


Amanda Bertazzoli Diogo; José Roberto Pegas; Mariana de Freitas Valente; Cristina Santos Ribeiro Bechara
Received on: 20/12/2019
Approved on: 25/08/2020
Financial support: None Conflict of interest: None
Acknowledgement: We thank our preceptors, especially Maria do Rosário Vidigal, for the teachings and encouragement
Study conducted at the Padre Bento de Guarulhos Hospital Complex, Garulhos (SP), Brazil
Koenen tumors are nail fibromas included among the main diagnostic criteria of tuberous sclerosis. Elongated and thin papules, firm, with smooth surface and broad base characterize these lesions, which are slightly erythematous and present varying sizes. Koenen tumors commonly affect toenails and result in aesthetic and functional concerns associated with deformities, pain, and bleeding. Several therapeutic options are described for Koenen tumors; however, there is a lack of consensus in the literature regarding standard treatment. We report the case of a patient who underwent surgery with excellent outcomes. Additionally, we discuss the advantages and disadvantages of each therapeutic modality.
Keywords: Dermatologic Surgical Procedures; Fibroma; Nails; Tuberous Sclerosis
Also known as Bourneville-Pringle epiloia or phacomatosis, tuberous sclerosis (TS) is a rare, multisystemic neurocutaneous disorder that can develop with hamartomas of skin, central nervous system, kidneys, and lungs.1
In the context of this autosomal dominant disease, it is known that half of the affected families are linked to chromosome 9q34, with inactivating mutations of the tumor suppressor genes of the hamartin protein (TSC1), and the other half to chromosome 16p13. It causes inactivating mutations of genes tumor suppressors of tuberin protein (TSC2). The hamartin-tuberin complex is an essential tumor growth inhibitor, and its absence triggers the loss of inhibition on cell proliferation and migration.2
Among the most common skin changes are facial angiofibromas, fibrotic plaques (Shagreen patch), periungual fibromas (Koenen’s tumors), hypochromic macules in the shape of leaves (ash leaves), and frontal fibrous plaque.1,2 Many patients have nail fibroma as the only cutaneous manifestation of the disease, so their presence in the dermatological physical examination should raise the disease’s clinical suspicion.3
In addition to Koenen’s tumor (KT), the literature describes other nail disorders in TS, such as subungual hyperkeratosis, reddish and whitish longitudinal leukonychia, hemorrhagic splinters, and longitudinal grooves. It is believed that the presence of reddish and/or whitish longitudinal ridges, in addition to nail fibroma, greatly increases the suspicion of TS.4
Other significant findings include seizures, intellectual disability, subependymal nodules, retinal, and other organ hamartomas.2 Although surgical excision is preferable for nail fibroma,5 other therapies are available. However, few studies compare the efficacy and disadvantages of different therapeutic modalities.
A 38-year-old woman presented progressive nail growths on her fingernails and toenails since the second decade of life. It caused local bleeding after minimal trauma, pain, and deformities, making it impossible to wear closed shoes and manipulate objects. She denied comorbidities and reported a father with TS.
The nail lesions presented as elongated and tapered papules, firm, with a smooth surface, broad base, slightly erythematous, and varied sizes, in all toes and some fingers (Figures 1-3). Regarding location, most had implantation in the proximal fold and a small part in the lateral folds. Some nail plates showed longitudinal lines and canalicular depressions of variable extension, with some thin whitish ridges (Figure 1). In the limbs, there were multiple hypochromic spots in the shape of a leaf (ash leaves), in addition to homochromatic lenticular lesions, confetti-like. On the face, we observed flat, normochromic, isolated, and coalescent papules, especially in the malar and dorsal nasal regions, suggesting angiofibromas. In the abdominal and dorsal area, she had hypochromic stains, measuring up to about 20 cm.
The anatomopathological examination of nail lesions was compatible with digital fibrokeratomas; on the face, with angiofibromas; and the hypochromic spots on the chest, with achromatic nevus. Computed tomography (CT) of the skull showed dysplasias and cortical fibromas, without other changes. Therefore, given skin and nail lesions, complementary exams, and family history, we established the TS diagnosis.
