


Laura Costa Beber de Jesus1; Gabriela Machado Dias Junqueira1; Getullio Pisa Carneiro1; Douglas Haddad Filho2
Received on: 30/04/2018
Approved on: 11/08/2020
Financial support: None
Conflict of interest: None
Acknowledgement: We thank our family members and tutors, who always encourage us to improve our knowledge in an attempt to offer the best to our patients
Study conducted at the University of Santo Amaro, São Paulo (SP), Brazil
Cysts are benign epithelial tumors widespread. The trichilemmal cysts, originating from the anagen’s isthmus, represent about 20% of the cysts and are located more frequently in the scalp (90%). Several methods can be used for the removal of the cysts. The choice of technique depends on its characteristics, such as size, mobility, consistency, quiescence, inflammation, and quantity. However, they may grow again if the capsule is incomplete removed. The authors present a simple variant of the marsupialization technique that allows its complete removal.
Keywords: Ambulatory Surgical Procedures; Cysts; Scalp Dermatoses
Cysts are widespread benign epithelial tumors. They consist of a space lined by an epithelium filled with liquid or pasty content, mobile concerning the deep planes, located in the dermis or subcutaneous.1,2 They are usually asymptomatic and are located mainly in the cephalic segment, neck, and upper trunk.¹
Epidermoid or follicular cysts are more common in adults and can originate from the hair infundibulum or follicular ostium (comedone). The pillar or trichilemmal cyst derives from the isthmus of the anagen hair and the steatocystoma, from the sebaceous glands, therefore being true sebaceous.3
Trichilemmal cysts are less common than epidermoid cysts, representing about 20% of cysts. They have a preference for women, middle-aged adults, or older than 60 years. They are more frequent on the scalp (90%) and rare on the face, limbs, and trunk.4,5 Unlike the epidermoid cyst, they have no orifice. They present a firmer consistency and are more mobile than the epidermoid cyst.3
Several methods can successfully remove the cysts. The choice depends on the cyst’s size, the quality of the overlying skin, the existence or not of the exit hole of the cyst, among other variables. However, they can relapse if there is incomplete removal of the capsule.6
We present a surgical marsupialization technique that allows safety in the total removal of the capsule, a technical variation not described in the literature.
A cyst (about 1.5 cm in its largest diameter) in the scalp’s midline, of elastic consistency, painless on palpation, not adhered to deep planes (Figure 1).
1. Marking of the incision on the line with the largest diameter of the cyst and its limits (Figure 1)
2. Local asepsis and antisepsis
3. Local anesthesia (lidocaine with vasoconstrictor),
2ml, in the incision, in the plane between the dermis and the anterior wall of the cyst (Figure 2)
4. Skin incision with a surgical scalpel blade n. 15 (Figure 3)
5. Incision in the cyst capsule with a surgical scalpel blade n. 15
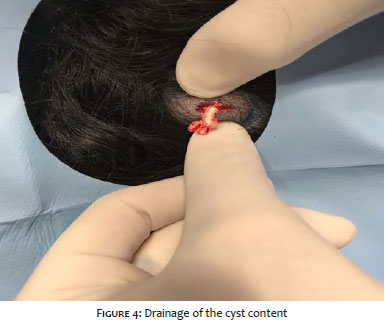
6. Drainage of cyst content (Figure 4)
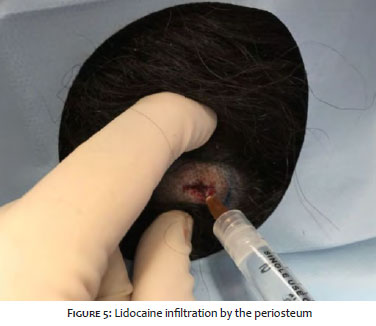
7. Deep anesthetic infiltration (1 ml) in the plane between the posterior wall of the cyst and the periosteum (Figura 5)
8. Expression of the cyst towards the skull (Figure 6)
9. Removal of the cyst using a Halsted clamp (Figure 7)
10. Suture
Epidermoid or follicular cysts can have a central orifice and are often found in the dermis, hypodermis, and subcutaneous tissue. Although they are a very common and easily resolved clinical entity, they still depend on surgical management.3
The need for resections of the skin segment above the cyst depends a lot on the skin’s quality since the cyst may have suffered inflammation and/or infections. Another fact requiring skin removal is the presence of the orifice that identifies the follicular ostium from which the cyst derives, which also must be removed.
