


Fernanda Catarina Ribeiro; Anndressa Camillo da Matta Setubal Gomes; Aline Lucy Galavotti Silveira;
Received on: 02/12/2019
Approved on: 12/08/2020
Financial support: None
Conflict of interest: None
Acknowledgement: The authors would like to thank Dr. Geldo Regis Moreira, Dr. Ana Luiza Alves Monteiro, Dr. Flavia Albuquerque de Rezende Dutra, Dr. Fernanda Soncini, Dr. Luciana Torrico Zubelli and Dr. Aline Fassini for their assistance in preparing of this report
Study conducted at the Department of Dermatology, Marcílio Dias Naval Hospital, Rio de Janeiro (RJ), Brazil
Onychomatricoma is a rare tumor of the nail complex of unknown etiology. It has a higher incidence in women in the 5th decade of life. However, this occurrence may be mistaken due to data and information that have not yet been fully elucidated. This study aims to review the literature and report two cases of onychomatricoma. We included two male patients with different age ranges and different tumor presentations. This study shows that the rarity and incidence reported in the literature are questionable and that the onychomatricoma can be underdiagnosed.
Keywords: Dermoscopy; Onychomycosis; Pathology, Clinical
The onychomatricoma is a rare and benign tumor of the nail complex, first described in 1992 by Baran and Kint. The classic tetrad characterizes it: xanthonychia, subungual hyperkeratosis, splinter hemorrhages affecting the nail plate, longitudinal and transverse hypercurvature of the nail plate.1,2,3,4,5,6 Thus, underdiagnosed conditions, confusion with specific differential diagnoses, or even the lack of knowledge about the tumor by some dermatologists justify the rarity of this condition.
Its etiology is still unknown.5,6,7 However, recent studies are in a continuous investigation for this motivation, assessing genetic and environmental conditions, risk factors, profession, history of trauma, domestic and/or aesthetic habits, and even associated diseases, suggesting new hypotheses for this tumor’s cause.
The onychomatricoma affects mainly women, with a higher occurrence in the 5th decade of life. 1,5,6,7,8 However, the present reported cases are of men, aged 42 and 64 years, respectively. This incidence may be wrong given specific data and information that have not yet been correctly clarified.
Most studies have related onychomycosis as a confounding factor.1,3,5,6 Thus, many patients are initially treated with antifungal drugs for years. It is possibly a justification for late diagnoses and, also, for underdiagnosed cases, reducing the percentage of reported cases and, consequently, the incidence rate, inducing to believe in the disease’s rarity.
Clinical characteristics can suggest the diagnosis, and it is more easily evidenced when it appears classically, grouped in a tetrad.
Complementary diagnostic methods guide the diagnosis, such as dermoscopy, ultrasound, and anatomopathological study.1,2,5,6,7 Other more recent exams present innovative ways for diagnostic purposes, as pointed out in some reports, expanding the possibilities for unveiling new cases of this tumor.
Treatment is complete local excision performed as a curative mean.1,5,6 Concomitantly with therapy, the anatomopathological study of the skin fragment is conducted to clarify the disease. There is a possibility to develop nail dystrophy after the surgical procedure, making this explanation necessary to the patient before the surgical approach. Therefore, it is plausible that some patients refuse to undergo surgery due to this disorder, reducing the number of confirmed cases.
This study aims to conduct a literature review with to expand the knowledge of dermatologists on the tumor, demonstrating various techniques to determine the disease, and reporting two cases of onychomatricoma with unequal presentations in men with different age groups, who obtained their diagnoses by different methods.
Two men with onychomatricoma, with different age groups, and different tumor presentation locations, were included. They obtained their diagnosis by the tumor’s clinical manifestation; however, the complementary methods to determine the diagnosis were unequal. Case 1 presented with nail onychodystrophy in the left hallux. After performing an anatomopathological examination, it showed compact hyperkeratosis, agranulose and acanthosis compatible with onychomatricoma. In the second case, the third finger’s dermoscopy revealed splinter hemorrhage, xanthonychia, subungual hyperkeratosis, and longitudinal hypercurvature of the nail plate, which constituted the classic tetrad. Still, radiography of the right hand was performed, showing no bone changes, and corroborating the diagnosis of neoplasia.