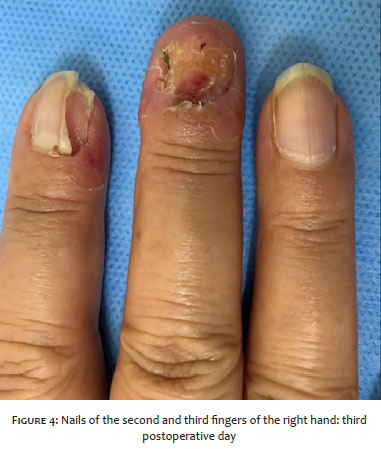
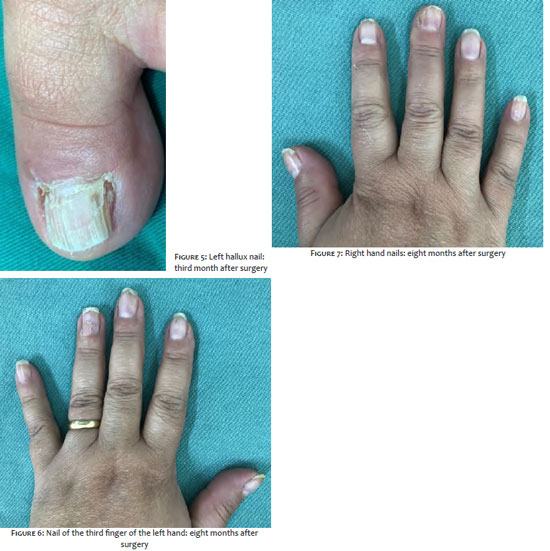
We opted for surgical excision of nail lesions, removing four tumors in each surgical period. The nails of the hands and the left foot were approached. Fibromas located in the posterior fold were excised by folding the nail plate through two parallel incisions at the posterior and lateral folds’ junction. Once folded, the origin of the tumor implantation was visualized, proceeding to their detachment, with the aid of dental spatulas, until its total removal. In the postoperative period (Figure 4), the patient followed the guidelines regarding rest, cleaning, and dressing, progressing satisfactorily, with good aesthetic and functional results (Figures 5-7). The patient is followed up to continue the surgical treatment.
KTs are nail hamartomas mainly in the toes, more common in women, and appearing mostly after the second decade of life. They can progressively increase in size, compressing the nail matrix, and causing changes such as longitudinal nail depressions.1 They are classified as peri or subungual, the first being the most common.6 It is a benign cutaneous manifestation of TS, present in about 50% of patients.7 Trauma and pressure exerted by the shoes are triggering factors, which justifies the feet’s most common location.3
The various treatment options include surgical excision, CO2 laser, shaving followed by phenolization,7 topical rapamycin,8 and even nail amputation.2 There are divergences in the literature about the best therapeutic option.7 Each modality has advantages and disadvantages, and, regarding the recurrence rate after the proposed treatments, there are no consistent data in the literature. However, it is believed that techniques that preserve the matrix may have significant recurrences.7
To choose the ideal treatment, one must consider the location of the tumor (hands or feet), age of the patient, main complaint (pain, discomfort, or cosmetic alteration), the life cycle of the tumor (primary or recurrent), number of lesions, and comorbidities.7
Surgical excision of the lesions is effective and inexpensive, not requiring specific devices. This treatment is preferable in patients with low surgical risk, recurrent tumors, extensive and multiple, especially in the feet. The aesthetic result is usually satisfactory.7 Given the above, we chose the surgery in our case due to the minimal surgical risk, the presence of large and multiple lesions, especially on the feet, in addition to nail deformities and the need for functional resolution.
Regarding the other therapeutic modalities, there is the CO2 laser, which directs bundles of light waves until the complete vaporization of the tumor. It has a low risk of bleeding, short duration (about 10 seconds per lesion), in addition to a satisfactory aesthetic result and excellent healing. It may be a proper choice for patients with surgical contraindications, small and moderate lesions, especially in the hands.4,5
Shave excision followed by phenolization involves removing the protruding portion of the tumor and applying phenol to the lesion base. This method allows the preservation of the matrix and the nail plate, being more used in patients with high surgical risk, prioritizing the aesthetic result, and patients with small tumors and preferably located in the hands.7 Possible complications are necrosis, infection, and deformities of the fold and nail plate, which are rare.9 We did not choose this option due to the high risk of worsening nail dystrophy.
