


Érico Pampado Di Santis1,2; Samira Yarak1; Marcos Roberto Martins3; Sergio Henrique Hirata1
Received on: 30/08/2020
Approved on: 10/11/2020
Financial support: None
Conflict of interest: None
Study conducted at the Evidence-Based Health Post-Graduate Program of the Universidade Federal de São Paulo
Acknowledgment: This research started at the suggestion and encouragement of the late professor Sebastião de Almeida Prado Sampaio, who used to archive news related to liposuction deaths. This professor has always believed in small volume liposuction safety under local anesthesia using microcannulas, as performed among dermatologists
INTRODUCTION: Liposuction is one of the most performed cosmetic surgeries in the world. Its mortality varies from 2,6 (6) to 19 (7) deaths/100 thousand. Data were obtained through questionnaires from medical societies (4-10) and retrospective data from forensic medicine institutes. However, both methods present flaws: the first due to professional bias and information duplicity, and the second due to the lack of data on the cause of death.
OBJECTIVES: To identify the number and causes of liposuction deaths through documentary records of news published in the press and study of death certificates.
METHODS: This is a documentary, descriptive-quantitative study. Knowing the deceased patients’ names and the cities where the death occurred, we obtained death certificates from the civil registry offices.
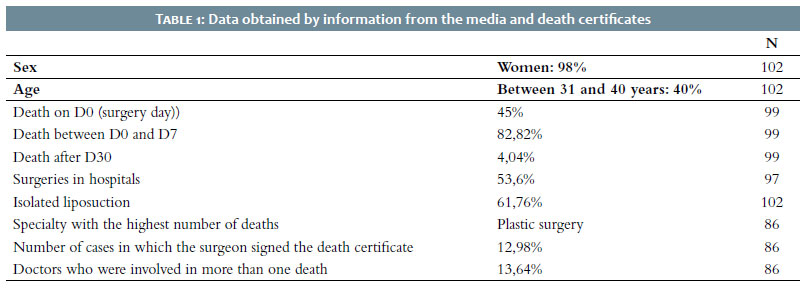
RESULTS: We surveyed 102 deaths and 86 death certificates. Pulmonary thromboembolism was the most cited cause of death in 17.44%, 45% on the same day of surgery. 53.6% of surgeries were performed in hospitals, and 61.76% of them, alone. Most physicians responsible for the surgeries were plastic surgeons (74%). Still, none were registered as a specialist in Dermatology at the Federal Medical Council. In 12.98% cases, doctors who participated in the surgery filled out the death certificate.
LIMITATIONS: The ethical impossibility of accessing medical records and the inadequate filling of death certificates.
CONCLUSION: The compulsory notification must be established by law to create a databa
Keywords: Liposuction; dead.
Liposuction is the medical-surgical procedure for treating the accumulation of superficial adipose tissue that damages the body silhouette. Aspiration is done through cannulas connected to the vacuum pump (sucker) or syringe, which generate negative pressure.1, 2
From 2011 to 2020, liposuction ranked among the first positions of the most performed cosmetic surgeries globally, with more than one million surgeries performed each year.
The number and causes of death, of young and healthy patients in general, are not well established.2,8,10
We believe that surveying the number of deaths through the news published in the press is a more effective method than sending questionnaires to members of medical societies or retrospectively studying legal medical records. The latter have deficiencies, such as the bias of responses and the lack of data on death certificates for reliable analysis. The data obtained may contribute indirectly to the establishment of prophylactic measures. Thus, this work aims to verify the incidence of causes of death from liposuction and to identify other variables that may be related to them.
This is a documentary, descriptive-quantitative study, approved by the Ethics and Research Committee of UNIFESP-EPM (CEP 542.458) from 1987, the date of the first death from a liposuction surgery in Brazil, until September 2015.
We used news from the media to raise the number of deaths related to liposuction in Brazil in this period, from the first news of death after liposuction to when 100 reported cases were exceeded. Our databases were news written in the largest printed newspapers and analysis of the leading news portals on the World Wide Web.
The press generally reports the victim’s name and surname, sex, age, marital status, local of the surgery institute, and surgery and death dates. With this information, together with the civil registry offices, we obtained death certificates. These documents allowed us to confirm the variables acquired by the press and to recognize other data such as color, causa mortis (reflected in the death certificate filled out by a medical professional), and the name of the professional involved. Data were also collected regarding sex, age, color, marital status, surgery and death dates, local of the surgery institute, and the cause declared by the sources (death certificate and press). Subsequent consultations on the websites of medical councils and societies allowed us to know the specialty of the doctor who performed the surgery.
