


Ana Beatriz Antunes Funes; Ana Carolina Gama Martins; André Matheus Camelo Neves; Marilda Aparecida Milanez Morgado de Abreu; Ana Cláudia Cavalcante Espósito
Receipt date: 12/03/2020
Approval date: 18/08/2020
Financial Support: None
Conflict of Interest: None
Study conducted at the Universidade do Oeste Paulista, Presidente Prudente (SP), Brazil.
INTRODUCTION: Dermatobia hominis is one of the main etiologic agents of furunculoid myiasis. It is more common in intertropical countries and induces the formation of a papule or nodule in the skin with a central orifice. When the lesion's diagnosis is not made or when the larva does not go out, it can progress to the formation of a tumor. We report a rare case of a lipoma-simulating lesion in the lower limb of a man living in the countryside. The etiological diagnosis was made exclusively through histopathological examination, which showed a cyst with exogenous material to the center, compatible with D. hominis, in a clear degradation process.
Keywords: Larva; Lipoma; Myiasis
Dermatobia hominis, of the family Cuterebridae, is the most common etiologic agent of furunculoid cutaneous myiasis.1 Its life cycle has a particular characteristic, called foresia, in which the female lays its eggs in the abdomen of a blood-sucking insect, establishing an interspecific harmonic relationship.2 More than 50 species can carry the eggs, especially Sarcopromusca pruna, Musca domestica, and Haematobia irritans.3 When the insect bites an individual, the eggs come into contact with the human skin’s heat, hatching. Then, the larva penetrates the skin, even if it is intact.1 The larva remains inside the formed papule or nodule for five to ten weeks, and during this period, it passes through the first, second, and third larval stages. In the complete cycle, the mature larva emerges on the skin’s surface during the night, falls to the ground, and forms the pupa. One month after leaving the host, the adult insect hatches, keeping the cycle.1
When the larva is placed on human skin, extraction is often done before the cycle is complete. However, in rare cases, the larvae encyst in the subcutaneous tissue and may progress to nodules’ formation. In the present article, we report the case of a patient with a subcutaneous tumor in the lower limb, with a long evolution, whose clinical characteristics simulated a lipoma. However, ultrasonography was compatible with a foreign body, and, after excision of the lesion, histopathological examination allowed the visualization of the larva.
A 56-year-old man, farmer, residing in the countryside, sought medical assistance due to the appearance, two years ago, of an asymptomatic lesion on the medial aspect of his left leg. The patient denied trauma preceding the development.
He presented a subcutaneous tumor of 4 cm in diameter on physical examination, with softened consistency, not adhered to the deep planes, painless on palpation, and without a central hole. The skin overlying the lesion did not show signs of inflammation (Figure 1). The clinical hypothesis was of lipoma. However, as the patient presented varicose veins in the lower limbs, we requested ultrasonography with Doppler Color for surgical planning. The imaging showed a fusiform hypoechoic capsule located in the subcutaneous tissue, and, in the center, there was a 17x6 mm hyperechoic image, which could be compatible with a foreign body.
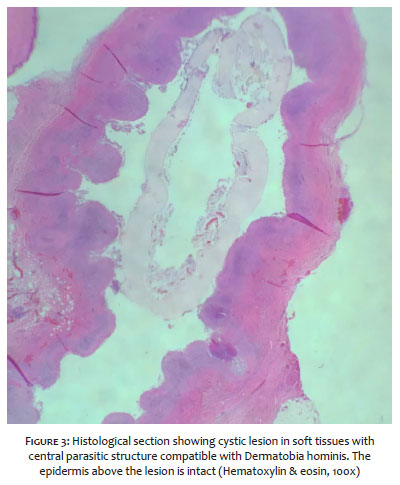
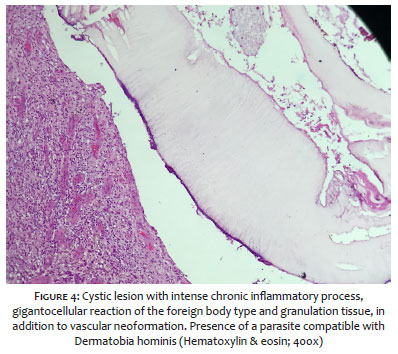
The complete excision of the lesion was performed according to previous demarcation (Figure 2). Upon histopathological examination of the material, we macroscopically observed a nodular formation measuring 1.8 cm, with a single cavity filled with a yellowish liquid. There was an intense chronic inflammatory process, with gigantocellular reaction of the foreign body type and granulation tissue with vascular neoformation and collagen degradation. In the center, there was an exogenous material compatible with D. hominis in a clear degradation process (Figures 3 and 4).
The patient evolved with adequate wound healing (Figure 5) and underwent routine dermatological follow-up for two years.