For aggressive, recurrent KTs with a high degree of morbidity, amputation of nail devices and reconstruction by full-thickness skin graft presents the possibility of an effective result.2
Another option is rapamycin, which belongs to the class of immunosuppressants. This medication inhibits mTOR (mammalian target of rapamycin), suppressing vascular growth factors, and destroying tumor cells. Its topical use shows promising results for the treatment of subungual fibroma. It is considered safe and well-tolerated, with rapid lesion involution. The recommendation is to use it twice a day, providing the clinical picture’s initial improvement in just two months and the total disappearance of the lesions after six months.8
So far, there is no gold standard treatment in the literature for TK.7 The decision must be based on the advantages and disadvantages of each method. We report the case of a patient successfully treated for fibroma after surgical approach, with healing, excellent aesthetic and functional results, without complications, and without recurrence of the lesions in the first eight months of follow-up.
Amanda Bertazzoli Diogo | 0000-0002-2708-3139 Approval of the final version of the manuscript; study design and planning; preparation and writing of the manuscript; data collection, analysis, and interpretation; active participation in research orientation; intellectual participation in propaedeutic and/or therapeutic conduct of studied cases; critical literature review; critical revision of the manuscript.
José Roberto Pegas | 0000-0002-2541-6008 Approval of the final version of the manuscript; study design and planning; data collection, analysis, and interpretation; active participation in research orientation; intellectual participation in propaedeutic and/or therapeutic conduct of studied cases; critical literature review; critical revision of the manuscript.
Mariana de Freitas Valente | 0000-0002-6798-7116 Approval of the final version of the manuscript; preparation and writing of the manuscript; critical literature review; critical revision of the manuscript.
Cristina Santos Ribeiro Bechara | 000-0002-7723-2980 Approval of the final version of the manuscript; preparation and writing of the manuscript; critical literature review; critical revision of the manuscript.
1. Rodrigues DA, Gomes CM, Costa IM. Tuberous sclerosis complex. An Bras Dermatol. 2012;87(2):185-97.
2. Oliveira GB, Rossi NCP, Cury DO, Coura MGG, Antonio, CR. Tumores de Köenen exuberantes: tratamento efetivo com amputação do aparelho ungueal e reconstrução com enxerto de pele de espessura total. Surg Cosmet Dermatol. 2017; 9(2):187-9.
3. Aldrich CS, Hong CH, Groves L, Olsen C, Moss J, Darling TN. Acral lesions in tuberous sclerosis complex: insights into pathogenesis. J Am Acad Dermatol. 2010; 63(2):244-51.
4. Sechi A, Savoia F, Patrizi A, Sacchelli L, Neri I. Dermoscopy of subungueal red comets associated with tuberous sclerosis complex. Pediatr Dermatol. 2019;36(3):408-10.
5. Berlin AL, Billick RC. Use of CO2 laser in the treatment of periungual fibromas associated with tuberous sclerosis. Dermatol surg. 2002;28(5):434-6.
6. Nguyen QD, DarConte MD, Hebert AA. The cutaneous manifestations of tuberous sclerosis complex. Am J Med Genet C Semin Med Genet. 2018; 178(3):321-5.
7. Liebman, JJ, Nigro, LC, Matthews, MS. Koenen tumor in tuberous sclerosis. Ann Plast Surg. 2014;73(6):721-2.
8. Muzic JG, Kindle SA, Tollefson MM. Successful treatment of subungual fibromas of tuberous sclerosis with topical rapamycin. JAMA Dermatol. 2014;150(9):1024-5.
9. Mazaira M, del Pozo Losada J, Fernández-Jorge B, Fernández-Torres R, Martinez W, Fonseca E. Shave and phenolization of periungual fibromas, Koenen's tumors, in a patient with tuberous sclerosis. Dermatol Surg. 2008;34(1):111-3.
 All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773
All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773



 Read in Portuguese
Read in Portuguese
 Portuguese PDF
Portuguese PDF
 Print
Print
 Send this article by email
Send this article by email
 How to cite this article
How to cite this article
 Submit a comment
Submit a comment
 Mendeley
Mendeley
 Pocket
Pocket
{kind=link}
{kind=link}
{kind=link}
{kind=link}