


Manoella Freitas Santos1,2; Maria Emilia Vieira de Souza1,2; Laura Luzzatto2; Leonardo Albarello2; Renan Minotto2
Receipt date: 17/05/2020
Approval date: 13/08/2020
Financial Support: None
Conflict of Interest: None
Acknowledgments: We thank the Department of Dermatology of the Santa Casa de Misericórdia, Porto Alegre.
Study conducted at the Department of Dermatology, Irmandade Santa Casa de Misericórdia de Porto Alegre, Porto Alegre (RS), Brazil.
INTRODUCTION: Onychomatricoma is a rare benign tumor characterized by a clinical tetrad of a yellowish longitudinal band of varying thickness, splinter hemorrhages, longitudinal and transverse hypercurvature of the nail plate, and digitiform projections emerging from the nail matrix, leaving cavitations in the nail plate. We report a case of a female patient, 49 years old, with a history of a tumoral lesion in the third left toe for about four years, with a progressive increase in this period. Physical examination revealed an exuberant tumor lesion clinically compatible with onychomatricoma, confirmed by pathological examination after complete tumor excision.
Keywords: Nails; Nail diseases; Neoplasms
Onychomatricoma is a rare benign tumor characterized by digitiform projections from the matrix, being the only tumor in which the lesion actively produces nail plate alteration.1,2 We report a case of an onychomatricoma presenting an exuberant aspect, highlighting the clinical characteristics and the diagnosis of the lesion.
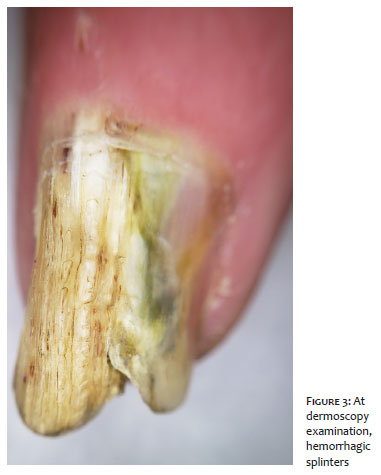
A 49-years-old woman, who works in the shoe industry, presented at the Dermatology Department with a tumoral lesion in the third left toe for about four years, with a progressive increase in this period. The patient denied pain or other injury-related symptoms. She had undergone several treatments for onychomycosis, without improvement. Physical examination revealed nail plate thickening, transverse hypercurvature, xanthonychia, hemorrhagic splinters, and small holes in the nail’s free edge (Figures 1 and 2). Dermoscopy of the blade surface allowed better visualization of the hemorrhagic splinters, and the free edge showed the presence of perforations (Figures 3 and 4).
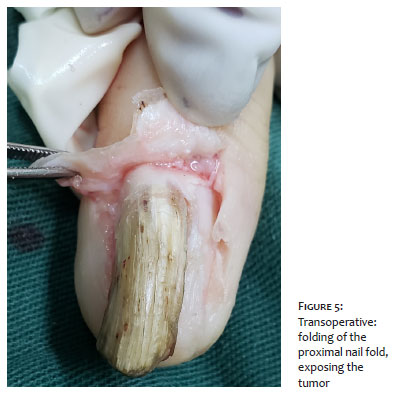
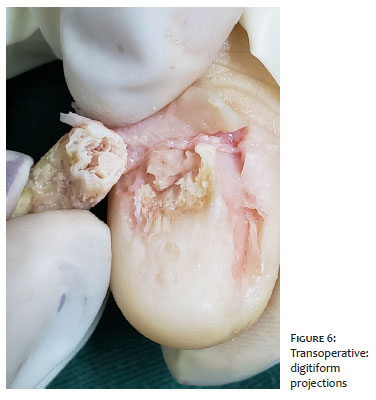
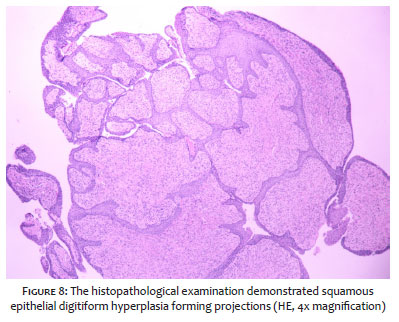
Due to suspected onychomatricoma, an excisional surgery of the lesion was performed. Two incisions were made in the proximal nail fold, which was rebound, exposing the tumor. The nail excision allowed the visualization of digitiform projections in the matrix area (Figures 5 and 6). We performed complete tumor excision and primary closure of the incisions in the proximal nail fold (Figure 7). The histopathologic exam demonstrated squamous epithelial digitiform hyperplasia forming projections, confirming the diagnosis of onychomatricoma (Figure 8).