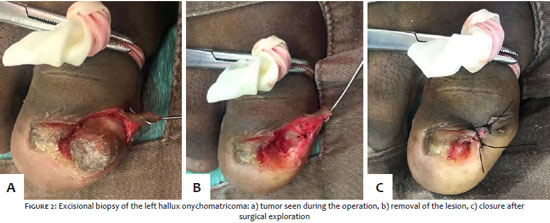
The patient mentioned previous trauma to the same toe ten years ago and reported mild pain when putting on his shoes, without other symptoms. He also explained that he had performed direct mycological examination and nail plate culture seven years ago, with a positive result for Candida sp, with topical antifungals being prescribed, with no success.
We performed radiography of the left foot, which did not reveal bone involvement. Based on this data, the possibility of a benign tumor of the nail complex was suspected. Then, we decided to perform an excisional biopsy (Figure 2), sending the material to the pathologist to confirm the diagnosis of onychomatricoma.
A 64-year-old man, skin phototype III, driver, with benign prostatic hyperplasia, systemic arterial hypertension, and peripheral arterial disease, presented to the Dermatology Service to assess an asymptomatic lesion located in the 3rd right finger, which appeared ten years ago, with a history of previous trauma.
He reported previous empirical topical treatments for onychomycosis, with no success. The clinical examination found subungual hyperkeratosis and longitudinal hypercurvature on the nail plate.
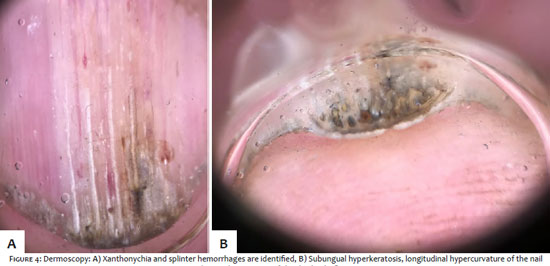
Dermoscopy observed the presence of xanthonychia, splinter hemorrhages, subungual hyperkeratosis, and longitudinal hypercurvature on the nail plate (Figure 3), suggesting the clinical and dermoscopic diagnosis of onychomatricoma (Figure 4). Radiography and computed tomography of the right hand were also performed, showing no bone involvement, and corroborating the tumor condition’s determination.
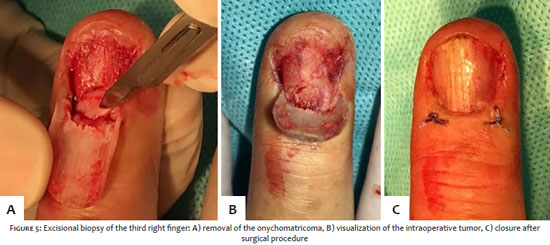
Subsequently, we performed the histopathological study by excisional biopsy (Figure 5), revealing in the microscopic examination discrete projections of the epidermal cones in the superficial dermis amid hyalinized collagen, mild solar elastosis, and vasodilation.
Altogether, the clinic, dermoscopy, imaging exams, and anatomopathological study help define the condition as onychomatricoma.
First described in 1992 by Baran and Kint,1,2,3,4,5,6,9 onychomatricoma is a rare and benign fibroepithelial neoplasm of the nail complex.1,2,3,4,5,6,7,9,10,11 The plurality of studies points to the nail matrix as the original site of the tumor. However, Mello et al. suggest its beginning in cell differentiation areas with matrix cells (metaplasia), which may be the portions of the proximal fold or the nail bed. Therefore, the hesitation in determining this neoplasm’s genesis also implies a lack of knowledge on the subject.
