


Mabel Duarte Alves Gomides1; Alceu Luiz Camargo Villela Berbert2
Received on: 07/09/2019
Approved on: 02/11/2020
Financial support: None
Conflict of interest: None
Acknowledgment: We thank the residents Nayara Fayad Souza Dib and Núbia Carvalho Pena de Oliveira Praeiro Alves, who participated in the case report under the guidance of assistant physician Dr. José Joaquim Rodrigues
Study conducted at the Dermatology Service, Hospital de Clínicas, Federal University of Uberlândia, Uberlândia (MG), Brazil
Proliferating Trichilemmal Tumor (PTT) is an uncommon benign neoplasm that usually affects adult women over 60 years old, preferably as a solitary nodule in the scalp. We report a case of PTT in a young woman presenting exuberant, asymptomatic scalp tumors 7 years ago, which recurred after surgical exeresis. The histopathology confirmed the diagnosis, and surgical excisions and clinical follow-up were performed. PTT appears to originate from the wall of trichilemmal cysts, from the isthmus of the hair follicle’s outer root sheath. Usually, it has benign biological potential with a low risk of malignancy and high recurrence. The therapy of choice is surgery.
Keywords: Cysts; Neoplasms; Scalp
Proliferating trichilemmal tumor (PTT) is an epidermal adnexal neoplasia formed by several cysts containing squamous epithelium with trichilemmal keratinization, in other words, the abrupt transition of a nucleated epithelial cells to an anucleated in the absence of a granular layer.1-3 PTT usually appears as a dermal nodule or solitary subcutaneous scalp of elderly women.1,3-13 It was first described by Wilson-Jones in 1966, who named it a proliferating epidermoid cyst due to its clinical and histological resemblance to squamous cell carcinoma.1,3, 5,9-13 Since then, PTT has received several other names, such as scalp pilaris tumor, proliferating trichilemmal cyst, trichilemic pillar tumor, invasive pilomatrixoma, hydatid keratinous cyst, trichoclamidocarcinoma, giant hair matrix tumor, hairy scalp tumor, and others.1,3,6 It exhibits the ability to grow rapidly over a given period of time, but the evolution to malignant PTT is uncommon.5,7,11,12 Therefore, it presents heterogeneous histological behaviors ranging from benign, locally aggressive growth with chances of causing invasions in the underlying tissue layers up to that time. with local recurrence metastatic potential and regional lymph node metastasis.3,10,11,12 PTT is a rare tumor that corresponds to 0.1% of benign cutaneous tumors and may form from a pre-existing or concomitant trichilemmal cyst or as an isolated lesion.5,11,12
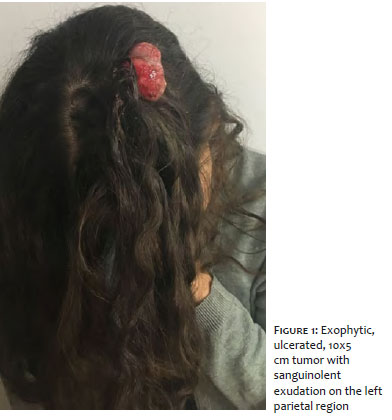
We report the history of a 24-year-old female patient from Uberlândia (MG), treated at the dermatology department of the Clinical Hospital of the Federal University of Uberlândia, complaining of painless nodules in scalp for seven years ago. It refers to progressive growth in recent months, followed by ulceration with output of bloody discharge. Reports recurrence of previously excised scalp lesions. She denies having suffered any kind of trauma.