The main agents of furunculoid cutaneous myiasis are Dermatobia hominis, Cordylobia anthropophaga, Cuterebra sp, and Wohlfahrtia sp.4,5 It is more common in developing (intertropical) countries, such as those in Central America, South America, and sub-Saharan Africa.6 The incident cases in individuals coming from other areas of the globe result, in general, from travelers who were in an endemic area, implying a significant diagnostic challenge when returning to their country of origin.7,8
Dermatobia hominis has rows of dark backward spines, a pair of hooks in the mouth, striated muscles, as well as an external cuticle that involves the internal organs.9 Larva infestation is related to poor hygiene habits, living in the countryside (as in the case reported), and low socioeconomic status.8
D. hominis' presence in the skin induces a papule or a nodule formation, with a central orifice of approximately 1 mm (corresponding to the invertebrate's respiratory pore and visualized by dermoscopy), from which a serosanguinous or purulent secretion leaks.7,8
In general, manual extraction of the larva is not a challenge, and the occlusion of the orifice with petroleum substances facilitates the process.5 However, when the diagnosis of the lesion is not performed correctly or when the larva is not broken (spontaneously or under manipulation), it can evolve to the formation of a tumor that simulates an epidermal cyst, lipoma (as the case presented), or even soft tissue malignancies.10,11 In these cases, the only effective procedure is surgical excision.
We report the case of a patient with furunculoid cutaneous myiasis, in which the larva was not expelled, evolving to form a large cystic lesion simulating a lipoma. This lesion persisted for two years, a period much longer than the usual. In endemic countries, especially in rural dwellers or under strict hygiene conditions, the possibility of larvae infestation should be considered.
Ana Beatriz Antunes Funes | 0000-0002-1224-8535
Approval of the final version of the manuscript; study design and planning; preparation and writing of the manuscript; critical literature review; critical revision of the manuscript.
Ana Carolina Gama Martins | 0000-0002-8507-0774
Approval of the final version of the manuscript; study design and planning; preparation and writing of the manuscript; critical literature review; critical revision of the manuscript.
André Matheus Camelo Neves | 0000-0001-8602-5724
Approval of the final version of the manuscript; study design and planning; preparation and writing of the manuscript; data collection, analysis, and interpretation; critical literature review; critical revision of the manuscript.
Marilda Aparecida Milanez Morgado de Abreu | 0000-0001-9099-6013
Approval of the final version of the manuscript; preparation and writing of the manuscript; data collection, analysis, and interpretation; active participation in research orientation; intellectual participation in propaedeutic and/or therapeutic conduct of studied cases; critical literature review; critical revision of the manuscript.
Ana Cláudia Cavalcante Espósito | 0000-0001-9283-2354
Approval of the final version of the manuscript; study design and planning; preparation and writing of the manuscript; data collection, analysis, and interpretation; active participation in research orientation; intellectual participation in propaedeutic and/or therapeutic conduct of studied cases; critical literature review; critical revision of the manuscript.
1. Villalobos G, Vega-Memije ME, Maravilla P, Martinez-Hernandez F. Myiasis caused by Dermatobia hominis: countries with increased risk for travelers going to neotropic areas. Int J Dermatol. 2016;55(10):1060-8.
2. Safdar N, Young DK, Andes D. Autochthonous furuncular myiasis in the United States: case report and literature review. Clin Infect Dis. 2003;36(7):e73-80.
3. Azevedo RR, Duarte JLP, Ribeiro PB, Krüger RF. Occurrence of Sarcopromusca pruna (Diptera) in Southern Brazil as a vector of Dermatobia hominis (Diptera) eggs. Arq Bras Med Vet Zootec. 2007;59(5):1348-50.
4. Ko JY, Lee I-Y, Park BJ, Shin JM, Ryu J-S. A case of cutaneous myiasis caused by Cordylobia anthropophaga larvae in a Korean traveler returning from Central Africa. Korean J Parasitol. 2018;56(2):199-203.
5. Suárez JA, Ying A, Orillac LA, Cedeño I, Sosa N. First case of furuncular myiasis due to Cordylobia anthropophaga in a Latin American resident returning from Central African Republic. Braz J Infect Dis. 2018;22(1):70-3.
6. Rodriguez-Cerdeira C, Gregorio MC, Guzman RA. Dermatobia Hominis infestation misdiagnosed as abscesses in a traveler to Spain. Acta dermatovenereol Croat. 2018;26(3):267-9.
7. Olsen J, Nejsum P, Jemec GBE. Dermatobia hominis misdiagnosed as abscesses in a traveler returning from Brazil to Denmark. Acta Dermatovenerol Alp Pannonica Adriat. 2017;26(2):43-4.
8. Dunphy L, Sood V. Dermatobia hominis "the human botfly" presenting as a scalp lesion. BMJ Case Rep. 2019;12(3).
9. Harbin LJ, Khan M, Thompson EM, Goldin RD. A sebaceous cyst with a difference: Dermatobia hominis. J Clin Pathol. 2002;55(10):798-9.
10. Schembre DB, Spillert CR, Khan MY, Lazaro EJ. Dermatobia hominis myiasis masquerading as an infected sebaceous cyst. Can J Surg. 1990;33(2):145-6.
11. Kahn DG. Myiasis secondary to Sermatobia hominis (human botfly) presenting as a long-standing breast mass. Arch Pathol Lab Med. 1999;123(9):829-31.
 All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773
All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773



 Read in Portuguese
Read in Portuguese
 Portuguese PDF
Portuguese PDF
 Print
Print
 Send this article by email
Send this article by email
 How to cite this article
How to cite this article
 Submit a comment
Submit a comment
 Mendeley
Mendeley
 Pocket
Pocket
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}