The onychomatricoma so far presents uncertain etiology.1,3,4 However, predisposing factors have been documented, such as onychomycosis and a history of previous trauma.1,5,6 In contrast, the study by Kallis and Tosti states that the tumor is the causative factor of onychomycosis due to the cavitations formed by the digitiform projections inside the nail plate, making the environment favorable for the invasion of fungi.
Nail mycosis is an extremely relevant point when addressing the onychomatricoma theme. Onychomycosis is reported from different perspectives: as a pathology caused by the tumor; as a precursor agent; as a disturbing factor for diagnosis; and, also, a complicating factor of the neoplasia.
Due to similar clinical and dermoscopic characteristics, the tumor is possibly initially diagnosed as onychomycosis and often treated as such,1,2,4,7 delaying its diagnosis and complicating the onychomatricoma condition. It is possible that, in some cases, the pathologies can indeed coexist, which contributes even more to the percentage of underdiagnosed cases of the tumor.
Some current studies (Table 1) describe trauma cases before the onychomatricoma, both accidental due to crushing6 or even due to small and repeated bruises, as in the case of a toolmaker.3 Such information allows us to conclude that the type of trauma is separated from the tumor’s occurrence and that the profession can be considered a risk factor.
In the present study, there was a history of previous trauma ten years ago in both cases. However, in other studies, patients deny previous trauma. There is also a single report of a four-year-old girl with onychomatricoma but without a history of pre-existing trauma,6 so it is hypothesized that this patient was predisposed due to onychomycosis.
Predisposing factors must be continually evaluated during anamnesis to collect a greater amount of data for medical research purposes, correctly defining information about the tumor.
The tumor is more prevalent in Caucasian women, with a peak incidence in the 5th decade of life,1,3,4,5,6,7,9 although some studies indicate that the development of the onychomatricoma has no preference for sex.7,10,12
In the reports of this study, both patients are men aged 42 and 64 years, respectively. The patient in case 1 has skin phototype V, making it another different data for the research statistics.
Most of this information may be mistaken, as analyzed in Table 1. This mistake probably occurs due to socio-cultural and environmental factors, such as aesthetics, care for personal health, profession, and even underdiagnosed cases or cases mistakenly treated as onychomycosis.
Recent information exposes that fingers are more commonly affected than toes, with 63% and 36% prevalence, respectively, and the disease may affect only a single finger or simultaneously.3,7,9,10 Nevertheless, diagnostic errors are common due to confusion with nail mycosis, and the true incidence in the lower extremity remains to be determined.
As shown in Table 1, it is possible to assess a disagreement between the literature’s statistical data and the present reports’ information. For this reason, the reported uncertainty may reveal to us how much more research is still needed.
The tumor extends digitiform projections of the matrix that penetrate the “nail plate”, causing thickening of the nail plate, xanthonychia, splinter hemorrhage, transverse and longitudinal hypercurvature, characterizing the clinical tetrad.1,2,4,5,6,7,9,10,11,12
Other findings may be present, including longitudinal groove, subungual hematoma, verrucosity of the proximal nail fold, erythema and edema of the proximal fold, longitudinal melanonychia, onychodystrophy, and dorsal pterygium.3,4,5
The onychomatricoma contains several differential diagnoses, such as onychomycosis, which represents 50% of nail disorders; nail and periungual tumors: digital fibrokeratoma and subungual fibroma; Bowen’s disease; common subungual wart; osteochondroma; squamous cell carcinoma; longitudinal melanonychia, and subungual exostosis.1,2,4,6,7,12
Fibrokeratoma and nail fibroma are considered the primary tumors for differential diagnoses. In the longitudinal sections of the onychomatricoma, the lesion resembles the first, and the stroma located in the lunula can also suggest the second. However, the presence of digitiform projections excludes these diagnoses.6
The diagnosis is based on the classical tetrad signs and additional methods, such as dermoscopy, ultrasound, and histopathology, the latter being considered the gold standard.1,2,3,4,5,7,9 Other studies include, as complementary exams, magnetic resonance imaging, radiography, nail clipping, and confocal microscopy.1,4,5,9,10
After surgical exploration, there is a possibility of permanent nail dystrophy. Therefore, this probable event should be informed to the patient and communicate that the tumor has an indolent nature and without any malignant potential, being possible to maintain only clinical follow-up if it is asymptomatic. Thus, the patient can develop an understanding to evaluate the need for surgery together with the dermatologist.