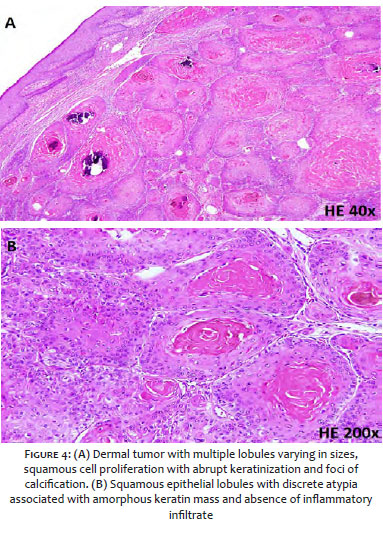
Dermatological examination showed exophytic, painless, ulcerated tumor with sanguinolent exudation, measuring 10x5 cm in size, in the left parietal region (figure 1), and several other smooth-surface tumors, soft consistency, measuring 1 to 3 cm in diameter, distributed on the scalp, some surrounded by alopecia (figure 2). There was no palpable adenomegaly in the cervical and scalp. Two lesions were excised (figure 3), whose pathological examination showed squamous cell proliferation in the dermis with formation of tumors with irregular multiple lobules of varying sizes, differentiating into large keratinocytes with discrete atypia, abrupt keratinization with foci of calcification and absence of invasion of adjacent tissues (figure 4).
Trichilemmal tumor, pilomatrixoma, protuberant dermatofibrosarcoma was clinically suspected, but the correlation between clinical and histopathological findings confirmed the diagnosis of PTT.
Surgical treatment of some lesions has been proposed, with wide margin exercises and simple interrupted suture with good healing results. Due to the recurrent nature of the lesions, the patient remains in outpatient clinical follow-up and other injuries are scheduled.
Trichilemmal cysts correspond to 20% of cutaneous cysts, the others classified as epidermoid cysts originating from trichilemmal or external root sheath of the hair follicle.1,11 PTT seems to originate from these lesions, presumably after inflammation or trauma, due to the fact that have areas with benign characteristics and others with malignant properties.1,5-12 It differs from the trichilemmal cyst because it is uncommon, larger, and histologically more atypical, and the malignant proliferative trichilemmal tumor is less aggressive.9 PTT occurs more frequently in women (79,5-87% of cases) with ages ranging from 21 to 88 years, mean 62.4 years, despite reports in children under 18 years.1,3,5,10-12 Lesions are usually solitary nodules, smaller than 1 cm to 12 cm (average 3.3 cm), although there are citations of multiple nodules, sometimes ulcerated and larger than 25 cm.3,10-13 It often presents a history of slow and progressive growth from months to years, followed by fast growth and exophytic appearance.2,10,12 The preferred location is the scalp (85.4-90% of cases) and sometimes has alopecia.1,3,5,10-13 The remaining 10% are mostly on the back and more rarely elsewhere, such as frontal, nose, eyelids, lips, oral cavity, neck, trunk, genital, buttocks, upper and lower limbs, and skull base.1,3,5,10-12 The reported case manifested unusual features, such as the onset of PTT at 17 years, the presence of multiple nodules and some ulcerated lesions. Most of the PTT presents benign biological behavior, but with a chance of recurrence, in a period of six months to more than 10 years after surgery, especially in cases of cleft excision , and in very rare cases may have malignant biological potential.3, 5,10-12 Local recurrence rates (3.7%) and lymph node metastasis (1.2%) are low, but when occur they may cause invasion into deep tissue planes by continuity, contiguity or spread, resulting in high morbidity rates and even mortality.3,5,10-12 Some studies have shown the importance of researching Ki-67 immunoexpression, a protein responsible for cell proliferation, because the expression index correlates with the degree of malignancy of the tumor.7,8 The differential diagnosis of PTT includes squamous cell carcinoma, basal cell carcinoma, keratoacanthoma, pilomatrixoma, sweat gland tumor, protuberant dermatofibrosarcoma, cylindroma, epidermoid cyst, malignant PTT, and angiosarcoma.1,4,11 Histopathological findings of squamous epithelium lobules, cells with abundant eosinophilic cytoplasm with abrupt keratinization, variable cytological atypia and absence of infiltration into adjacent stroma.1,4,12,13 PTTs are recurrent and potentially invasive, so, the therapy of choice is surgeries with a margins of 0.5 to 1 cm.5,7,9-12 Among surgical techniques, Mohs’ micrographic surgery has a good indication, because its margins may to exceed visible clinical limits and thus reduce the risk of relapse and metastasis.5,9,11 Other treatments such as lymph node dissection, radiotherapy, and chemotherapy may be required in cases of metastatic dissemination or transformation to malignant PTT.5,11 Therefore, long-term follow-up is indispensable.7,10-12
Mabel Duarte Alves Gomides | 0000-0003-1253-9428 Approval of the final version of the manuscript; study design and planning; preparation and writing of the manuscript; active participation in research orientation; intellectual participation in propaedeutic and/or therapeutic conduct of studied cases; critical literature review; critical revision of the manuscript.