Conventional removal is performed with infiltration anesthesia around and superficially to the anterior cyst wall, and it is one of the most used techniques in treating follicular cysts.4 It is performed through an incision on the skin surface, exposing the underlying cyst. The Halsted clamp is used to facilitate the detachment of the cyst's lateral and deep walls with delicately curved iris scissors until the total removal of the structure.1,6,7
Although this technique is highly efficient, the possibility of rupture of the cyst in the tissues’ dissection increases the probability of the permanence of capsule residues, potentiating a recurrence.
The technique presented performs the infiltration in the cyst's posterior region, which, with a two_en-finger compression maneuver, everts the cyst towards the incision when it is pulled. The inflammatory and infectious cyst recurrence processes can lead to the formation of a perilesional granuloma and reactive fibrosis, making it difficult to remove the capsule. In such cases, the presented technique’s applicability may not be indicated since the existing fibrosis in the region would hinder the cyst’s complete removal. Thus, removing the block structure, that is, skin and cyst, is recommended, which, although increasing the procedure’s volume, guarantees the complete removal of the capsule.
The advantage of the presented technique lies in the fact that it is not necessary to separate the cyst's tissue and neighboring tissues, which, in turn, decreases bleeding and, consequently, the surgical time. This technique is simple, quick and applicable to places like the rigid scalp surface.3
Laura Costa Beber de Jesus | 0000-0003-2347-5554
Study design and planning; preparation and writing of the manuscript; critical literature review.
Gabriela Machado Dias Junqueira | 0000-0003-0899-9341
Preparation and writing of the manuscript; critical literature review.
Getullio Pisa Carneiro | 0000-0001-7748-0282
Approval of the final version of the manuscript; critical revision of the manuscript.
Douglas Haddad Filho | 0000-0001-9304-4739
Approval of the final version of the manuscript; study design and planning; preparation and writing of the manuscript; active participation in research orientation; intellectual participation in propaedeutic and/or therapeutic conduct of studied cases.
1. Junior WB, Chiacchio ND, Criado PR. Tratado de dermatologia. 2nd ed. São Paulo: Atheneu, 2014. p. 2332.
2. Sampaio SAP, Rivitti EA. Dermatologia. 3th ed. São Paulo: Artes Médicas, 2007. p. 1120-1121.
3. Galdelha ADR, Costa IMC. Cirurgia Dermatológica. 3th ed. São Paulo : Atheneu, 2017. p. 761-762.
4. Al-Khateeb TH, Al-Masri NM, Al-Zoubi F. Cutaneous cysts of the head and neck. J Oral Maxillofac surg. 2009;67(1):52-7.
5. Fitzpatrick TB. Fitzpatrick's color atlas and synopsis of clinical dermatology. 5th ed. New York: McGraw-Hill, 2005. p. 171.
6. Mehrabi D, Leonhardt JM, Brodell RT. Removal of keratinous and pilar cysts with the punch incision technique: analysis of surgical outcomes. Dermatol Surg. 2002;28(8):673-7.
7. Lopes Filho LL, Lopes LRS. Cistos (Epidérmico, Pilar, Mixoide, Dermoide), Dermatofibroma e Lipoma. In: Palermo E. [et al.] editors. Tratado de cirurgia dermatológica, cosmiatria e laser da Sociedade Brasileira de Dermatologia. 1st ed. Rio de Janeiro: Elsevier, 2013. p. 621-627.
 All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773
All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773



 Read in Portuguese
Read in Portuguese
 Portuguese PDF
Portuguese PDF
 Print
Print
 Send this article by email
Send this article by email
 How to cite this article
How to cite this article
 Submit a comment
Submit a comment
 Mendeley
Mendeley
 Pocket
Pocket
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}