


Luciana Pereira Paes Gomes Saraiva1; Renata do Val Guimarães1; Guillermo Loda1,2; Marcela Benez1
Received on: 08/10/2018
Approved on: 26/02/2020
Financial support: None
Conflict of interest: None
Study conducted at Dermatological Surgery Service of the Rubem David Azulay Institute, Santa Casa de Misericórdia do Rio de Janeiro, Rio de Janeiro (RJ), Brazil
The nasal region is often affected by cutaneous neoplasm, especially in individuals of low phototypes, where the incidence of basal cell carcinoma is high. Surgical defects in the nasal wing and perinasal region constitute a challenge to its reconstruction since it involves several cosmetic units and preservation of the nasal groove. The preservation of the limits between these units is thus fundamental for good functional and aesthetic results. This article aims to show the application of the Shark Island Flap for the correction of defects in the nasal and perinasal regions.
Keywords: Nasal Surgical Procedures; Neoplasms, Basal Cell; Nose Neoplasms
Skin neoplasms frequently affected the nasal region, especially in individuals with low skin phototypes, in whom the incidence of basal cell carcinoma is high.
According to a study conducted at the Brazilian National Cancer Institute (INCA), basal cell carcinoma was responsible for nasal defects in which partial or subtotal nose reconstructions were performed. Moreover, squamous cell carcinoma was the main responsible in cases of total nasal reconstruction.
Non-melanoma skin cancer is the most frequent among Brazilian men and the second among women. Approximately 93% of basal cell carcinomas occur in the head and neck and, of these, 25% appear in the nasal pyramid. Thus, it is undoubtedly the most common cancer of the head and neck.1
The nose region has unique characteristics that surgeons should consider when planning the surgical reconstruction of the defect. The complex topography, with concave and convex surfaces, needs to be preserved. The nasal wing’s free margin can be easily raised and distorted if the reconstruction is not carefully planned. The lower third of the nose’s skin has reduced mobility and is not easily recruited for primary wound closure without causing anatomical distortions. It is also a region with a unique texture and coloring characteristics, not resembling the surrounding skin. Finally, the nose’s functional aspect must always be considered, preserving the bone, cartilage, and mucosa structure, never compromising the airway.2
The lateral nasal wing, lateral side of the nose, malar region, and supralabial skin delimit the nasal and perinasal region.3
Surgical defects involving this region are challenging at the time of its reconstruction. This is because the combination of these defects involves several cosmetic units of the face, and transgressing from one unit to another, at the time of reconstruction, can lead to the erasure of the nasal sulcus and the loss of the limits of these units, causing an unsatisfactory aesthetic result.4
Options for managing deep defects in the nasal wing and perinasal region include primary closure, healing by secondary intention, local flaps, interpolation flaps, and skin grafts.
Performing a flap using skin adjacent to the surgical defect is ideal for obtaining a good functional and cosmetic result. In this case, the subcutaneous shark island pedicle flap proved to be effective, as it is a procedure performed in a single surgical procedure, under local anesthesia, with skin that preserves the same characteristics of texture, color, and concentration of sebaceous glands in the dry area, besides preserving the nasal sulcus and maintaining the limits between the cosmetic units of the face.
A 58-year-old man presented nodular, erythematous-pigmented lesion, with telangiectasias, of about 5 mm x 6 mm, with pearly edges, in the nasal sulcus and right perinasal region, suggestive of basal cell carcinoma (Figure 1).
Due to the surgical lesion location (Figure 2), the subcutaneous shark island pedicle flap proved to be one of the options to be considered.
The pedicle flap’s demarcation was performed so that the upper arm rotated 90 degrees concerning the surgical defect as if the “shark’s fin” fits the alar edge of the nose (Figure 3).
Subsequently, the tissue was rotated, causing the rest of the flap to form an inverted cone of skin redundancy (Figure 4), resulting in the natural creation of the nasal wing and sulcus, without the need for anchoring the flap.
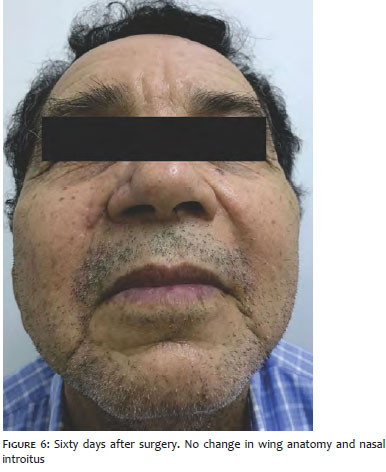
Finally, the flap’s lower arm was sutured, positioning the scar along the nasolabial fold, which provided a satisfactory immediate postoperative result without altering the anatomy of the wing and nasal introitus (Figures 5 e 6).
