25, and VAMP (vesicle-associated membrane protein). SNAREs are the main components of coupling and fusion of vesicles with the presynaptic membrane. The blockade BTs A and B vesicles contain neuropeptides through SNAP and VAMP cleavage, respectively. Choi et al. demonstrated direct inhibition of Mcs degranulation in a rosacea model in mice, showing that onabotulinum A and B toxins increased SNAP-25 cleavage and decreased VAMP2 staining in Mcs. In mice, the injection of toxin Onabotulinum A significantly reduces cutaneous erythema induced by LL-37, Mcs degranulation, and mRNA expression of rosacea biomarkers (TRPV, MMP9, KLK5, and others).14
These findings show multiple BT targets and may offer therapeutic advantages over the treatments currently available. Our pilot study shows that, since the second week, there was an improvement in erythema in more than 80% of cases. The exciting fact is that electroporation and needle application had a very similar effect, maintained by more than 85% by week 12. We highlight the advantage of electroporation to avoid trauma.
Assessing the quality of life questionnaire, more than 90% of patients had a positive impact on quality of life. As for adverse events, we did not observe facial dynamics changes; only minimal adverse events to the application are described.
BT is effective in reducing the erythema of patients with rosacea. It can be applied with a needle or electroporation, and its effect remains until week 12. Therefore, it is essential to consider it as a therapeutic tool in erythema and flushing of rosacea. It is a treatment of simple application and low adverse events.
Natacha Quezada Gaón | 0000-0003-2322-3402
Approval of the final version of the manuscript; study design and planning; preparation and writing of the manuscript; data collection, analysis, and interpretation; active participation in research orientation; intellectual participation in propaedeutic and/or therapeutic conduct of studied cases; critical literature review; critical revision of the manuscript.
Maria Isabel Herane Herane | 0000-0003-3362-1623
Statistical analysis; approval of the final version of the manuscript; study design and planning; preparation and writing of the manuscript; data collection, analysis, and interpretation; active participation in research orientation; intellectual participation in propaedeutic and/or therapeutic conduct of studied cases; critical literature review; critical revision of the manuscript.
Mathias Yagnam Diaz | 0000-0003-3562-537X
Statistical analysis; study design and planning; data collection, analysis, and interpretation; active participation in research orientation; intellectual participation in propaedeutic and/or therapeutic conduct of studied cases.
Marlene Waissbluth Morales | 0000-0002-8719-9117
Statistical analysis; study design and planning; preparation and writing of the manuscript; data collection, analysis, and interpretation; active participation in research orientation.
1. Wilkin J, Dahl M, Detmar M, Drake L, et al. Standard classification of rosacea: report of the National Rosacea Expert Committee on the Classification and Staging of Rosacea. J Am Acad Dermatol. 2002;46(4):584-7.
2. Tan J ,Almeida LMC, Bewley A, Cribier B, et al. Updating the diagnosis,classification and assessment of rosácea: recommendations from tje global Rosacea Consensus (ROSCO) panel. Br J Dermatol. 2017;176(2):431-8.
3. Aimee M, Two AM, Wu W, Gallo RL, Hata TR. Rosacea.Part I. Introduction, categorization, histology, pathogenesis and risk factors. J Am Acad Dermatol. 2015;72(5):749-58.
4. Steinhoff M, Schmelz M, Schauber J. Facial erythema of rosacea-aethiology, different pathophysiologies and treatment options. Acta Derm Venereol. 2016;96(5):579-86.
5. Steinhoff M, Schauber J, Leyden JJ. New insights into rosacea pathophysiology: a review of recent findings . J Am Acad Dermatol. 2013;69(6 Suppl ):S15-26.
6. Anzengruber F, Czermielewski J, Conrad C, Feldmeter L, et al. Swiss S1 guideline for the treatment of rosacea. J Euro Acad Dermatol Venereol. 2017;31(11):1775-91.
7. Logger JGM, Olydam JI, DriessenJB. Use of beta-blockers for rosacea-associated facial erythema and flushing: a systematic review and update on proposed mode of action. J Am Acad Dermatol. 2020;83(4):1088-97.
8. Feily A, Fallahi H, Zandian D, Kalantar H. A succinct review of botulinum toxin in dermatology; update of cosmetic use and noncosmetic use. J Cosm Dermatol. 2010;10(1):58-67.
9. Dayan SH, Pritzker RN, Arkins JP. A new treatment regimen for rosacea: onabotulinumtoxin A. J Drugs Dermatol. 2012;11(12):e76-9.
10. Antonio CA, Tridico LA, Antonio JR. Treatment of rosácea with botulinum toxin. Surg Cosmet Dermatol 2018;(3 Suppl 1):36-9.
11. Huang W, Foster JA, Rogachefsky AS. Pharmacology of botulinum to9xin. J Am Acad Dermatol. 2000;43 (2 Pt 1):249-59.
12. Aoki KR. Review of a proposed mechanism for the antinociceptive action of botulinum toxin type A. Neurotoxicology 2005;26(5):785-93.
13. Wilkins BW, Chung LH, Tublitz NJ, Womg BJ, et al. Mechanisms of vasoactive intestinal peptide mediated vasodilatation im human skin. J.Appl Physiol. 2004;97(4):1291-8.
 All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773
All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773



 Read in Portuguese
Read in Portuguese
 Portuguese PDF
Portuguese PDF
 Print
Print
 Send this article by email
Send this article by email
 How to cite this article
How to cite this article
 Submit a comment
Submit a comment
 Mendeley
Mendeley
 Pocket
Pocket
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}