


Raíssa Rigo Garbin1; Gabriela Leiria Bencke1; Ciro Paz Portinho2; Fernando Eibs Cafrune1
Receipt date: 15/04/2020
Approval date: 17/07/2020
Financial Support: None
Conflict of Interest: None
Acknowledgments: We thank to the Dermatology Service staff at the Santa Casa de Misericórdia in Porto Alegre.
Study conducted at the Irmandade Santa Casa de Misericórdia de Porto Alegre, Porto Alegre (RS), Brazil.
The ear is one of the regions with the highest prevalence of cutaneous tumors. The reconstruction of auricular defects resulting from its excision tends to be complicated, especially when extensive and of the total thickness. We report two cases of reconstruction of surgical defects due to the resection of auricular basal cell carcinomas by Mohs micrographic surgery. One case was reconstructed through an interpolated island flap mobilized from the retroauricular region through the primary defect itself, and the other by retroauricular skin flap with anterior rotation through the primary defect. Both presented satisfactory aesthetic and functional results.
Keywords: Mohs Surgery; Skin Neoplasms; Surgical Flaps
Non-melanoma cutaneous neoplasms are prevalent and affect preferentially photoexposed areas, especially head and neck. Its treatment is eminently surgical, aiming to obtain tumor-free margins. Areas of aesthetic and functional importance are usually affected, which refers to the complexity of the surgical defects reconstruction in these places, such as the auricular pavilion.1,2 The objective of this study was to report two cases of total thickness auricular defects reconstruction through cutaneous flaps.
Case 1
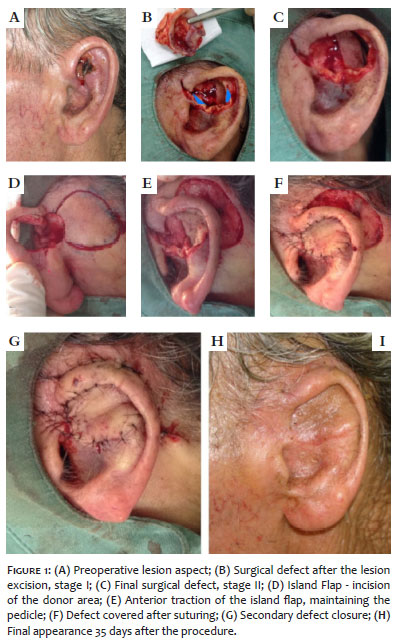
A 68-year-old man presented infiltrative basal cell carcinoma in the left ear, affecting the anti-helix, triangular fossa, and the anterosuperior portion of the helix (Figure 1A). He was submitted to two-stage Mohs micrographic surgery (Figures 1B and 1C) with total excision of the invading lesion, in addition to the anterior ear skin and posterior ear cartilage and skin. Removal of the tumor resulted in an extensive full-thickness auricular defect. We chose an interpolated island flap brought from the retroauricular region to the anterior auricular region for the reconstruction. After anesthesia with bupivacaine, the ear was folded anteriorly, and the donor area was demarcated immediately posterior to the retroauricular groove. An island-shaped incision was performed, maintaining an intact subcutaneous pedicle (Figure 1D). The flap was then mobilized to the anterior auricular region through the primary defect, attempting to avoid twisting, traction, or compression of the pedicle, causing vascular involvement (Figure 1E). After placing the flap on the primary defect, it was sutured with 5-0 mononylon (Figure 1F). The ear’s upper face was later drawn towards the secondary defect and fixed to the retroauricular region (Figure 1G), leaving only a small area to heal by secondary intention. The surgery was performed in a single stage, under sedation and local anesthesia, without complications and with adequate aesthetic and functional results (Figure 1H).
Case 2
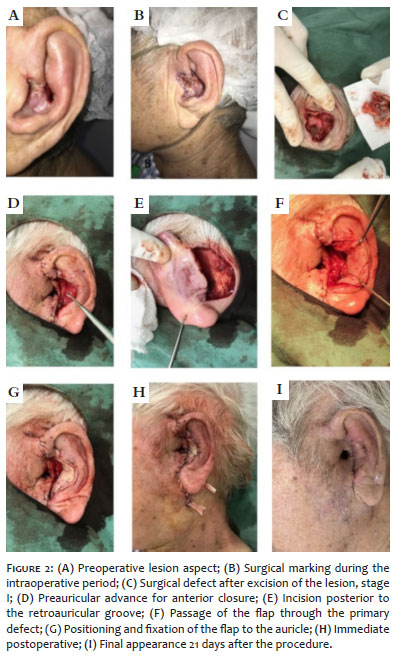
An 85-year-old woman presented extensive infiltrative basal cell carcinoma affecting the entire concha auricular, extending to the external acoustic meatus, tragus, crus of helix, and antihelix (Figure 2A and B). Previous magnetic resonance ruled out invasion of deep structures (vascular and neural). Under local anesthesia with bupivacaine and sedation, the patient was submitted to Mohs micrographic surgery, with total tumor excision in the second stage. The procedure resulted in an extensive and complex full-thickness surgical defect involving cartilage, subcutaneous tissue, and distal part of the external acoustic canal (Figure 2C). We performed closure with a retroauricular skin flap with anterior rotation through the primary defect. Initially, the anterior portion of the defect was closed with a pre-auricular flap followed by an incision in the central area to recreate the external acoustic meatus (Figure 2D). Afterward, we made a semilunar incision posterior to the retroauricular groove (Figure 2E) and, after detachment of the flap, we folded it forward through the surgical defect (Figure 2F) and sutured it to the concha (Figure 2G). A longitudinal fusiform incision was then made in the flap’s posterior region, so the anterior border was rotated toward the acoustic canal, against the preauricular flap, and the posterior border toward the mastoid region, setting the back face of the ear. A drain was maintained in the first seven postoperative days to avoid collections (Figure 2H) and evolved with good aesthetic and functional results (Figure 2I).
