


Luciane Prado Silva Tavares1,2; Yasmin Pugliesi2; Lucas Barros Terra Cunha3; Daniel Martins Hiramatsu4
Received on: 30/08/2019
Approved on: 25/02/2020
Financial support: None
Conflict of interest: None
Study conducted at the Hospital Geral Público de Palmas, Palmas (TO), Brazil
The giant BCC is a rare variant, and the repair of large defects in the scalp, generated after oncologic resection, is a surgical challenge. We report the case of a patient submitted to late scalp reconstruction after oncologic resection of giant BCC in the scalp with the association of techniques. Reconstruction of scalp lesions depends on a comprehensive understanding of the anatomy of this site, knowledge of the arsenal of surgical techniques, and a detailed assessment of patient factors and expectations, given the impact on the quality of life and morbidity related to each therapeutic option.
Keywords: Carcinoma, Basal Cell; Reconstructive Surgical Procedures; Scalp Dermatoses
Basal cell carcinoma (BCC) is the most common cancer in light-skinned populations, accounting for more than 75% of non-melanoma skin cancers. It occurs in the head and neck region in approximately 80% of cases. Giant BCC (GBCC), defined as a lesion larger than 5 cm in its largest diameter, is a rare variant of BCC, with an incidence of 0.5%.1-3 In contrast to the small lesion, the giant variant develops on non-exposed skin, including the back, shoulders, groins, and thighs. Scalp involvement is extremely rare. The lesion can invade the underlying deep tissue, compromising treatment options and challenging reconstruction methods.
Many therapeutic modalities have already been reported as surgical options, with varying results. The main ones include surgical excision and reconstruction, radiotherapy, and Mohs micrographic surgery, the latter being the gold standard treatment for giant BCC.1,2
Scalp reconstruction after ablative surgery can be challenging. Physicians must evaluate each case individually. The best proposal for reconstruction must be based on the patient’s health, psychosocial aspect, and the therapeutic planning of the underlying disease, without compromising the oncological surgery principles.4,5
This study aims to report the case of a patient who underwent late scalp reconstruction after oncological resection of giant basal cell carcinoma on the scalp, with the association of techniques.
A 74-year-old woman, retired, living in a rural area, presented a papular-nodular lesion on the scalp eight years ago. The lesion had slow and progressive growth, with central healing, bleeding, and local itching.
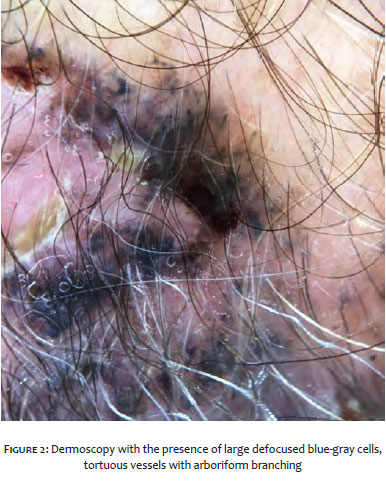
Upon dermatological examination, we observed a scalp with an extensive plaque of scarring alopecia, presenting an atrophic center, with exulcerations and crusts, periphery with papulous, pigmented, lacy-looking edges, measuring 17 x 17 cm, located in the right frontotemporoparietal region. (Figure 1). Dermoscopy showed the presence of large, unfocused blue-gray cells, with edges tending to form rounded structures and tortuous vessels with arboriform ramifications (Figure 2). Anatomopathology was compatible with pigmented basal cell carcinoma.
We performed a scalp lesion excision, respecting oncological surgical margins, aided by dermoscopy. Healing by secondary intention was chosen with late reapproach (Figures 3 e 4).
After four months, partial skin grafting of the lateral aspect of the left thigh was performed on the recipient area’s granulation tissue, using a dermatome.
The patient evolved with good response to the graft, presenting necrosis of approximately 10% of its extension and subsequent total healing (Figure 5).