Alceu Luiz Camargo Villela Berbert | 0000-0001-8441-7388 Approval of the final version of the manuscript; intellectual participation in propaedeutic and/or therapeutic conduct of studied cases.
1. Peryassu MA, Peryassu BC, Peryassu RC, Piñeiro-Maceira J, Ramos-e-Silva M. Proliferating trichilemmal tumor: a case on the nose of a 70-year-old man. Case Rep Dermatol. 2013;5:248-53.
2. Rosmaninho A, Caetano M, Oliveira A, Almeida TP, Selores M, Alves R. Tumor triquilemal proliferante do nariz. An Bras Dermatol. 2012;87:914-6.
3. Ye J, Nappi O, Swanson PE, Patterson JW, Wick MR. Proliferating pilar tumors: a clinicopathologic study of 76 cases with a proposal for definition of benign and malignant variants. Am J Clin Pathol. 2004;122:566-74.
4. Miyachi H, Togawa Y, Yamamoto Y, Oguma R, Suehiro K, Matsue H. Proliferating trichilemmal tumour: a comparison of dermoscopic, ultrasonographic and histopathological features. Eur J Dermatol. 2016;26:400-2.
5. Capurso-Garcia MA, Bautista-Piña V, Pomerantz A, Galnares-Olalde JA, Blachman-Braun R, Rodríguez-Rodríguez S. Atypical proliferating trichilemmal cyst with malignant breast skin transformation: a case report and review of the literature. Case Rep Oncol Med. 2016:7481569. Epub 2016 Jun 14.
6. Deshmukh BD, Kulkarni MP, Momin YA, Sulhyan KR. Malignant proliferating trichilemmal tumor: a case report and review of literature. J Cancer Res Ther. 2014; 10:767-9.
7. Rangel-Gamboa L, Reyes-Castro M, Dominguez-Cherit J, Vega-Memije E. Proliferating trichilemmal cyst: the value of Ki67 immunostaining. Int J Trichology. 2013;5:115-7.
8. Takeda H, Ikenaga S, Kaneko T, Nakajima K, Harada K; Hanada K et al. Proliferating trichilemmal tumor developing in nevus sebaceous. Eur J Dermatol. 2010; 20:664-5.
9. Cavaleiro LH, Viana FO, Carneiro CM, Miranda MF. Proliferating trichilemmal tumor - Case Report. An Bras Dermatol. 2011;86:S190-2.
10. ury Y, Bloxham C. Proliferating trichilemmal tumour. Diagn Histopathol. 2009; 15:273-7.
11. Satyaprakash Ak, Sheehan Dj, Sangüeza Op. Proliferating trichilemmal tumors: a review of the literature. Dermatol Surg. 2007;33:1102-8.
12. Arcaute LB, Taveras A, González L. Tumor triquilemal proliferante maligno. A propósito de un caso. DermatologíaCMQ. 2005;3:346-8.
13. Fonseca TC, Bandeira CL, Sousa BA, Farias TP, Eisenberg ALA. Proliferating trichilemmal tumor: case report. J Bras Patol Med Lab. 2016;52:120-3.
 All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773
All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773



 Read in Portuguese
Read in Portuguese
 Portuguese PDF
Portuguese PDF
 Print
Print
 Send this article by email
Send this article by email
 How to cite this article
How to cite this article
 Submit a comment
Submit a comment
 Mendeley
Mendeley
 Pocket
Pocket
{kind=link}
{kind=link}
{kind=link}
{kind=link}