We surveyed 102 cases of death related to liposuction between January 17, 1987, and September 15, 2015. Also, we obtained 86 death certificates (84.31%) from civil registry offices.
Women represented 98.04% of these 102 patients. The age varied between 18 and 62 years. The age group between 31 and 40 years represented 40% of the cases (Table 1).
Death on day zero (day of surgery) occurred in 45% of cases. When considering death between the day of surgery and the end of the first week (D7), this value increased to 82.82%; from the second week to the 28th day, 13.13%, and after the first month, 4.04% (N=99). It was possible to identify 97 institutional sites that performed the surgeries. Hospitals performed 53.6% of surgeries, and clinics outside hospitals conducted 46.4%. The association of liposuction with other procedures occurred in 38.24% of cases, while 61.76% of cases reported liposuction performed in isolation.
Regarding the specialties of the doctors involved, we were able to detect them in 86 cases. Of these, 66 doctors had a registered specialty, 61 in plastic surgery, two in general surgery, two in orthopedics, one in diagnostic imaging; 20 professionals had not registered any medical specialty; and 13.64% of doctors were involved in more than one surgery that resulted in the patient’s death.
Of the causes of death, thromboembolism ranked first with 17.44%, followed by perforation (13.95%), infection (9.3%), hemorrhage (5.81%), fat embolism (4.65%), and acute lung edema and anesthetic complications, with 2.32% each (N=86). In 44.18% of the cases, it was not possible to determine the cause of death.
Death resulting from liposuction is a misfortune in public health.3 The lack of knowledge of its causes prevents us from having reliable data to elaborate protocols that can prevent it.
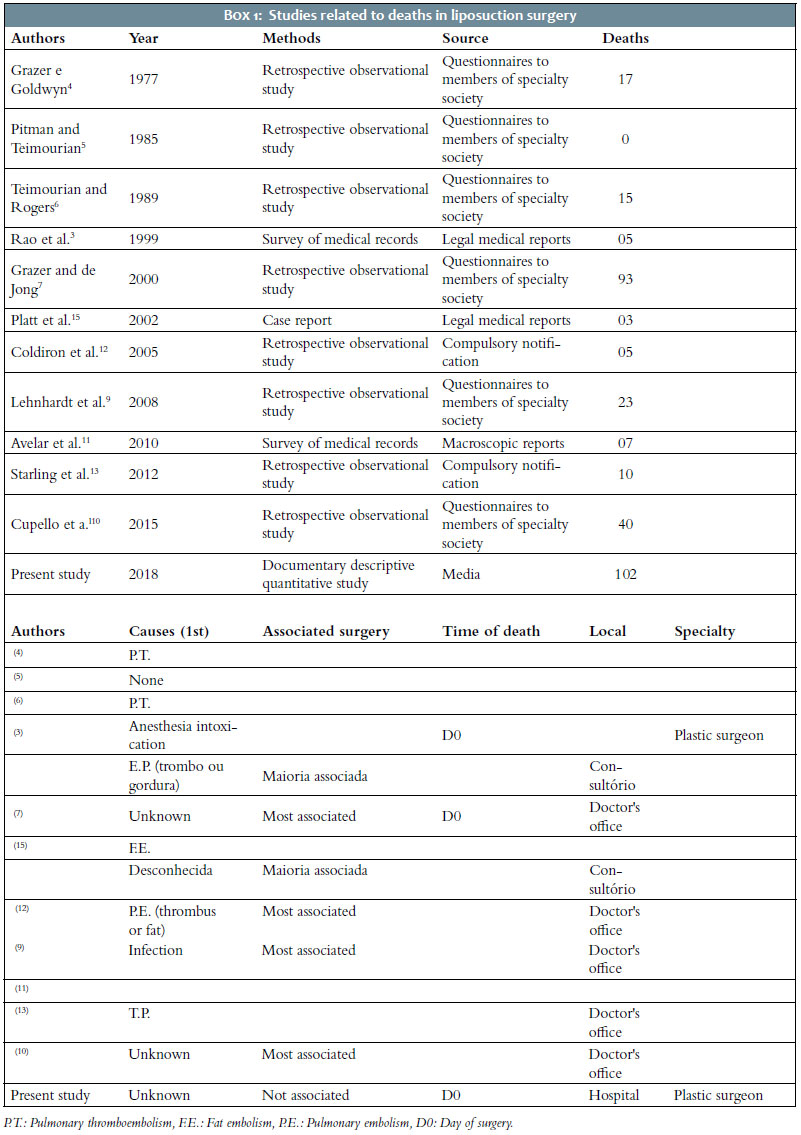
The sample found in the studies previously conducted is related to the difficulty in obtaining data regarding deaths. In the literature, we found two methods to obtain this information: questionnaires sent to members of medical societies, usually plastic surgery societies,4-10 and the retrospective study of data obtained from a legal medical institute.3, 11
The method that used sending questionnaires was criticized7 for the possibility of biased responses. It is reasonable to assume that the doctor did not answer or omit data, as he can use the legal benefit of not producing evidence against him. The low response rate observed in most of these studies confirmed this hypothesis.4-6, 9,10 This type of result is expected since the doctor involved has the right not to present evidence that could harm him. Retrospective studies3,11 of data obtained in legal medical institutes are also deficient, as the surgical procedure involved is often not mentioned, hindering the ability to identify deaths related to liposuction.