The nasal surgical reconstruction options must contemplate the region’s functional and aesthetic preservation, always trying to use techniques that camouflage the scars in the face’s folds and natural lines.5
A surgical option in this region is healing by second intention and primary closure, quick and straightforward solutions for small defects. However, in more extensive cases, such as the one described, they can retract the nasal wing and functional impairment when modifying the nasal introitus’s anatomy.
On the other hand, the skin graft is a good option for large defects, especially in areas where there is no tissue distensibility and in cases where it is not possible to delimit the intraoperative tumor area. However, professionals should avoid its use whenever possible, as it does not give a satisfactory aesthetic aspect. It may occur because it is a technique that does not always use skin with similar characteristics to the area to be reconstructed regarding color, texture, thickness, and concentration of sebaceous glands, which can lead to local hypopigmentation.
Bilobed transposition flaps would not be a good option because they are more indicated in defects more centralized in the nasal dorsum or the nose’s lateral wall. Besides, they also have a chance of skin redundancy with a trapdoor effect.
An option that could be used in this surgical wound is the pedicle advancement skin flap or island pedicle flap. It preserves the anatomy of this concave region of the face and presents a pattern of myocutaneous vascularization, which gives the flap great viability.
In our case, we chose the shark island pedicle flap, which receives this name because it resembles the shape of a shark, with the “fin” and ventral mouth formed from the surgical defect.
The advancement of the flap with the rotation movement of the “shark’s fin” region, spontaneously, creates an inverted cone of skin redundancy, which redefines the groove of the nasal wing, and the perinasal tissues restore the contour of the nasal wing region, maintaining a well-defined boundary between the cosmetic units of the malar and nasal regions.6
Therefore, the shark island pedicle flap is a surgical reconstruction technique for defects in the nasal and perinasal region, reproducible, performed in a single operative time, and offers a very satisfactory functional and cosmetic result without distorting the anatomy and of the area.
Luciana Pereira Paes Gomes Saraiva | 0000-0003-1138-6255
Preparation and writing of the manuscript; data collection, analysis, and interpretation; critical literature review; critical revision of the manuscript.
Renata do Val Guimarães | 0000-0003-1070-1778
Data collection, analysis, and interpretation; critical literature review; critical revision of the manuscript.
Guillermo Loda | 0000-0003-0511-0025
Study design and planning; active participation in research orientation; critical revision of the manuscript; approval of the final version of the manuscript.
Marcela Benez | 0000-0003-0289-5656
Active participation in research orientation; critical revision of the manuscript; approval of the final version of the manuscript.
1. Souza Filho MVP, Kobig RN, Barros PB, Dibe MJA, Leal PRA. Reconstrução nasal: análise de 253 casos realizados no Instituto Nacional do Câncer. Rev. Bras. Cancerol. 2012;48(2):239-45.
2. Zitelli JA. The bilobed flap for nasal reconstruction. Arch Dermatol. 1989;125(7):957-9.
3. Asgari M, Odland P. Nasalis island pedicle flap in nasal ala reconstruction. Dermatol Surg. 2005;31(4):448-52.
4. Cvancara J, Wentzell JM. Shark island pedicle flap for repair of combined nasal ala-perialardefects. Dermatol Surg. 2006;32(5):726-9.
5. Levasseur JG, Mellette JR Jr. Techniques for reconstruction of perialar and perialar nasal ala combined defects. Dermatol Surg. 2000;26(11):1019-23.
6. André MC, Fraga A, Garcia CR, Pignatelli JG, Soares RO. Retalho em ilha de tubarão: uma técnica cirúrgica reconstrutiva de defeitos localizados na área nasal alar/perialar. Um procedimento simples. An Bras Dermatol. 2011;86(4suppl.1):160-3.
 All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773
All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773



 Read in Portuguese
Read in Portuguese
 Portuguese PDF
Portuguese PDF
 Print
Print
 Send this article by email
Send this article by email
 How to cite this article
How to cite this article
 Submit a comment
Submit a comment
 Mendeley
Mendeley
 Pocket
Pocket
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}