


Natalia Naomi Suzuki; Juliana Schinzari Palo; Renata Ferreira Magalhães; Thais Helena Buffo; Hamilton Ometto Stolf
Received on: 27/07/2020
Approved on: 16/11/2020
Financial support: None
Conflict of interest: None
Acknowledgement: We thank Dr. Hamilton Ometto Stolf for his mastery of surgical technique and his brilliant ability to teach his students, and to Dr. Thais Helena Buffo for the ease and love with which she teaches dermatological surgery
Study conducted at the Universidade Estadual de Campinas, Campinas (SP), Brazil
Rhinophyma is a disfiguring and progressive disease of the nose with high prevalence. Despite being considered a benign condition, many patients have sought curative treatments due to aesthetic deformity and social stigmatization. There are several surgical techniques described in the treatment of this disease. This report aims to present a case that required an unusual therapeutic approach for the treatment of rhinophyma, given the patient's multiple comorbidities. The procedure was performed with no complications in the intra and postoperative period. The patient maintains an outpatient follow-up with a good long-term aesthetic result.
Keywords: Dermatologic Surgical Procedures; Rhinophyma; Rosacea
Rhinophyma is a disease of the nose characterized by hypertrophy of the sebaceous glands and proliferation of blood vessels and connective tissue.1 Phymatous changes classically affect the lower two-thirds of the nose, and may also occur in the chin, forehead, or ear.1 It is considered the most severe expression of the final stage of rosacea.1
Clinically, rhinophyma manifests with an enlarged nose with irregular texture, enlarged pores, and telangiectasia.2 These findings correspond, in histopathology, to sebaceous hyperplasia, infundibular dilation, and surrounding lymphohistiocytic infiltrate.2 In more advanced stages, the nasal contours are distorted, and there is a loss of demarcation between its subunits, which can compromise the respiratory airways.2,3
Despite being considered a benign disease, many patients have sought curative treatments. Surgical methods are preferred over clinical treatment since the condition has a significant cosmetic deformity and social stigmatization.2 The literature describes different surgical techniques for the treatment of rhinophyma, including the use of cold scalpels, electric scalpels and handles, and the CO2 laser.4
This report aims to present the cross-shaped excision technique for treating rhinophyma in a patient with multiple comorbidities. The surgery was performed without complications in the intra and postoperative periods, and long-term outpatient follow-up showed good aesthetic results.
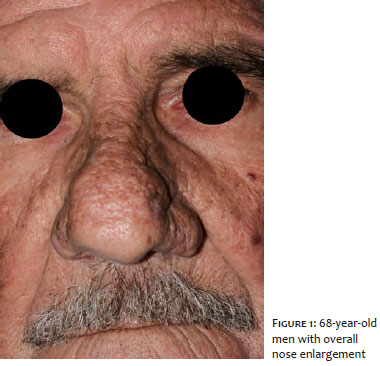
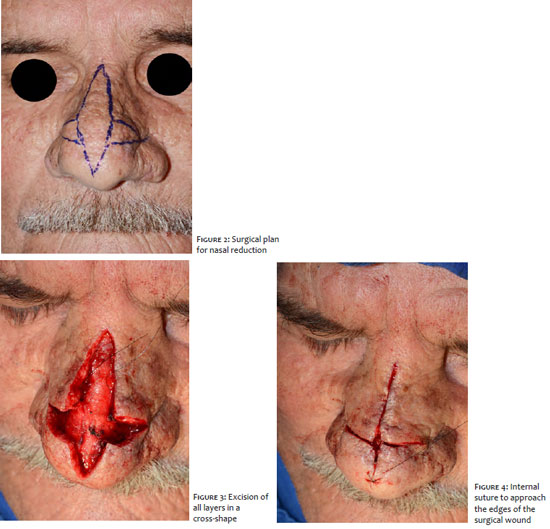
A 68-year-old man presented progressive nasal enlargement with an irregular surface, enlarged pores, and telangiectasia (Figure 1). He reported aesthetic discomfort and social damage. We then opted for surgical treatment. As he presented several comorbidities, such as heart transplantation using immunosuppressants and antiplatelet agents, abdominal aortic aneurysm, and arterial hypertension, it was necessary to choose a quick surgical approach, with little bleeding and with a lower risk of complications. A vertical incision excised the excised skin at the nasal tip and dorsum and a horizontal cut in the alar sulcus, in a cross-shape, to reduce the hypertrophic tissue and the nose (Figures 2 to 4). It was followed by primary closure of the lesion, initially with internal suture approaching the surgical wound’s edges and, after, external suture. There were no immediate complications or recurrence of the condition during the 36-month follow-up (Figure 5).
Friedrich Dieffenbach presented the first descriptions of surgical treatment for rhinophyma in 1845. He excised the phymatous skin by making a vertical incision in the nasal tip and a horizontal incision in both nasal alar grooves, subsequently proceeding to the lesion’s primary closure.4,5 This cross-shaped resection technique to reduce nasal volume is a quick procedure, with little bleeding and low risk of complications, with the advantage of removing part of the hypertrophic tissue, providing a good aesthetic result for the patient and, most importantly, providing a fast recovery.5
The use of scalpels, cold or electric, and a tangential excision knife (for shaving) for superficial decortication of the rhinophyma and healing by secondary intention corresponds to a fast, low-cost, and relatively easy technique. However, it presents the main limitations of the excessive bleeding and, consequently, worse visualization of the surgical field and difficulties in modeling the affected region, besides care with dressings and successive returns.6 Since the reported patient had a previous history of platelet anti-aggregation and immunosuppression therapy by heart transplantation, we couldn’t suspend the medication; thus this technique was not the first treatment choice.
The CO2 laser, on the other hand, is a good therapeutic option, when available, with adequate hemostasis and precision. However, it requires specially trained staff, prolonged time to perform the procedure, and has a high cost.6,7
The risk of recurrence is variable and has been described in some series of cases, with good short-term cosmetic results but varying percentages according to the treatment performed and the follow-up time.4 A series of 70 patients, published in 2016, pointed to a recurrence rate of 38% with the cold scalpel technique and secondary wound closure after 54-month follow-up.4 The reappearance of the phymatous changes occur by maintaining the pilosebaceous units, which provide the basis for reepithelization.4 In the case described, part of the hypertrophic tissue was excised in all its thickness, which could be a contributing factor for reducing long-term recurrences. When performed in two stages, a few months apart, the entire cosmetic unit’s mechanical abrasion helps in camouflaging the surgical scar.5 Because it is not frequently used, there are no studies showing the rate of rhinophyma recurrence in patients undergoing the technique used in this report.
Cross-shaped excision and primary closure are a great option with very satisfactory results in patients with multiple comorbidities. A simple, safe, efficient, and not usually reported surgical technique for the treatment of rhinophyma.
Natalia Naomi Suzuki | 0000-0003-0034-8480 Approval of the final version of the manuscript; study design and planning; preparation and writing of the manuscript; critical literature review; critical revision of the manuscript.
Juliana Schinzari Palo | 0000-0002-7914-5370 Approval of the final version of the manuscript; critical revision of the manuscript.
Renata Ferreira Magalhães | 0000-0001-9170-932X Approval of the final version of the manuscript; critical revision of the manuscript.
Thais Helena Buffo | 0000-0002-6833-7596 Approval of the final version of the manuscript; study design and planning; active participation in research orientation; critical revision of the manuscript.
Hamilton Ometto Stolf | 0000-0003-4867-0276 Approval of the final version of the manuscript; study design and planning; active participation in research orientation; intellectual participation in propaedeutic and/or therapeutic conduct of studied cases; critical revision of the manuscript.
1. Krausz AE, Goldberg DJ, Ciocon DH, Tinklepaugh AJ. Procedural management of rhinophyma: a comprehensive review. J Cosmet Dermatol. 2018;17(6):960-7.
2. Tüzün Y, Wolf R, Kutlubay Z, Karakus O, Engin B. Rosacea and rhinophyma. Clin Dermatol. 2014;32(1):35-46.
3. Sadick H, Goepel B, Bersch C, Goessler U, Hoermann K, Riedel F. Rhinophyma: diagnosis and treatment options for a disfiguring tumor of the nose. Ann Plast Surg. 2008;61(1):114-20.
4. Schweinzer K, Kofler L, Spott C, Krug M, Schulz C, Schnabl SM, et al. Eur J Dermatol. 2017;27(3):281-5.
5. Elliott RA, Ruf LE, Hoehn JG. Rhinophyma and its treatment. Clin Plast Surg. 1980;7(3):277-88.
6. Karacor-Altuntas Z, Dadaci M, Ince B, Altuntas M. A new surgical technique of rhinophyma (Gull-Wing Technique). J Craniofac Surg. 2015;26(1):e28-e30.
7. Fink C, Lackey J, Grande DJ. Rhinophyma: a treatment review. Dermatol Surg. 2018;44(2):275-82.
 All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773
All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773



 Read in Portuguese
Read in Portuguese
 Portuguese PDF
Portuguese PDF
 Print
Print
 Send this article by email
Send this article by email
 How to cite this article
How to cite this article
 Submit a comment
Submit a comment
 Mendeley
Mendeley
 Pocket
Pocket
{kind=link}
{kind=link}
{kind=link}