Given the above, some patients choose not to perform the procedure. Countless cases may be ignored and not documented, contributing to reducing the percentage of its incidence.
It is possible to see perforations in the distal portion of the nail plate, hemorrhagic streaks, and longitudinal white grooves corresponding to the nail plate’s channels in dermoscopy.1,2,4,7,9,10
X-ray examination shows no underlying bone involvement linked to the onychomatricoma.3,7,10 In the present reported cases, the radiography did not reveal erosion or bone remodeling, reinforcing the suspected diagnosis of the tumor.
The ultrasound examination reveals a hypoechoic tumor lesion affecting the nail matrix and a hyperechogenic area corresponding to the digitiform projections.1,4,7,9,10
Magnetic resonance imaging points to the nail matrix with low signal uptake, while the distal digitiform projections show high uptake.1,4,9,10 This imaging method should be considered for dystrophic nails with negative mycological tests. So far, there are no other lesions reported in the literature that have the same presentation as this tumor, becoming specific.9
Another possible exam to be performed is nail clipping, which corresponds to the plate’s distal cut, studied histologically, revealing peculiar characteristics such as thickening of the nail blade, cavitations filled with serous material, and periphery with a thin layer of epithelium.4 Nail clipping presents itself as an easy and minimally invasive resource, aiding in the diagnosis, and excluding associated fungal infections.
Confocal microscopy was used in four cases, and it seemed useful in the preoperative diagnosis of the onychomatricoma, thus being another available method.9
Histologically, the onychomatricoma is a fibroepithelial tumor comprising two different zones: the proximal and the distal. The first, located below the posterior nail fold, is characterized by having deep epithelial invaginations occupied by overlapping nail protrusions, in the shape of V. The second, still a distal zone, corresponding to the lunula, contains epithelial originating from the matrix epithelium, which proliferates and causes perforations in the nail plate.1,3,6,7,10
Treatment consists of complete surgical excision, including the entire proximal matrix, to avoid local recurrence.1,4,5,6,7,10,12 The long-term prognosis seems favorable since there is only one case of recurrence reported so far.
After anesthesia, an avulsion of the nail plate is performed, allowing the visualization of the tumor projections that will be removed.4,7 For symptomatic tumors, tangential excision is preferable to avoid onychodystrophy. However, there is a risk of incomplete removal.6 It is plausible that this sequelae will be permanent if the tumor is larger than 3mm.13
Mohs surgery allows tumor distancing with minimal removal of the affected nail matrix and, thus, minimizes the potential aesthetic and functional impacts of the surgery.10 It is possible that, in the future, this technique will be performed in most cases, encouraging greater medical demand for both diagnosis and treatment.
In short, the onychomatricoma remains a rare tumor, but statistical data on its epidemiology is doubtful.
Its tendency to be asymptomatic and the misdiagnosis of onychomycosis favor diagnostic difficulties. There is a need to raise the rate of clinical suspicion when a single nail is affected or if topical antifungals do not achieve therapeutic success, or even if there is a history of trauma.
The histopathological examination must confirm the diagnosis when the classical tetrad does not reveal the tumor. However, the variety of complementary tests currently used facilitates diagnostic suspicion. It is essential to report that more recent methods are being introduced, minimizing the aesthetic impact and contributing to patients’ acceptance of research.
The gold standard for treatment is complete surgical excision. However, knowledge of appropriate surgical techniques is essential to prevent tumor recurrence and possible onychodystrophy.
We reported two cases of onychomatricoma to expand the disease’s knowledge; after all, it is still a diagnostic challenge.
