


Dhesi Ariembi1,2; Retno Indar Widayati1,2; Diah Adriani Malik1,2
Receipt date: 30/06/2020
Approval date: 07/09/2020
Financial Support: None
Conflict of Interest: None
Study conducted at the Medical School of the Diponegoro University and the Hospital Dr. Kariadi Semarang, Indonesia.
INTRODUÇÃO: O melasma é uma hiperpigmentação simétrica adquirida que afeta mais comumente as áreas expostas ao sol.
OBJETIVO: Este estudo tem como objetivo provar a eficácia do tratamento com creme com ácido tranexâmico a 4% em pacientes com melasma tratados com laser QS Nd:YAG 1064 nm de baixa fluência.
MÉTODOS: Os sujeitos do estudo foram divididos em dois grupos, A e B, que receberam terapia a laser QS Nd:YAG 1064 nm de baixa fluência dia inicial do estudo, e após 4 e 8 semanas. O grupo A recebeu creme com ácido tranexâmico a 4% (AT) e o grupo B recebeu creme com placebo, aplicado duas vezes ao dia durante 12 semanas. A avaliação utilizou as pontuações MASI e MELASQoL.
RESULTADOS: O resultado mostrou que o creme AT a 4% foi eficaz na redução dos escores MASI e MELASQoL em pacientes com melasma tratados com laser QS Nd:YAG 1064 nm de baixa fluência.
CONCLUSÕES: O creme AT 4% foi eficaz na redução dos escores MASI e MELASQoL em pacientes com melasma tratados com laser QS Nd:YAG 1064 nm de baixa fluência.
Palavras-chave: Creme para a Pele; Melanose; Terapia a Laser
ABSTRACT
INTRODUCTION: Melasma is acquired symmetric hyperpigmentation that affects most commonly in sun-exposed areas.
OBJECTIVE: This study aim to prove the effectiveness of 4% tranexamic acid cream (AT) treatment for melasma patients treated with low-fluence QS Nd:YAG 1064-nm laser.
METHODS: The study subjects were divided into two groups A and B who received low-fluence QS Nd:YAG 1064-nm laser therapy at baseline, fourth week, and eighth week. Group A received Tranexamic acid 4% (TA) cream, and group B received a placebo cream, applied twice a day for 12 weeks. The assessment uses MASI and MELASQoL scores.
RESULTS: The result showed that TA 4% cream was effective in reducing MASI and MELASQoL scores in melasma patients treated with low-fluence QS Nd:YAG 1064-nm laser.
CONCLUSIONS: TA 4% cream was effective in reducing the MASI and MELASQoL scores in melasma patients treated with low-fluence QS Nd:YAG 1064\\\-nm laser.
Keywords: Melanosis; Laser Therapy; Skin Cream
Melasma comes from the Greek melas, which means black patches, or chloazein, which means green. Melasma is more common in women than in men. This disorder runs chronic and tends to recur.1,2 Melasma mainly occurs in Fitzpatrick III–V skin types, living in areas with high-intensity ultraviolet light.3
Melasma can affect all races, mostly Asian, Hispanic, Latin American, and Arabic. Handel et al. mentioned a melasma prevalence of 8.4% of dermatology cases in Brazil, 14.5% in the Arabian population in Detroit (USA), and 8.8% in the Latin population in Texas (USA).4 Melasma covers 50% of the aesthetic cases in Asia.5,6 The incidence of melasma in Southeast Asia was 40% of women and 20% of men.5 In Indonesia, the ratio of women and men who suffers from melasma is 24:1.7
The pathogenesis of melasma is not clear until now. The main predisposing factors include genetic, ultraviolet rays, and hormonal exposure.2,3 The clinical features of melasma are brown, dark brown, or black macules, symmetrical, with irregular borders, single or multiple, found in the forehead, temple, upper lip, cheeks, and other parts exposed to sunlight. Melasma based is divided into three distinctive patterns on the distribution of lesions: centrofacial (65%), malar (20%), and mandibular (15%).8,9
Wood’s lamps and histopathological examination can be used to determine the depth of the melasma pigment. Based on Wood’s lamp examination, melasma is divided into three types: epidermal, dermal, and mixed.7 Research that assesses the validity of Wood’s lamp to identify melasma patterns compared to histopathology showed the level of sensitivity, low specificity, and low accuracy (46%) in all three types of melasma pathology.10
The basic principles of melasma management are suppressing melanocyte proliferation, inhibiting melanosome formation, and increasing melanosome degradation.8 Research on melasma therapy has been conducted with varying results. However, until now, there has not been a single effective therapy with satisfactory results.11,12