Because they are impactful news, deaths due to liposuction are widely reported in the press and generate enormous concern in gyms and medical councils. Based on this fact, the present study was initiated, which searched for news published in the printed and digital media and subsequently analyzed public documents.
With this methodology, we found 102 deaths related to liposuction, the largest sample among the scientific literature studied4-10 (Box 1). The analysis of death certificates prevents the same case from being included two or more times, as can occur in studies using questionnaires that can send it to two doctors who participated in the same surgery.
As this surgery is performed more frequently on women, the majority of deaths found were among women (98.04%) and among young people (97.05%), similar to data from the International Society of Aesthetic Plastic Surgery (84.9% of the patients submitted to liposuction in 2017 were women). These patients were healthy and underwent elective surgery expecting to remain in good health.
Regarding the reason for deaths, there are differences when consulting the literature. In the present study, it was impossible to establish the cause of death in 44.18% of the cases (undetermined). Thromboembolisms occurred in 17.44% and infection in 9.3% of cases.
The unknown cause also ranked first place in the Grazer and Jong’s study,7 with 28.5% of cases, and ranked fifth in the Lehnhardt et al. study,9 with 4.35%.
Regarding the known causes, when compared with the Grazer and Jong’s study,7 (method used: questionnaires sent to doctors), the order of the first two causes coincides: thromboembolic phenomena are the first, with 23.1%, and perforation is the second, with 14.6%. The leading causes of death in Lehnhardt et al. study9 are infection as the first cause, with 65%, perforation as second, with 13%, followed by thromboembolic phenomena in the third position, with 8%.
But we must take care when interpreting the data. Cupello et al.10 stated that their data should be interpreted with caution, as the study included many missing responses. Unknown death cause ranked last place in Lehnhardt et al. study.9 However, even with the support of several medical societies and sending three thousand questionnaires, only 23 cases of death were recorded.
Hughes8 reported an alarming increase in the mortality rate when liposuction was performed concurrently with abdominoplasty compared to when it was performed alone, with one death in 3,281 surgeries versus one death in 47,415 surgeries, respectively. Combining these surgeries or large volume liposuction can play an essential role in the causes of death. We did not find the same result. The number of deaths found in liposuction performed in isolation, declared in media interviews by members of the surgical team, was 61.76%.
Our study showed that the critical period in liposuction surgeries is the first week after surgery, especially the first day (45% of patients died on the day of surgery and 82,82% on the first week). We believe that this data demonstrates the importance of care in the 24-hour postoperative period and the first week, with more frequent reevaluations.
For the 102 cases investigated, there was no evidence of deaths occurring with the use of tumescent local anesthesia, as described by Klein.16 There was also no mention in the death certificates of lidocaine poisoning as a cause of death or process that led to it. Klein’s technique is safer because the patient under local anesthesia still has a pain reflex and feels pain if the cannula touches the muscular fascia. It avoids the possibility of muscle perforation, which can occur when the cannula is not placed in the appropriate place. Also, the rate of blood depletion using this technique is significantly lower.
Compulsory notification of cases would favor the creation of a database. This notification must document the detailed study of the surgery (technique performed, anesthesia used, amount aspirated, etc.), the preoperative health status, and the postoperative complications that led the patient to death. Also, it must be accessible so that committees can establish guidelines for death prevention in cosmetic surgery.
It is crucial that public health authorities develop strategies to identify deaths related to aesthetic procedures and that these cases undergo necropsy (including toxicological tests).14 The data obtained will assist in the establishment of preventive measures. In the United States, Florida’s and Alabama’s governments determined the obligation to report complications occurring in extra-hospital surgical procedures.12,13 Our study could only find data such as the type of anesthesia used in these surgeries by consulting patients’ medical records and confidential documents.
Future studies with the records of these victims may clarify the gaps left in the present study. A standard access to medical records by medical researchers, with all ethical and legal rigor, will undoubtedly benefit public health.
