


Gerson Dellatorre1; Marcos Noronha Frey2; Roberto Gomes Tarlé1
Received on: 05/04/2020
Approved on: 25/08/2020
Financial support: None
Conflict of interest: None
Study conducted at the Santa Casa de Curitiba Hospital, Curitiba (PR), Brazil
Skin cancer frequently occurs on the pinna. The three-dimensional conformation and the limited availability of redundant regional skin make the reconstruction of this anatomical area challenging. We report the reconstruction of anti-tragus using an earlobe transposition flap.
Keywords: Carcinoma, Squamous cell; Ear auricle; Mohs surgery; Skin neoplasms; Surgical flaps
The pinna is a place with a high incidence of skin cancer. The literature estimates that about 16% of skin tumors occur at this location.1 The pinna is formed by several subunits endowed with concavities and convexities that make its shape peculiar, requiring a detailed surgical reconstruction after the excision of tumors. We describe the reconstruction of a full-thickness defect of the antitragus using an earlobe transposition flap after a Mohs micrographic surgery (MMS).
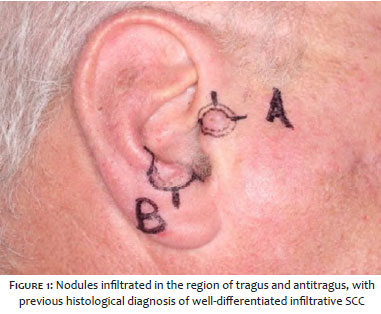
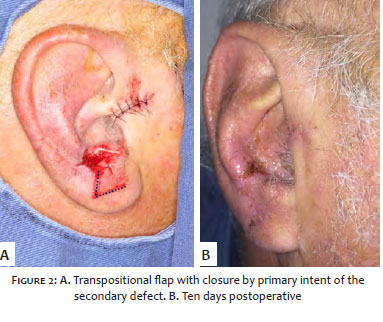
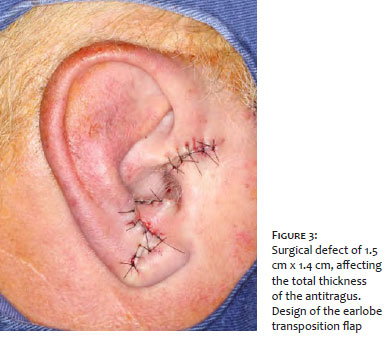
A 72-year-old patient presented two well-differentiated squamous cell carcinomas (SCCs), located (Figure 1) in the region of the tragus and the antitragus. Both tumors were treated using the MMS technique, with free margins obtained in the first stage. After the closure by primary intent of the tragus region, a surgical defect of 1.5 cm x 1.4 cm, compromising the sub-unit of antitragus, was still present. An earlobe transposition flap was planned (Figure 2), with its redundancy in the pivotal region, purposely left to recreate the contour and projection present in the antitragus’ natural anatomy (Figure 3).
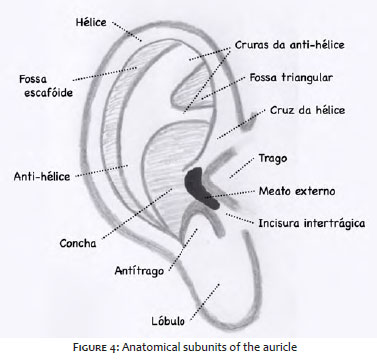
About 12 subunits or anatomical points of interest form the pinna (Figure 4).2 Regarding the antitragus, the literature on its reconstruction is scarce. A literature review found three articles describing complex techniques for its reconstruction, with good cosmetic results. A case report written by Chadha, Grob, and Soldin3 described an “open book” flap in the reconstruction of a defect involving antitragus, conchal bowl, and antihelix in a case of SCC. The lesion was removed, and the surgical defect repaired using a tunneled transposition flap of the preauricular region in a single time. Finally, Gonzalez-Sixto et al.5 described a series of four reconstructed ear defects with a chondrocutaneous advancement flap by V-Y advancement. One of them used the flap to reconstruct the antitragus.
Primary and secondary wound closures are also simple closure options for this subunit, although earlobe elevation may occur as a consequence. The limited availability of redundant skin and the frequent extrapolation of anatomical subunits by tumors in this region make the pinna reconstruction challenging.6,7 The earlobe is one of the few ear sites with sagging skin, thus being useful for use as a donor site in flaps.
Gerson Dellatorre | 0000-0002-9657-0002 Approval of the final version of the manuscript; study design and planning; preparation and writing of the manuscript; data collection, analysis, and interpretation; active participation in research orientation; intellectual participation in propaedeutic and/or therapeutic conduct of studied cases; critical revision of the manuscript.
Marcos Noronha Frey | 0000-0003-3914-2586 Approval of the final version of the manuscript; study design and planning; preparation and writing of the manuscript; data collection, analysis, and interpretation; intellectual participation in propaedeutic and/or therapeutic conduct of studied cases; critical literature review.
Roberto Gomes Tarlé | 0000-0003-2831-6579 Approval of the final version of the manuscript; study design and planning; critical revision of the manuscript.
1. Norris II, Cook J. The cheek interpolation flap for reconstruction of auricular Mohs defects. Dermatol Surg. 2020;46(8):1039-44.
2. Alvord LS, Farmer BL. Anatomy and orientation of the human external ear. J Am Acad Audiol. 1997;8(6):383-90.
3. Chadha A, Grob M, Soldin M. Use of the earlobe in auricular reconstruction post tumour extirpation. J Plast Reconstr Aesthet Surg. 2009;62(4):539-41.
4. Braga AR, Pereira LC, Grave M, Resende JH, Lima DA, Souza AP, et al. Tunnelised inferiorly based preauricular flap repair of antitragus and concha after basal cell carcinoma excision: case report. J Plast Reconstr Aesthet Surg. 2011;64(3):e73-5.
5. Gonzalez-Sixto B, Perez-Bustillo A, Otero-Rivas MM, Rodriguez-Prieto MA. Subcutaneous pedicled V-Y advancement flap for surgical reconstruction of the auricle of the ear. Actas Dermosifiliogr. 2014;105(4):e23-6.
6. Brodland DG. Advanced reconstruction of the ear: a framework for successful wound closure. Dermatol Surg. 2014;40(Suppl 9):S71-85.
7. Reddy LV, Zide MF. Reconstruction of skin cancer defects of the auricle. J Oral Maxillofac Surg. 2004;62(12):1457-71.
 All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773
All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773



 Read in Portuguese
Read in Portuguese
 Portuguese PDF
Portuguese PDF
 Print
Print
 Send this article by email
Send this article by email
 How to cite this article
How to cite this article
 Submit a comment
Submit a comment
 Mendeley
Mendeley
 Pocket
Pocket
{kind=link}
{kind=link}
{kind=link}
{kind=link}