Tranexamic acid is a synthetic derivative of the lysine amino acid, which reduces the activity of melanocyte tyrosinase involved in melanogenesis.11,13 Tranexamic acid can be administered systemically or topically; however, serious adverse events have been reported on tranexamic acid when given systemically. Still, it is safer when given topically.14
Low-fluence Q-switched neodymium-doped yttrium aluminum garnet (QS Nd:YAG) 1064-nm laser is one of the modalities used in melasma therapy, through a sub-thermolytic mechanism. Research on low-fluence QS Nd:YAG 1064-nm laser in melasma has been carried out. Still, high recurrence rates after laser therapy and poor long-term results are observed when low-fluence QS Nd:YAG 1064-nm laser is used as monotherapy.15 Some of the researchers concluded that to get better results in melasma treatment with low-fluence QS Nd:YAG 1064-nm laser, it should be combined with other therapies including topical agents such as tranexamic acid.16
Research combination of tranexamic acid 4% cream and low-fluence QS Nd:YAG 1064-nm laser has not been conducted in Indonesia. It led to a high recurrence rate in melasma and various adverse events arising from the treatment. Thus, effective combination therapy with minimal adverse events is needed. We conducted this study to prove the effectiveness of tranexamic acid 4% cream in melasma treatment with low-fluence QS Nd:YAG 1064-nm laser.
The difference between this study and the previous research conducted by Laothaworn et al. is the sample number’s research design, as many as 16 people, and how the subjects were treated. The treatment duration was 12 weeks, and the parameters assessed in this study were MASI and MELASQoL scores.
This study is a double-blind, randomized, controlled, two-groups, pre and post-design trial. This study population’s criteria were all melasma patients seeking treatment at the Dermatology and Venereology Clinic of the Diponegoro National Hospital from August to October 2019. The study subjects comprised 16 melasma patients diagnosed clinically and by Wood’s lamp examination, who were over 20 years of age, had Fitzpatrick skin type IV-V, and willing to participate and obtain therapy in the research. Patients received an explanation of the therapeutic procedure and signed informed consent.
Exclusion criteria included a history of allergy to tranexamic acid, pregnancy or breastfeeding, using hormonal contraception, active infection in the area of melasma, and history of hypertrophy or keloid scar. Patients with a history of oral retinoid consumption or topical facial lightening treatment products must stop these medications at least one year and one month before the first visit. Furthermore, patients with a history of receiving oral tranexamic acid therapy or undergoing cosmetic procedures on the face (laser, dermabrasion, chemical peels) must stop these medications at least six months before the first visit.
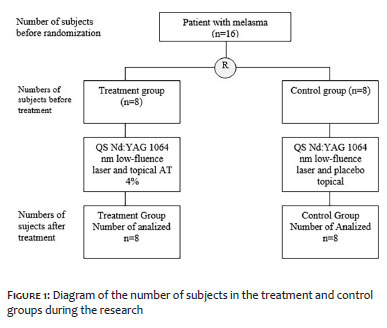
Consecutive sampling, conducted upon the patient’s arrival, selected research subjects, and we performed block randomization. The study subjects were divided into two groups: A and B. Both groups received low-fluence Q-switched Nd:YAG 1064-nm laser therapy at baseline, fourth, and eight weeks. After the laser therapy, group A received tranexamic acid 4% cream, and group B received placebo cream, applied twice a day for 12 weeks. MASI and MELASQoL scores were assessed in both groups at baseline and after twelve weeks.
MASI score parameters are expressed as mean and standard deviations because they are normally distributed. In contrast, MELASQoL scores are expressed as medians, minimum, and maximum values due to abnormal distribution. The Shapiro-Wilk test conducted the normality test because the sample size was small (number of samples <50).
The hypothesis tested the mean difference of MASI scores before and after treatment with paired t-test. An unpaired t-test carried out the hypothesis test of differences in MASI scores and delta MASI scores between the treatment and control groups.
The Wilcoxon test assessed the hypothesis of MELASQoL average scores before and after treatment. The Mann–Whitney test carried out the hypothesis testing of MELASQoL score differences between the treatment and control groups. An unpaired t-test examined the difference in MELASQoL delta scores between the treatment and control groups.
Differences were considered significant if p<0.05. