


Mariana de Oliveira Trintinalha1; Gabriele Belniowski Mendes1; Fernanda Villar Fonseca2
Received on: 07/07/2019
Approved on: 02/11/2020
Financial support: None
Conflict of interest: None
Acknowledgment: We thank the reported patient, whose case brought the opportunity for study and research on a subject of great importance
Study conducted at Hospital Erasto Gaertner, Curitiba (PR), Brazil
Genital infection by Human Papillomavirus occurs 65% of the time after contact with contaminated skin and mucosa. Most people eliminate the virus through the immune system. Individual factors such as smoking, age, multiparity, prolonged use of hormonal contraceptives, sexual behavior, and infection by other Sexually Transmitted Diseases cause viral perpetuation and genital lesions, most of them asymptomatic. The most affected regions are anogenital. Treatment should be individualized. Excessive treatment can lead to scarring. We report a case of multiple treatments for removal of genital condyloma with consequent formation of extensive vulvar keloid.
Keywords: Condyloma acuminatum; Scar; Scar, Hypertrophic; Keloid
Human papillomavirus (HPV) is a very prevalent sexually transmitted disease (STD). Subtypes 6 and 11 cause genital warts and have a low potential for malignancy.1 The risk of transmission of verrucous lesions from sexual contact is 65%. After contact with the virus, most people eliminate it. However, in some individuals, there is viral perpetuation, due to factors such as smoking, age, multiparity, prolonged use of hormonal contraceptives, sexual behavior, and infection by other STDs.2 Subclinical forms and lack of knowledge about HPV manifestations increase the potential for transmission.3,4
After contact with HPV, there are three forms of infection: latent (detection of viral DNA), subclinical (microscopic change), and clinical (visible, verrucous, and often in anogenital regions). Non-macroscopic manifestation and non-knowledge of the lesions lead to potential transmitters.3,4 Diagnosis involves psychological care. The patient may feel guilty or punished, thus avoiding treatment, or performing it in an exacerbated way.2
The treatment is individualized and seeks removal of the lesion. Measures to reduce transmissibility4 should be targeted, followed by medications, surgeries, and immunotherapy.
Vulvar condylomas can be treated with trichloroacetic acid 70 to 80%, Podofylline (effect on lesions smaller than 10 cm²) or Imiquimod (antiviral and antitumor effect for limited lesions).8
Extensive and recurrent lesions are treated surgically.5 CO2 vaporization is effective for extensive lesions of the lower genital tract with a resolution of up to 71%.6 Large lesions requiring histopathology are removed by surgical excision.7 Due to the high rates of recurrence (25%), multiple treatments can be applied, being detrimental because of the potential of disorders in the cicatricial processes. Healing is the new tissue in a region of solution of continuity.
Some factors interfere and form keloid scars (reddish, irregular, pigmented, and without respect to the region’s previous margins).7 The pathophysiology of the keloid is still unclear; hyperproliferation of collagen and fibroblasts of the dermis is known to cause exacerbated scarring.8 Among the risk factors are race black/yellow, age between 10 and 30 years, female, hypertension, and excessive surgical manipulation. The sites most affected are upper abdomen, ear lobule, and sternal region. Such scars are free of dermal appendages, with a smooth and shiny appearance.8,9 We report a case of cicatricial hypertrophy after numerous treatments for excision of genital condyloma with formation of extensive vulvar keloid and physical and emotional sequelae for the carrier.
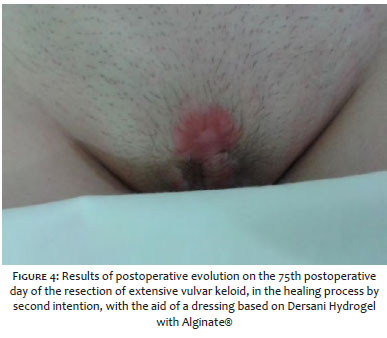
A 22-year-old white, nulligesta woman with on combined hormonal contraceptive use and male condom, without comorbidities, was admitted to a gynecological clinic with a history of extensive vulvar condylomatosis treated with chemical cauterization and thermokauterization. It evolved with itchy and painful vulvar lesion. The vulvar physical examination showed extensive fibrous plaques lesion, on the clitoris, 5 cm in diameter, extended to large lips, hardened and fixed, obliterating the clitoris (figure 1). The diagnostic hypothesis of extensive vulvar keloid was confirmed by biopsy, suggesting sequelae of multiple treatments. Prescribed high-potency corticosteroid and simple vulvectomy schedule with local infiltration of large lips with injectable triamcinolone 20mg/ml. Resected lesion under locoregional anesthesia with no possibility of surgical wound suture due to localization and extension, leaving wound healing for second intention, under hygiene care and occlusive dressing with oily lotion, as seen in figure 2. She remained two days hospitalized for analgesia and learning of care. On the 13th postoperative day: no complaints, satisfied, without pain and presenting a wound of good evolution. In the locality, good granulation of the surgical wound, without signs of infection and without formation of new keloid, decrease in the hardening of the labia majora and the obliteration of the clitoris. On the 25th postoperative day, wound with good evolution, decrease of diameter and depth of bloody area (figure 3). On the 75th postoperative day, area of young tissue under the former surgical wound and improvement of skin thickening in large lip region (figure 4), local pruritus complaint, prescribed topical corticosteroid therapy and hydration. After 105 days, a totally epithelial bloody area and a 1.5 cm scar in the region, without relief, color discreetly pinker than the original skin, improved hardening around the clitoris and large lips, good individualization of small and large lips. Patient in clinical follow-up three years ago, with no signs of recurrence of keloid or condylomas and satisfied with final treatment results.