The search for ways to best fill out death certificates can mean an improvement in the system, functioning, and knowledge of the real causes of deaths. It would allow us to be more efficient in preventing deaths.
We believe that the compulsory notification of complications by cosmetic procedures can act prophylactically against damage to individuals’ health, families’ suffering, and expenses in the health system.
The search for deaths related to liposuction reported in the media is a tool that adds to the other methods available in the literature. Among the 102 cases studied, thromboembolism was the most cited cause of death, and most deaths occurred in the first seven postoperative days. There was no relationship between fatalities and the performance of more than one procedure in the same surgery or the place where the surgeries were performed.
Érico Pampado Di Santis | 0000-0001-5782-9205
Approval of the final version of the manuscript; study design and planning; preparation and writing of the manuscript; data collection, analysis, and interpretation; critical revision of the manuscript.
Samira Yarak | 0000-0002-5657-6645
Approval of the final version of the manuscript; study design and planning; preparation and writing of the manuscript; data collection, analysis, and interpretation.
Marcos Roberto Martins | 0000-0001-7985-0910
Approval of the final version of the manuscript; preparation and writing of the manuscript; data collection, analysis, and interpretation.
Sergio Henrique Hirata | 000-0003-4026-9664
Approval of the final version of the manuscript; preparation and writing of the manuscript; data collection, analysis, and interpretation.
1. Fischer A, Fischer G. First surgical treatment for molding body's cellulite with three 5 mm incisions. Bull Int Acad Cosmet Surg. 1976;3:35.
2. EH C. Liposuction: some memories and thougths. Aesth surg j. 1997;17(2):107-11.
3. Rao RB, Ely SF, Hoffman RS. Deaths related to liposuction. N Engl J Med. 1999;340(19):1471-5.
4. Grazer FM, Goldwyn RM. Abdominoplasty assessed by survey, with emphasis on complications. Plast Reconstr Surg. 1977;59(4):513-7.
5. Pitman GH, Teimourian B. Suction lipectomy: complications and results by survey. Plast Reconstr Surg. 1985;76(1):65-72.
6. Teimourian B, Rogers WB. A national survey of complications associated with suction lipectomy: a comparative study. Plast Reconstr Surg. 1989;84(4):628-31.
7. Grazer FM, Jong RH. Fatal outcomes from liposuction: census survey of cosmetic surgeons. Plast Reconstr Surg. 2000;105(1):436-46; discussion 47-8.
8. III. Hughes C. Reduction of lipoplasty risks and mortality: an ASAPS survey. Aesth Surg J. 2001;2:120-7.
9. Lehnhardt M, Homann HH, Daigeler A, Hauser J, Palka P, Steinau HU. Major and lethal complications of liposuction: a review of 72 cases in Germany between 1998 and 2002. Plast Reconstr Surg. 2008;121(6):396e-403e.
10. Cupello AMB, Dornelas M, Aboudib Junior J, Castro CC, Ribeiro LC. Intercorrências e óbitos em lipoaspiração: pesquisa realizada pela comissão de intercorrências da SBCP. Rev Bras Cir Plást. 2015;30(1):58-63.
11. Avelar LET, Lapertosa L. Óbitos pós-lipoaspiração. Rev Bras Cir Plást. 2010;25(3):60.
12. Coldiron B, Fisher AH, Adelman E, Yelverton CB, Balkrishnan R, Feldman MA, et al. Adverse event reporting: lessons learned from 4 years of Florida office data. Dermatol Surg. 2005;31(9 Pt 1):1079-92; discussion 93.
13. Starling J, Thosani MK, Coldiron BM. Determining the safety of office-based surgery: what 10 years of Florida data and 6 years of Alabama data reveal. Dermatol Surg. 2012;38(2):171-7.
14. Jong RH, Grazer FM. "Tumescent" liposuction alert: deaths from lidocaine cardiotoxicity. Am J Forensic Med Pathol. 1999;20(1):101.
15. Platt MS, Kohler LJ, Ruiz R, Cohle SD, Ravichandran P. Deaths associated with liposuction: case reports and review of the literature. J Forensic Sci. 2002;47(1):205-7.
16. Klein JA. Tumescent technique for regional anesthesia permits lidocaine doses of 35 mg/kg for Liposuction. J Dermatol Surg Oncol. 1990;16:248-63.
 All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773
All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773



 Read in Portuguese
Read in Portuguese
 Portuguese PDF
Portuguese PDF
 Print
Print
 Send this article by email
Send this article by email
 How to cite this article
How to cite this article
 Submit a comment
Submit a comment
 Mendeley
Mendeley
 Pocket
Pocket
{kind=link}
{kind=link}