


Nelson Marcos Ferrari Junior; Daniel Luiz Marques Gonçalves
Received on: 21/12/2019
Approved on: 12/08/2020
Financial support: None
Conflict of interest: None
Study conducted at the Hospital das Clínicas, Faculty of Medicine, University of São Paulo, São Paulo (SP), Brazil
The digital myxoid cyst is a benign lesion of controversial origin, usually in the distal phalanx, close to the posterior nail fold. Clinical picture or imaging techniques, such as ultrasound and magnetic resonance imaging, can help diagnose the condition. It may present with discomfort to patients because it is often painful. There are several possible treatments, such as surgical excision and suturing, with or without grafting, cryotherapy, electrocoagulation, and curettage. However, it presents high recurrence rates. In this paper, we propose a simple, fast, and low-cost method for treating digital myxoid cyst, so far with low recurrence rates.
Keywords: Ambulatory Surgical Procedures; Dermatology; Nails
Myxoid cyst is a benign tumor whose origin is still controversial. It may be caused by minor trauma that degenerates the connective tissue into mucoid material or would derive directly from the adjacent interphalangeal joint, damaged by osteoarthritis osteophytes, leading to the formation of a 5-20 mm in diameter rounded nodule. The cysts affect the fingers of the hands and feet, but especially the hands, and usually occur near the distal joints of the fingers.1
The cysts can be painful and sometimes, when periungual, can produce grove or structural changes in the nail lamina that are reversible with treatment, which is evidence of the benignity of the lesion, since malignant lesions usually produce permanent onychodystrophy, due to the invasion of the matrix and not just compression.1
The diagnosis is made by high-resolution ultrasound or magnetic resonance imaging, but can be made by transillumination with a small flashlight or by puncturing with a large needle, revealing the transparent mucous material inside.
The histologic exam presents a focal deposition of mucin in the dermis with surrounding fibrous stroma and no epithelial lining; mucin can be highlighted by the alcian blue and colloidal iron stains.
Several treatments are described in the literature2,3, such as electrocoagulation and cryotherapy4, both with significant relapse rates and even surgery5, with higher cure rates, which is the first choice especially under the matrix¹. In this article, we will demonstrate a simple, safe and that has shown very satisfactory results technique.
After local asepsis, the cyst contents are emptied through a needle (40x1.2 mm/18 G11/ 2”). Digital nerve block may be performed, but the procedure usually generates little discomfort to the patient.
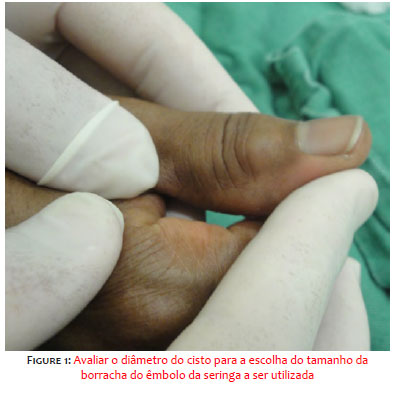
Depending on the diameter of the cyst (image 1), the size of the syringe plunger rubber to be used should be chosen.
The rubber should be placed above the emptied cyst (image 2) and with the aid of micropore fixed by compression, thus collapsing the walls of the cyst together (image 3).
The secret to the success of the method is to tell the patient not to remove this bandage for at least 15 days, as this will allow the cyst to “heal”, leading to the definitive collapse of the walls, preventing recurrence (image 4).
During a six months follow up, there were not relapses, except in those who lost the dressings early, not reaching the recommended time of 15 days. In these cases, relapse occurs in a matter of days.
In the treatment of the mucous cyst, we had seen recurrences even after procedures such as removal by saucerization followed by electrocoagulation of the internal base of the cyst, close technique cryotherapy for 45 to 60 seconds with a probe compressing the cyst walls, both techniques with high morbidity rate; or even surgical excision of the cyst, whether or not followed by local graft.
With higher recurrence rates for the first two methods and for simple excision and slightly lower for cases in which total skin grafting was applied under a Brown dressing.
This is evidence that optimal treatment does not depend on tissue destruction, but rather on effective and lasting local compression that allows the inner walls of the cyst to reestablish and recap.
Despite the compression applied for a period of 15 days, we have not yet witnessed local necrosis. Even if this happens, it should not be something to fear, as the recommended procedures for treatment of myxoid cysts, such as electrocoagulation or cryotherapy, generate local necrosis.
Myxoid cyst is a benign lesion that should be treated conservatively.5 The method described above should be used because it is a simple, fast, inexpensive, and easy procedure, with no major complications observed so far, and can be performed in the office during the initial consultation of the patient. As a disadvantage, we point out the inconvenience that it is necessary for the patient to remain with the dressing for an extended period, which, if not performed, may impair the effectiveness of the method.
Nelson Marcos Ferrari Junior | 0000-0002-2034-8042 Approval of the final version of the manuscript; study design and planning; preparation and writing of the manuscript; data collection, analysis, and interpretation; intellectual participation in propaedeutic and/or therapeutic conduct of studied cases; critical literature review.
Daniel Luiz Marques Gonçalves | 0000-0002-7060-0162 Preparation and writing of the manuscript; critical literature review; critical revision of the manuscript.
1. De Berker D, Goettman S, Baran R. Subungual myxoid cysts: clinical manifestations and response to therapy. J Am Acad Dermatol. 2002;46:394-8.
2. Baran R, Haneke E. Tumors of the nail apparatus and adjacent tissues. In: Baran R,Dawber RPR, eds. Diseases of the nails and their management. 2nd ed. Oxford: Blackwell Sience; 1994. p. 474-6.
3. Becker D. Treatment of myxoid cysts. J Dermatol Treat. 1995;6:55-7.
4. Dawber RPR, Colver G, Jackson A, Cutaneous Cryosurgery. Principles and clinical practice. London: Dunitz, 1992:71-2.
5. Salache SJ. Myxoid cysts of the proximal nail fold, a surgical approach. J Dermatol Surg Oncol. 1984;10:35-9.
 All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773
All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773



 Read in Portuguese
Read in Portuguese
 Portuguese PDF
Portuguese PDF
 Print
Print
 Send this article by email
Send this article by email
 How to cite this article
How to cite this article
 Submit a comment
Submit a comment
 Mendeley
Mendeley
 Pocket
Pocket
{kind=link}
{kind=link}
{kind=link}
{kind=link}