HPV is a sexually transmitted disease whose infection occurs by accessing the virus to the epithelial basement membrane by microtraumas during sexual intercourse or virus entry into the cervix transformation zone.1
Patients diagnosed with HPV infection are emotionally fragile, presenting fear, guilt, and anger, because the social stigmas of STDs.10 This can provoke a desire for punishment by avoiding treatment or by performing it exacerbated.3 The patient, on menacing and using oral hormonal contraceptive, risk factors for viral perpetuation, underwent treatment for vulvar condylomatosis with chemical cauterization and electrocauterization and evolved with extensive vulvar lesion.3 The electrocauterization destroys the tissue by heat, among its adverse effects are the cicatricial process, loss of pilification, retractions, and local hypochromia.8 The patient evolved, biopsy confirmed keloid tissue, requiring treatments for scar excision and personal satisfaction. Gomes et al states that spontaneous regression is possible and present in up to 30% of cases within three months of observation.10 Already the excessive treatment can be cause an abnormal cicatricial process. The patient presents as risk factors to age, female gender, and excessive surgical manipulation.5,6,8 It is questioned to what extent overlapping treatments would bring more benefits than harm.3,8
HPV is present in most of the sexually active population, mostly eliminated by the immune system. Recurrence should be treated cautiously. Exaggerated manipulation of the region is a risk factor for inadequate scarring and formation of keloids. The psychological counseling necessary for many patients is emphasized.
Mariana de Oliveira Trintinalha | 0000-0002-4471-5695 Study design and planning; preparation and writing of the manuscript; data collection, analysis, and interpretation; critical literature review.
Gabriele Belniowski Mendes | 0000-0002-9787-6230 Study design and planning; preparation and writing of the manuscript; data collection, analysis, and interpretation; critical literature review.
Fernanda Villar Fonseca | 0000-0002-01629893 Approval of the final version of the manuscript; study design and planning; preparation and writing of the manuscript; active participation in research orientation; intellectual participation in propaedeutic and/or therapeutic conduct of studied cases
1. Yanofsky VR, Patel RV, Goldenberg G. Genital warts: a comprehensive review. J clin aesthet dermatol. 2012.5(6):25-36.
2. Coser J, Boeira TR, Wolf JM, Cerbaro K, Simon D, Lunge VR. Cervical human papillomavirus infection and persistence: a clinic-based study in the countryside from South Brazil. Braz J Infect Dis. 2016;20:61-68.
3. Barros SKC, Oliveira FL, Carvalho KS, Costa NJA. Condiloma acuminado: qual o reflexo desta DST em adolescentes do sexo masculino? Adolesc Saúde, 2012;9(3),72-5.
4. Naud PSV, Matos JCD, Hammes LS, Vettorazzi J. Infecção pelo papiloma vírus humano (HPV). Revista HCPA. 2000;20(2):138-42.
5. Sociedade Portuguesa de Ginecologia. Consenso sobre infecção HPV e lesões intraepiteliais do colo, vagina e vulva. [Acessed 08 de abril 2019]. Coimbra: 2011. Available from: http://www.spginecologia.pt/uploads/consenso_definitivo.pdf.
6 Federação Brasileira das Associações de Ginecologia e Obstetrícia. Manual de orientação trato genital inferior. Condiloma. 2010;10:122-8.
7. Bras F, Sardinha R, Pacheco A. Modalidades terapêuticas no tratamento dos condilomas acuminados. Acta Obstet Ginecol Port, 2015;9(5):383-92.
8. Ferreira C, D'Assumpção EA. Cicatrizes hipertróficas e quelóides. Rev Bras Cir Plást. 2006;21(1):40-48.
9. Hochman B, Locali RF, Oliveira LQR, Ferreira LM. Disfunções cicatriciais hiperproliferaticas: quelóide. Estima. 2004.4(4):33-9.
10. Gomes CM, Rades E, Zugaib M. Como devem ser tratados os condilomas genitais durante a gestação? Rev Assoc Méd Bras. 2006;52(5):286-7.
 All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773
All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773



 Read in Portuguese
Read in Portuguese
 Portuguese PDF
Portuguese PDF
 Print
Print
 Send this article by email
Send this article by email
 How to cite this article
How to cite this article
 Submit a comment
Submit a comment
 Mendeley
Mendeley
 Pocket
Pocket
{kind=link}
{kind=link}
{kind=link}
{kind=link}