


Rachel de Avila Coelho1; Juliana Cristina Silva Fraga1; Pedro Romanelli de Castro2; Marco Aurelio Lima de Sousa Figueiredo3
Received on: 14/09/2019
Approved on: 11/08/2020
Financial support: None
Conflict of interest: None
Acknowledgment: We thank the Dermatology, Urology and Pathological Anatomy staff at the Military Police Hospital
Study conducted at the Military Police Hospital of Minas Gerais, Belo Horizonte (MG), Brazil
Penile cancer is a rare tumor that has a significant impact on patients’ quality of life. In Brazil, the incidence is 5.7 cases/ 100,000 men/year, representing 2% of all types of cancer affecting men in the country and, in 2015, it culminated in 402 deaths. The traditional treatment is total penectomy with perineal urethrostomy and the consequent loss of normal sexual and urinary functions. For the preservation of penile function, organ-sparing surgery is preferred when possible, and Mohs micrographic surgery is an essential surgical alternative.
Keywords: Carcinoma, Squamous Cell; Mohs Surgery; Penile Neoplasms
Penile cancer is a rare tumor worldwide, but it has a great impact on patients’ quality of life. According to a Colombian study of systematic review and meta-analysis carried out in 2017, the incidence of penile cancer worldwide is 0.84 cases per 100,000 men/year, with the highest incidence rate found in Romania: 7.6 cases per 100,000 men/year. Brazil approaches the upper mark, with an incidence of 5.7 cases/100,000 men/year.1
According to the National Cancer Institute (INCA), the malignancy corresponds to 2% of all types of cancer that affect men in the country and that, in 2015, culminated in 402 deaths.2 The most common sites of involvement in decreasing order are: the glans, the foreskin, and the penile shaft3. Traditional treatment is partial or total amputation of the penis associated with urethral reconstruction and consequent loss of ability to maintain sexual intercourse and normal urinary functions.3
In a survey conducted by Opjordsmoen, S et al, men with penile cancer would choose the treatment with the lowest long-term survival to increase the chance of being sexually potente.4 Therefore, to preserve penile function, today organ-sparing surgery is preferred when this possibility exists.
We present a case of a 46-year-old patient with moderately differentiated squamous cell carcinoma in the glans, who opted for surgery with margin control by cutting and freezing intraoperative to preserve the male organ.
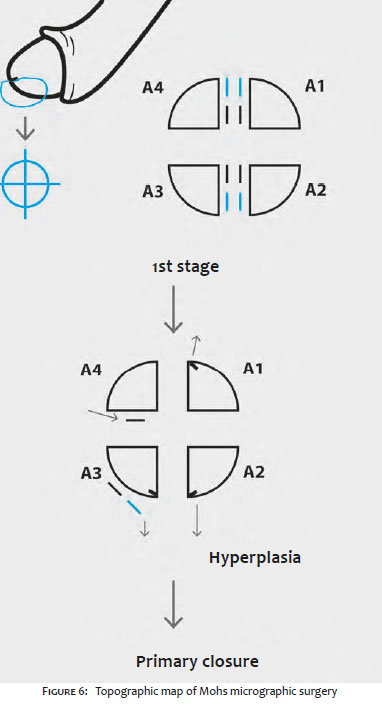
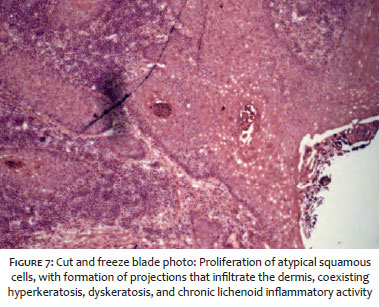
A 46-year-old male patient with phototype III attended the dermatology clinic referred by the urology team for evaluation of a hardened, ulcerated consistency plate on the glans for 1 year. He had a history of moderately differentiated invasive squamous cell carcinoma (SCC) in the glans 10 years ago, approached with partial penectomy and inguinal and pelvic emptying by laparoscopy, with one positive lymph node. He denied risky sexual behavior. After partial penectomy, the patient got married and had three children. On physical examination, he presented hypochromic stains on the penile glans and a hardened erythematous-hypochromic plaque with central ulceration on the ventral face of the glans (Figure 1). A biopsy was performed on the lesions that showed moderately differentiated SCC with an infiltrative growth pattern, with no identified angiolymphatic invasion and penile intraepithelial neoplasia. Computed tomography of the abdomen and pelvis showed no evidence of lymph node metastasis. In view of the findings of a new malignant lesion restricted to the glans, the tumor staging was T1aN0M0, with imprecise clinical limits. To preserve sexual function, Mohs Micrographic Surgery (CMM) was chosen in a joint approach with the urology team. We marked the clinical limits of the lesion (Figure 2), antisepsis, field placement and local anesthesia with Klein’s solution. Excision of the visible tumor was performed with a scalpel angled at 90º, a stage known as Debulking (Figures 3 and 4). Then, the surgical defect was enlarged by 2mm, deeply and peripherally, with resection of part of the distal urethral mucosa, configuring the 1st. CMM stage (Figure 5). In this stage, before the complete removal of the fragment, cross-sectional markings were made (Nicks), which served as a reference in the perilesional tissue for correct mapping of possible margins to be enlarged. The excised part was divided into four fragments that were placed in gauze with standardized orientation, stained and named A1, A2, A3, and A4, for making the histological slide by freezing and topographic map (Figures 5 and 6). After histopathological analysis, tumor-free margins and foci of penile intraepithelial neoplasia reaching the edges of fragments A3 and A4 (Figures 6 and 7) were found. Primary closure was performed (Figure 8) after defining the subsequent clinical treatment of the other lesions identified at the anatomical pathological examination.
Penile cancer affects mainly men in the sixth and seventh decades of life, and may also affect younger men. The mutilating potential of therapeutic surgical approaches permanently and significantly affects the quality of life of these patients. Recent studies emphasize that the histopathological characteristics of these tumors and the absence of lymph node involvement are more significant prognostic factors than the aggressiveness of surgical treatment.5 The most common histological variant is SCC, which corresponds to more than 95% of cases.3 Organ preservation can be achieved through non-surgical therapies such as external radiotherapy, brachytherapy, and topical immunomodulators. However, these are limited options in more advanced cases and have several undesirable consequences.6 All patients must be circumcised before considering conservative non-surgical treatment.3 The option for radiotherapy involves high rates of radiation, with proportionally high rates of urethral stenosis, fibrosis, and penile necrosis, and has higher failure rates than partial penectomy.7 Topical immunomodulators, such as Imiquimod 5% or 5-fluouracil, are effective for carcinomas in situ, have modest cure rates (63%), require daily application for 6-8 weeks, and can make it difficult to identify recurrent disease.8
Genital preservation surgeries aim to completely excise the primary tumor and perform local reconstruction, if necessary, to preserve the patient’s reproductive and urinary functions.9 Genital preservation surgeries are indicated for tumors in situ / Ta / T1 and some well or moderately differentiated T2 tumors and selected cases of T3 stage.10,11 The main disadvantage of these procedures is the higher local recurrence rate, which requires quarterly monitoring in the first two years, every six months from the 3rd to the 5th year, and annual until the 10th postoperative year.3
Among the surgical options, we have laser surgery, Mohs micrographic surgery, circumcision, local wide excision, “glans resurfacing”, glandectomy, partial penectomy, and total penectomy with preservation of the urethra. Mohs micrographic surgery uses intraoperative microscopic evaluation to ensure complete tumor excision with maximum preservation of normal perilesional tissue. It has excellent cure rates for SCC from other locations, but the literature shows recurrence rates of 26-32% when located on the penis.12,13,14
However, a study shows that with the strict maintenance of oncological surveillance and consequent re-approaches when necessary, the overall survival rates are excellent and the rates of progression are low.15 The same study considers that Mohs micrographic surgery should not be limited to the approach of low-grade, small, and superficial tumors as was suggested in the older literature, but that it should be used as a treatment strategy for tumors with urethral involvement, saving patients from total or partial penectomies.15 The recurrence rate found in this study was 11.1% and the re-approach of these patients with new Mohs micrographic surgery showed a final cure rate of 100%, both in cases of SCC in situ (mean follow-up of 72.5 months) and invasive SCC (mean follow-up of 77 months). In view of the great psychosocial impact of aggressive penile cancer treatment and the possibility of management with preservation of sexual and urinary functions associated with good overall survival rates, we believe that the best approach is one that allows the maintenance of quality of life despite the need for more frequent and prolonged follow-ups.
Rachel de Avila Coelho | 0000-0002-7947-7754
Author’s contribution: Approval of the final version of the manuscript; study design and planning; preparation and writing of the manuscript; data collection, analysis, and interpretation; intellectual participation in propaedeutic and/or therapeutic conduct of studied cases; critical literature review; critical revision of the manuscript.
Juliana Cristina Silva Fraga | 0000-0002-1593-8742
Author’s contribution: Approval of the final version of the manuscript; preparation and writing of the manuscript; active participation in research orientation; intellectual participation in propaedeutic and/or therapeutic conduct of studied cases.
Pedro Romanelli de Castro | 0000-0003-3717-9748
Author’s contribution: Active participation in research orientation; intellectual participation in propaedeutic and/or therapeutic conduct of studied cases.
Marco Aurelio Lima de Sousa Figueiredo | 0000-0002-1037-1433
Author’s contribution: Intellectual participation in propaedeutic and/or therapeutic conduct of studied cases.
1. Montes Cardona CE, García-Perdomo HA. Incidence of penile cancer worldwide: systematic review and meta-analysis. Rev Panam Salud Publica. 2017;41:e117.
2. Instituto Nacional do Câncer [homepage]. Câncer de Pênis [acessed 20 de outubro de 2019]. Available from: https://www.inca.gov.br/tipos-de-cancer/cancer-de-penis.
3. Hakenberg OW, Comperat EM, Minhas, S. EAU guidelines on penile cancer: 2014 update. Eur Urol. 2015;67(1):142-50.
4. Opjordsmoen S, Fossa, SD. Quality of life in patients treated for penile cancer. A follow-up study. Br J Urol. 1994;74(5):652-7.
5. Ficarra V, Akduman B, Bouchot, O. Prognostic factors in penile cancer. Urology 2010;76(2 Suppl 1):S66-73.
6. Kamel MH, Bissada N, Warford R, Farias J, Davis R. Organ Sparing Surgery in Penile Cancer: a Systematic Review, J Urol. 2017;198(4):770-9.
7. Zouhair A, Coucke PA, Jeanneret W. Radiation therapy alone or combined surgery and radiation therapy in squamous-cell carcinoma of the penis? Eur J Cancer 2001;37(2):198-203.
8. Deen K, Burdon-Jones D. Imiquimod in the treatment of penile intraepithelial neoplasia: an update. Australas J Dermatol, 2017;58(2):86-92.
9. Philippou, P., Shabbir, M., Malone, P. Conservative surgery for squamous cell carcinoma of the penis: resection margins and long-term oncological control. J Urol 2012;188(3):803-8.
10. Pompeo AC, Zequi Sde C, Pompeo AS. Penile cancer: organ-sparing surgery. Curr Opin Urol 2015;25(2):121-8.
11. Horenblas S, van Tinteren H, Delemarre JF. Squamous cell carcinoma of the penis. II. Treatment of the primary tumor. J Urol 1992;147(6):1533-8.
12. Brown MD, Zachary CB, Grekin RC, Swanson NA. Penile tumors: their management by Mohs micrographic surgery. J Dermatol Surg Oncol. 1987;13(11):1163-7.
13. Mohs FE, Snow SN, Larson PO. Mohs micrographic surgery for penile tumors. Urol Clin North Am 1992;19(2):291-304.
14. Shindel AW, Mann MW, Lev RY, Sengelmann R. Mohs micrographic surgery for penile cancer: management and long-term followup. J Urol 2007;178(5):1980-5.
15. Machan M, Brodland D, Zitelli J. Penile Squamous Cell Carcinoma: Penis-Preserving Treatment With Mohs Micrographic Surgery. Dermatol Surg 2016;42(8):936-44.
 All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773
All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773



 Read in Portuguese
Read in Portuguese
 Portuguese PDF
Portuguese PDF
 Print
Print
 Send this article by email
Send this article by email
 How to cite this article
How to cite this article
 Submit a comment
Submit a comment
 Mendeley
Mendeley
 Pocket
Pocket
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}