


Flávia Trevisan1; Gabriela Ferreira Kalkmann2; Isabela do Prado Nascimento2; Emerson Luis Batista Filho2
Receipt date: 09/07/2020
Approval date: 07/09/2020
Financial Support: None
Conflict of Interest: None
Acknowledgments: We thank the residents of the Complex Dermatology Service of the Hospital de Clínicas, Universidade Federal do Paraná.
Study conducted at the Universidade Federal do Paraná, Curitiba (PR), Brazil.
INTRODUCTION: Acrochordons are very prevalent in dermatological offices and can reach almost 60% of the population over 70. One possible therapeutic approach is contact cryotherapy.
OBJECTIVES: Compare pain tolerance, aesthetic results, and the preference of participants for electrocoagulation or contact cryotherapy techniques in the treatment of acrochordons.
METHODS: Ten participants, with at least four acrochordons each, had their lesions divided into two groups. One group was submitted to electrocoagulation and the other to contact cryotherapy. We measured pain tolerance using the analog pain scale (EAD). The aesthetic result was assessed by visual comparison between the treatment groups in each participant, and the patient’s preference was evaluated by asking the participant objectively.
RESULTS: All points analyzed had statistical significance. The participants gave lower scores in EAD for lesions submitted to contact cryotherapy. The esthetic result evaluated after 30 days was superior in the lesions of the electrocoagulation group. All participants preferred the contact cryotherapy technique.
CONCLUSIONS: Contact cryotherapy is the preferred method with better pain tolerance in treating acrochordons, but the aesthetic result was better with electrocoagulation.
Keywords: Cryosurgery; Cryotherapy; Electrocoagulation; Electrosurgery; Fibroma
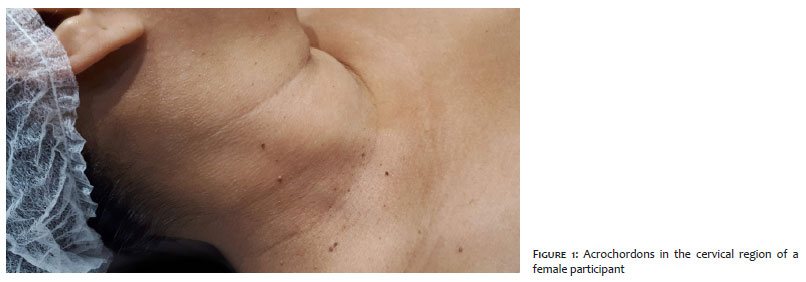
Acrochordons (or cutaneous fibroepithelial polyps or skin tags) are benign skin neoplasms easy to diagnose clinically (Figure 1). They are present in about 0.9% to 1.2% of dermatological consultations in the Brazilian adult population.1 They occur in 46% of people over 40, reaching 59% of individuals over 70.2,3
Although benign, they can cause significant discomfort to patients. Treatment techniques include tangential exeresis, chemiocauterization, electrosurgery, and cryotherapy.3 Since cryo-jet therapy can cause hypochromia in the surrounding skin due to the increased sensitivity of melanocytes to freezing, contact cryotherapy is a useful approach. Two previous publications described a similar procedure.4,5 This study aims to compare pain tolerance, aesthetic results, and the participant’s preference between electrocoagulation (ECG) and contact cryotherapy (CC), techniques in the treatment of acrochordons.
This is a prospective interventionist study with adult participants of both sexes, selected at the Complex Dermatology Clinic of the Hospital de Clínicas of the Federal University of Paraná, in Curitiba (PR), Brazil, from August to December 2019. The individuals had a clinical diagnosis of at least four acrochordons measuring from 2 mm to 5 mm.
The lesions of each participant were randomized into two groups. Group 1 underwent electrocoagulation (ECG), and group 2 underwent contact cryotherapy (CC).
After antisepsis with aqueous chlorhexidine digluconate solution 1%, the acrochordons from group 1 were submitted to electrocoagulation treatment with a high-frequency scalpel (Wavetronic 5000 Digital® Loktal, São Paulo, SP, Brazil, 60-100 Watts, coag mode, power 7), by direct contact of the active tip in the dry lesion, for four seconds.