The repair of large scalp defects generated after cancer resection is a surgical challenge. Modern surgery techniques have provided a greater capacity for resolving lesions and as a reduction in perioperative and postoperative complications, and a better aesthetic and functional result.6
Size, location, local tissue’s quality, and scalp distortion help choose the best reconstructive method. Practitioners must also consider the patient’s intrinsic and psychosocial factors, given the impact on their quality of life.4,6
Healing by secondary intention can be used when the pericranial layer with extensive exposure is present, and when a shorter surgical time is required. The disadvantages of this method include delayed healing, alopecia, telangiectasias, and thin coverage.4
The partial skin graft has been used in large defects due to the technique’s speed and ease, the possibility of monitoring tumor recurrence, and fast healing.7 It should be used when aesthetic issues are not a concern, as they can lead to alopecia, hypopigmentation, contour deformity, and morbidity of the donor site.4
A retrospective study assessed 65 patients who underwent skin grafts on the scalp, with grafts from various sites, including six thigh flaps. This study reported a low rate of surgery complications and satisfactory and long-lasting cosmetic results. It recommended using anterolateral thigh (ALT) flaps for surgeries in the scalp’s temporal-lateral region.8
As in the case reported, the association of healing by secondary intention techniques and partial skin graft can be used. The formation of granulation tissue is related to greater adherence of the skin graft due to greater vascularization, enabling better results.4
The reconstruction of scalp lesions depends on a comprehensive understanding of the scalp’s anatomy, knowledge of the surgical techniques’ arsenal, and a detailed assessment of the patient’s factors and expectations. The reconstructive goal must be adapted for each patient individually, aiming at the success of the reconstruction and a satisfactory aesthetic-functional result.
Luciane Prado Silva Tavares | 0000-0002-2410-3843
Approval of the final version of the manuscript; active participation in research orientation; intellectual participation in propaedeutic and/or therapeutic conduct of studied cases; critical revision of the manuscript.
Yasmin Pugliesi | 0000-0003-0630-4980
Statistical analysis; study design and planning; preparation and writing of the manuscript; data collection, analysis, and interpretation critical literature review.
Lucas Barros Terra Cunha | 0000-0002-0710-3219
Statistical analysis; study design and planning; preparation and writing of the manuscript; data collection, analysis, and interpretation; critical literature review.
Daniel Martins Hiramatsu | 0000-0001-5983-5801
Approval of the final version of the manuscript; active participation in research orientation; intellectual participation in propaedeutic and/or therapeutic conduct of studied cases; critical revision of the manuscript.
1. Heo YS. Yoon JH, Choi JE, Ahn HH, Kye YC, Seo SH. A case of superficial giant basal cell carcinoma with satellite lesions on scalp. Ann. Dermatol. 2011;23(Suppl 1):S111-5.
2. Larsen AK, Ghulam El-Charnoubi WA, Gehl J, Krag C. Neglected giant scalp basal cell carcinoma. Plast Reconstr Surg. Glob Open. 2014;2(3):e120.
3. Chatterjee S, Mott JH, Dickson S, Kelly CG. Extensive basal cell carcinoma of the forehead and anterior scalp: use of helical tomotherapy as a radiotherapy treatment modality. Br. J. Radiol. 2010;83(990):538-40.
4. Desai SC, Sand JP, Sharon JD, Branham G, Nussenbaum B. Scalp reconstruction an algorithmic approach and systematic review. JAMA Facial Plast Surg. 2015;17(1):56-66.
5. Ebrahimi A, Nejadsarvari N, Ebrahimi A. Reconstructions of small scalp defects with step flap. J Cutan Aesthet Surg. 2017;10(2):106-8.
6. Souza CD. Reconstrução de grandes defeitos de couro cabeludo e fronte em oncologia: tática pessoal e experiência - análise de 25 casos. Rev Bras Cir Plást. 2012;27(2):227-37.
7. Anbar RA, Almeida KG, Nukariya PY, Anbar RA, Coutinho BBA. Métodos de reconstrução do couro cabeludo. Rev Bras Cir Plást. 2012;27(1):156-9.
8. O'Connell DA, Teng MS, Mendez E, Futran, N. D. Microvascular free tissue transfer in the reconstruction of scalp and lateral temporal bone defects. Craniomaxillofac Trauma Reconstr. 2011;4(4):179-88.
 All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773
All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773



 Read in Portuguese
Read in Portuguese
 Portuguese PDF
Portuguese PDF
 Print
Print
 Send this article by email
Send this article by email
 How to cite this article
How to cite this article
 Submit a comment
Submit a comment
 Mendeley
Mendeley
 Pocket
Pocket
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}