A clinical tetrad characterizes the onychomatricoma, consisting of a yellowish longitudinal band of varying thickness, splinter hemorrhages, longitudinal and transverse hypercurvature of the nail plate, and digitiform projections emerging from the nail matrix, leaving cavitations in the nail plate.3,4 It may also manifest with longitudinal melanonychia, subungual hematoma, nail dystrophy, proximal nail fold verrucosity, dorsal pterygium, giant variant, pseudofibrokeratoma type, and may have characteristics similar to onychomycosis.4,5 Plaque dermoscopy demonstrates perforations in the distal portion of the nail plate, hemorrhagic striae, and white longitudinal grooves corresponding to the nail plate channels.1,4,6
Differential diagnoses include subungual exostosis, fibrokeratoma, vulgar wart, onychomycosis, squamous cell carcinoma, keratoacanthoma, superficial acral fibromyxoma, melanoma, bacterial infections, dermatofibrosarcoma protuberans, porocarcinoma, and osteochondroma. Onychomycosis is cited as a predisposing factor for the emergence of onychomatricoma (reactive lesion theory). On the other hand, the tumor can also be considered a predisposing factor for onychomycosis.6,7
Imaging exams such as radiography, ultrasound, and MRI may help in the diagnosis of the lesion. Still, in most cases, the clinical and dermoscopic examination associated with the pathological examination is sufficient for the diagnosis, as in the case reported.8,9 Anatomopathological examination demonstrates a fibroepithelial tumor composed of two portions. The first portion, proximal, is located under the posterior nail fold, characterized by epithelial invaginations filled with a thick V-shaped keratinized zone, well-defined fibrillar and fibrocystic stroma, and thickening of the nail plate. Digitiform projections, perforations in the nail plate and deep, poorly delimited penetration of the connective stroma in the dermis characterize the second portion, the distal area in the lunula.10
The treatment of onychomatricoma is surgical, and a complete tumor excision should be performed. The long-term prognosis is generally favorable, but nail dystrophies are common.11
Manoella Freitas Santos | 0000-0002-5024-5976
Approval of the final version of the manuscript; study design and planning; preparation and writing of the manuscript; intellectual participation in propaedeutic and/or therapeutic conduct of studied cases; critical literature review; critical revision of the manuscript.
Maria Emilia Vieira de Souza | 0000-0001-6717-8362
Approval of the final version of the manuscript; study design and planning; preparation and writing of the manuscript; intellectual participation in propaedeutic and/or therapeutic conduct of studied cases; critical literature review; critical revision of the manuscript.
Laura Luzzatto | 0000-0002-4193-6943
Approval of the final version of the manuscript; study design and planning; preparation and writing of the manuscript; data collection, analysis, and interpretation; active participation in research orientation; intellectual participation in propaedeutic and/or therapeutic conduct of studied cases; critical literature review; critical revision of the manuscript.
Leonardo Albarello | 0000-0002-8785-6885
Approval of the final version of the manuscript; study design and planning; preparation and writing of the manuscript; data collection, analysis, and interpretation; active participation in research orientation; intellectual participation in propaedeutic and/or therapeutic conduct of studied cases; critical literature review; critical revision of the manuscript.
Renan Minotto | 0000-0002-1451-0461
Approval of the final version of the manuscript; study design and planning; preparation and writing of the manuscript; data collection, analysis, and interpretation; active participation in research orientation; intellectual participation in propaedeutic and/or therapeutic conduct of studied cases; critical literature review; critical revision of the manuscript.
1. Haneke E, Franken J. Onychomatricoma. Dermatol Surg. 1995;21(11):984-7.
2. Ko CJ, Shi L, Barr RJ, Molne L, Ternesten-Bratel A, Headington JT. Unguioblastoma and unguioblastic fibroma an expanded spectrum of onychomatricoma. J Cutan Pathol. 2004;31(4):307-11.
3. Thomas L, Zook EG, Haneke E, Drapé JL, Baran R. Tumors of the nail apparatus and adjacent tissues. In: Baran R, de Baker DAR, Holzberg M, Thomas L. Baran and Dawber''s diseases of the nails and their management. 4th ed. USA: Wiley-Blackwell; 2012. p. 637-743.
4. Perrin C, Baran R. Onychomatricoma with dorsal pterygium: pathogenic mechanisms in 3 cases. J Am Acad Dermatol. 2008;59(6):990-4
5. Goettmann S, Zaraa I, Moulonguet I. Onychomatricoma with pterygium aspect: unusual clinical presentation. Acta Derm Venereol. 2006;86(4):369-70.
6. Baran R, Nakamura R. Doença das Unhas: do diagnóstico ao tratamento. Rio de Janeiro: Elsevier; 2011.
7. Cañueto J, Santos-Briz Á, García JL, Robledo C, Unamuno P. Onychomatricoma: genome-wide analyses of a rare nail matrix tumor. J Am Acad Dermatol. 2011;64(3):573-8.
8. Rosamary Soto, Ximena Wortsman, Yamile Corredoira. Onychomatricoma: Clinical and Sonographic Findings. Arch Dermatol. 2009;145(12):1461-2.
9. Goetmann S, Drapé JL, Baran R, Perrin C, Haneke E, Belaï ch S. Onychomatricome: 3nouveaux cas: intérêt de la résonance magnétique nucléaire. Ann Dermatol Venereol. 1994;121(Suppl 1):S145.
10. Perrin C, Goettmann S, Baran R. Onychomatricoma: clinical and histopathologic findings in 12 cases. J Am Acad Dermatol. 1998;39(4 pt 1):560-4.
11. Di Chiacchio N, Richert B, Haneke E. Surgery of the matrix. In: Richert B, Di Chiacchio N, Haneke E. Nail Surgery. New York: Informa Healthcare. 2011; p 103-32.
 All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773
All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773



 Read in Portuguese
Read in Portuguese
 Portuguese PDF
Portuguese PDF
 Print
Print
 Send this article by email
Send this article by email
 How to cite this article
How to cite this article
 Submit a comment
Submit a comment
 Mendeley
Mendeley
 Pocket
Pocket
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}