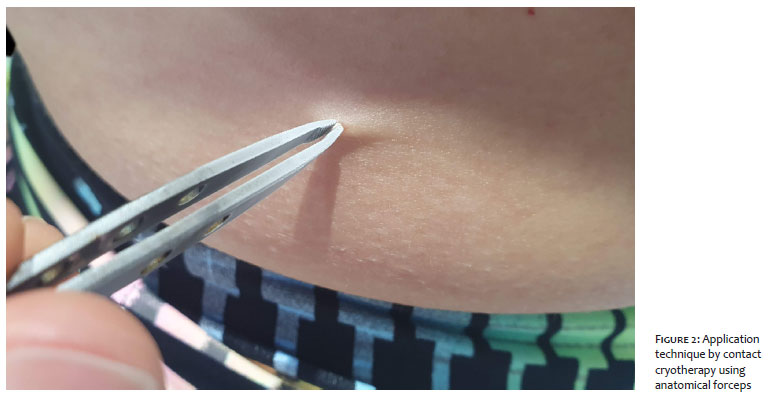
The lesions in group 2 were submitted to contact cryotherapy. After immersing the 10 cm anatomical forceps for 15 seconds in liquid nitrogen, the lesion was clamped. The contact with the surrounding skin was minimized for as long as possible during 10 seconds until bleaching, with defrost time equal to or greater than freezing time ( Figure 2).
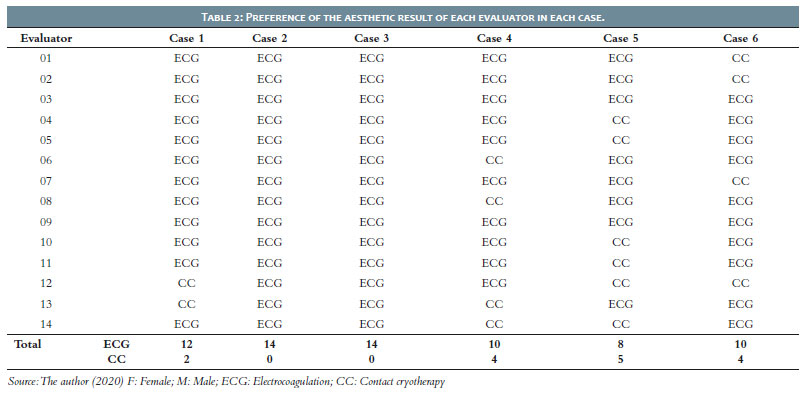
The degree of pain for each method was assessed using the pain analog scale (0 to 10, where 0 was no pain, and 10 was the worst pain the participant ever felt). The aesthetic result was assessed based on standardized photographs taken before and 30 days after the treatment. Fourteen experienced dermatologists analyzed the images on a computer screen, without knowing which treatment group each lesion was part of, choosing the one presenting the best aesthetic result.
The research ethics committee released the study under CAAE number 15233019.7.0000.0096. Statistical analysis was performed by parametric methods and comparison of means in the analysis of pain tolerance and non-parametric methods for the participant’s aesthetic result and preference (chi-square).
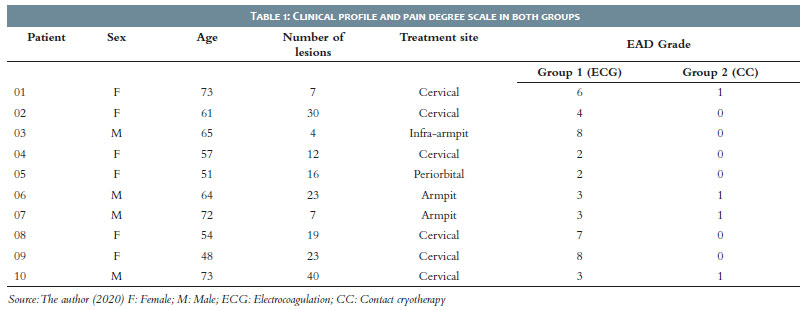
We selected 30 participants and, after applying the inclusion and exclusion criteria, we reached n = 10. There were four men and six women, with an average age of 61.4 years and an average number of lesions of 18.1. The most affected region was the cervical.