This study allowed a new question: is the diagnostic difficulty due to the rarity of the onychomatricoma, or is it due to the dermatologists’ insufficient knowledge?
Fernanda Catarina Ribeiro | 0000-0001-5447-4250 Statistical analysis; approval of the final version of the manuscript; study design and planning; preparation and writing of the manuscript; data collection, analysis, and interpretation; active participation in research orientation; intellectual participation in propaedeutic and/or therapeutic conduct of studied cases; critical literature review; critical revision of the manuscript.
Anndressa Camillo da Matta Setubal Gomes | 0000-0002-9074-645X Active participation in research orientation.
Aline Lucy Galavotti Silveira | 0000-0001-5316-3960 Active participation in research orientation.
1. Joo HJ, Kin MR, Cho BK, Yoo G, Park HJ. Onychomatricoma: A rare tumor of nail matrix. Ann Dermatol. 2016;28(2):237-41.
2. Belda Junior W, Chiacchio N, Criado PR. Tratado de Dermatologia. 3th ed. São Paulo: Atheneu, 2019.
3. Kallis P, Tosti A. Onicomicose e onychomatricoma. Skin Appendage Disord. 2016;1(4):209-12.
4. Kamath P, Wu T, Villada G, Zaiac M, Elgart G,Tosti A. Onychomatricoma: a rare nail tumor with an unusual clinical presentation. Skin Appendage Disord 2018;4(3):171-3.
5. Rushing CJ, Ivankiv R, Bullock NM, Rogers DE, Spinner SM. Onychomatricoma: a rare and potentially underreported tumor of the nail matrix. J Foot Ankle Surg. 2017; 56(5):1095-98.
6. Tavares GT, Chiacchio N, Chiacchiob NG, Souza MV. Onicomatricoma: um tumor desconhecido pelo dermatologista. An Bras Dermatol. 2015;90(2):268-70.
7. Mello CDBF, Noriega LF, Chiacchio NG, Campos-Garzac JC, Chiacchio N. Onychomatricoma of the nail bed. Skin Appendage Disord. 2019;5(3):165-8.
8. Madi A, Meguerian ZB, Kanj VC, Bakhach J. Pigmented onychomatricoma may originate from a childhood trauma: a case report. Hand Surg Rehabil. 2019;38(6):386-9.
9. Charfi O, Jaber K, Khammouma F, Rabhi F, Youssef S, Dhaoui R, Doss N. Magnetic resonance imaging in the diagnosis of onychomatricoma: a case report. Skin Appendage Disord. 2019;5:246-50.
10. Mundada P, Becker M, Lenoir V, Stefanelli V, Rougemont AL, Beaulieu JY, et al. High resolution MRI of nail tumors and tumor-like conditions. Eur J Radiol. 2019;112:93-105.
11. Park SJ, Ahn GR, Hong JY, Seo SJ. A case of veiled onychomatricoma. Eur Acad Dermatol Venereol. 2019;33(11):e420-22.
12. Tambe SA, Ansari SMM, Nayak CS, Chokkar R, Patil PD. Surgical management of onychopapilloma, Onychomatricoma, and subungual osteochondroma: case series. J Cutan Aesthet Surg. 2018;11(3):143-7.
13. Nakamura R, Baran R. Doenças da Unha. 2nd ed, Rio de Janeiro: Elsevier; 2018.
14. Zou XK, Yu J, Yang SX. Image gallery: a case of onychomatricoma with typical clinical, dermoscopic and histopathological findings. British J Dermatol. 2019;181(6):e146.
 All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773
All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773



 Read in Portuguese
Read in Portuguese
 Portuguese PDF
Portuguese PDF
 Print
Print
 Send this article by email
Send this article by email
 How to cite this article
How to cite this article
 Submit a comment
Submit a comment
 Mendeley
Mendeley
 Pocket
Pocket
{kind=link}
{kind=link}
{kind=link}
{kind=link}