Approximately 90% of cutaneous neoplasias affect the head and neck, and basal cell carcinoma is the most prevalent histological type.3 The ear is one of the anatomical sites with the highest occurrence of carcinomas because of its projection to the head, making it more susceptible to ultraviolet radiation.4
Mohs micrographic surgery is the recommended treatment for extensive, infiltrative, and/or poorly delimited auricular basal cell carcinomas. The auricular defects reconstruction presents a challenge to the dermatological surgeon due to its curved and concave shape, the small amount of adjacent skin, and the difficulty in preserving the original auricular shape and support.2,3,5
The main options for anterior auricular defects correction, in which the primary closure would distort the ear format, are the use of grafts, flaps, or closure by secondary intention. When the defect is extensive, as in the cases reported, healing by secondary intention may cause contraction with consequent auricular form and auditory function alteration. The use of skin and cartilage grafts also has limited role for extensive defects, as their contraction tends to distort the ear’s structural support. Moreover, its aesthetic result is usually inferior to the use of flaps, especially due to the difficult equivalences of skin color and texture between the donor and recipient area.1,2,4,6
The retroauricular region functions as a skin reservoir. Because of its proximity to the defect, it is ideal for anterior ear surface reconstruction, resulting in similar skin color and texture, as well as mild scarring.7 The pull-through flap (Case 1) is based on the idea of passing a retroauricular flap through a tunnel in the cartilaginous structure (the primary defect itself, in the case reported) to reach the anterior auricular surface.1
The interpolated flap is an appropriate closure option for defects with significant auricular impairment, such as the subcutaneous pedicle flap, transferred from the retroauricular region to the anterior auricular region through the primary defect (Case 2).1,4,8 Masson first described it, and the procedure was called revolving door flap or flip-flop flap.3,4 Its advantages include the possibility of correcting large defects, the use of adjacent protected and vascularized skin, and the completion of the procedure in a single step.1,4,5,8
Surgical defects of the outer ear are especially challenging when extensive or affecting the cartilage because of auricular support loss. The small amount of adjacent free skin makes it difficult to reconstruct this anatomical region. Some closure options, such as primary, secondary intention, or use of grafts, have limited roles. In such cases, reconstruction with cutaneous flap is preferential, with favorable results.
Raíssa Rigo Garbin | 0000-0002-9771-1209
Approval of the final version of the manuscript; study design and planning; preparation and writing of the manuscript; critical literature review; critical revision of the manuscript.
Fernando Eibs Cafrune | 0000-0002-6645-0122
Approval of the final version of the manuscript; study design and planning; preparation and writing of the manuscript; active participation in research orientation; intellectual participation in propaedeutic and/or therapeutic conduct of studied cases; critical literature review; critical revision of the manuscript.
Gabriela Leiria Bencke | 0000-0002-1521-0452
Author’s contribution: Study design and planning; preparation and writing of the manuscript.
Ciro Paz Portinho | 0000-0001-7188-9423
Author’s contribution: Intellectual participation in propaedeutic and/or therapeutic conduct of studied cases.
1. Adler n, Ad-El D, Azaria R. Reconstruction of nonhelical auricular defects with local flaps. Dermatol Surg 2008;34(4):501-7.
2. Carrol BT, Gillen WS, Maher IA. Transpositional modification of the posterior auricular pull-through flap: a new twist. Dermatol Surg 2014;40(1):79-82.
3. Humphreys TR, Goldberg LH, Wiemer DR. The postauricular (Revolving Door) island pedicle flap revisited. Dermatol Surg 1996;22(2):148-50.
4. Nemir S, Hunter-Ellul L, Codrea V, Wagner R. Reconstruction of a large anterior ear defect after mohs micrographic surgery with a cartilage graft and postauricular revolving door flap. Case Rep Dermatol Med 2015:484819. Epub 2015 Sep 3.
5. Larcher L, Plotzeneder I, Tasch C, Riml S, Kompatscher P. Retroauricular pull-through island flap for defect closure of auricular scapha defects - a safe one-stage technique. Journal of Plastic, Reconstr Aesthet Surg 2011;64(7):934-6.
6. Redondo P, Lloret P, Sierra A, Gil P. Aggressive tumors of the concha: treatment with postauricular island pedicle flap. J Cutan Med Surg 2003;7(4):339-43.
7. Ali E, Nasrin N, Azin E. Aesthetic reconstruction of the upper antihelix in external ear with banner pullthrough flap. J Cutan Aesthet Surg 2015;8(4):218-221.
8. Braun JR M, Cook J. The Island Pedicle Flap. Dermatol Surg 2005;31(8 Pt 2):995-1005.
 All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773
All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773



 Read in Portuguese
Read in Portuguese
 Portuguese PDF
Portuguese PDF
 Print
Print
 Send this article by email
Send this article by email
 How to cite this article
How to cite this article
 Submit a comment
Submit a comment
 Mendeley
Mendeley
 Pocket
Pocket
{kind=link}
{kind=link}