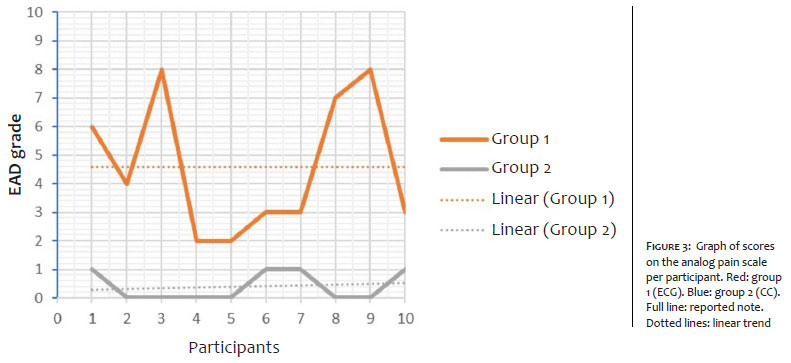
The degree of pain in group 1 ranged from 2 to 8, with a mean of 4.6 (SD = ± 2.41, var 5.82, mode 3) and in group 2, it ranged between 0 and 1, with a mean of 0.4 (SD = ± 0.52, var = 0.63, mode 0) (Table 1). All participants rated pain with the lowest score in group 2. The best pain tolerance in group 2 was statistically significant, with p<0.0001 (difference -4.20, CI -5.84 to -2.56) (Figure 3).
Six participants returned after 30 days. When assessing the aesthetic result (Table 2), the average percentage of preference was 80.95% for electrocoagulation and 19.05% for contact cryotherapy (p = 0.0013, CI 25.04% to 79.91%).
All participants preferred the contact cryotherapy technique. No participant had postoperative complications in any of the groups.
Pain sensitivity is very variable among participants. Its graduation can be entirely subjective, and EAD tries to make this analysis objective. In addition to the interpersonal difference in pain tolerance, the same individual may experience the painful sensation differently at different times and on each side of the body. Therefore, we compared the two techniques on the same participant, on the same day, and with a random selection of lesions.
Open cryo-jet therapy is widely used in dermatological practices. It has good applicability and low operating cost. However, the opening diameter can influence the level of pain, the halo of action, and the aesthetic result. Also, the outlet pressure of liquid nitrogen can cause apprehension and fright in the patient.
As the jet of liquid nitrogen forms a cone, a larger opening should be further away from the target, achieving more healthy skin. It creates a greater risk of sequelae, such as dyschromia, blistering, increased diameter, and the action halo’s deepening.4 With contact cryotherapy, the better accuracy to reach the target reduces this risk, especially in cases of pedunculated lesions such as the acrochordons.4,5
Most participants (6 out of 10) gave a score of 0 on EAD for the CC method, which demonstrated superiority in pain tolerance with good statistical significance (p<0.0001). This less painful sensitivity is extremely useful in the acrochordons treatment close to the eyes. It reduces the reflex of instinctive escaping or closing the eyes, very common in ECG cases without anesthesia or in open cryo-jet therapy.
The lower painful sensitivity of CC also allows excellent comfort to the patient, making it possible to treat a large number of acrochordons at the same time without the need for infiltrative anesthesia. It reduces the exposure to its risks, such as bruising, pain, or, exceptionally, intoxication, in addition to benefiting patients with needles phobia.
The good efficacy and the easiness of treating acrochordons by electrocoagulation are not denied. Still, contact cryotherapy adds up the advantages of its easy access in dermatological offices, fast learning, low technical complexity, non-interference with participants’ electronic devices (such as pacemakers and hearing aids), and the absence of need for sterile instruments such as the active tip of the electronic scalpel.
To assess the aesthetic result of the two techniques, photographic images with lighting and standardized equipment reduced the interpretation bias. For evaluating dermatologists, the technique used in each location was not mentioned.
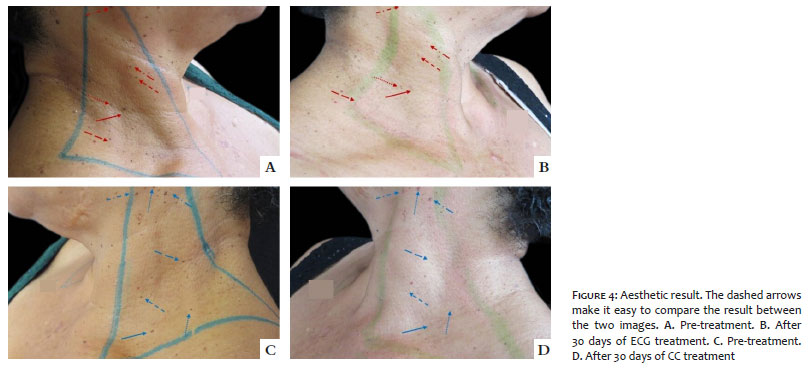
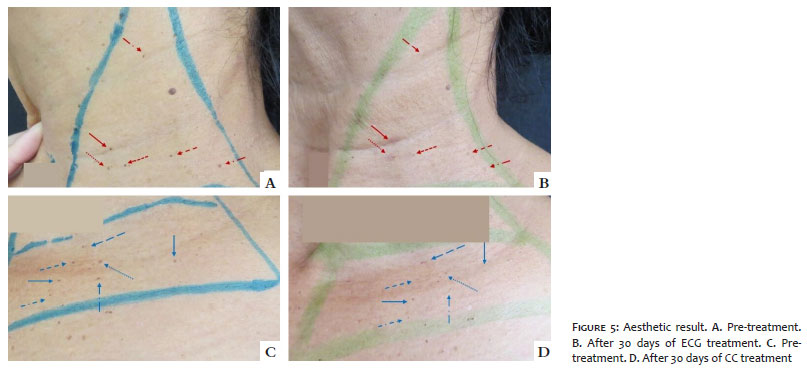
Lesions treated with ECG had an aesthetic result considered better than those treated with CC, with statistical significance when comparing the percentages of preferences using the chi-square method (Figures 4 and 5).
Although it was not the focus of this study, the authors observed that there were six cases of residual lesions in group 2 (submitted to contact cryotherapy). In one of the authors’ opinion, the larger acrochordons treated by contact cryotherapy need a time greater than 10 seconds or repetition of the freezing cycles for two or even three times, until slight erythema or edema of the lesion is observed.
When asked about the preference of the method, all patients chose contact cryotherapy as the best. Possible motivations for this choice are the lower pain of the method, the possibility of rapid application in several acrochordons, and its enormous practicality.
The removal of acrochordons by contact cryotherapy proved to be the preferred method among the participants, and it is less painful than the ECG. The aesthetic result after 30 days was superior for electrocoagulation.
Flávia Trevisan | 0000-0001-5855-3685
Análise estatística; aprovação da versão final do manuscrito; concepção e planejamento do estudo; elaboração e redação do manuscrito; obtenção, análise e interpretação dos dados; participação efetiva na orientação da pesquisa; participação intelectual em conduta propedêutica e/ou terapêutica de casos estudados; revisão crítica da literatura; revisão crítica do manuscrito.
Gabriela Ferreira Kalkmann | 0000-0003-0040-7591
Obtenção, análise e interpretação dos dados; revisão crítica da literatura.
Isabela do Prado Nascimento | 0000-0002-3436-9311
Obtenção, análise e interpretação dos dados; revisão crítica da literatura.
Emerson Luis Batista Filho | 0000-0002-2124-5715
Obtenção, análise e interpretação dos dados; revisão crítica da literatura.
1. Sociedade Brazileira de Dermatologia. Perfil nosológico das consultas dermatológicas no Brazil. An Bras Dermatol. 2006;81(6):549-58.
2. Banik R, Lubach D. Skintags: localization and frequencies according to sex and age. Dermatologica. 1987;174(4):180-3
3. Belgam Syed SY, Lipoff JB, Chatterjee K. Acrochordon. [atualização em 24 de março de 2020]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2020. Disponível em: https://www.ncbi.nlm.nih.gov/books/NBK448169/
4. Goodheart HP. Surgical Pearl: a rapid technique for destroying small skin tags and filiform warts. Dermatol Online J. 2003;9(5):34.
5. Taylor JE, Osmun WE. Just a pinch: technique for skin tag removal in sensitive areas. Can Fam Physician. 2016;62(12):998-9.
 All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773
All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773



 Read in Portuguese
Read in Portuguese
 Portuguese PDF
Portuguese PDF
 Print
Print
 Send this article by email
Send this article by email
 How to cite this article
How to cite this article
 Submit a comment
Submit a comment
 Mendeley
Mendeley
 Pocket
Pocket
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}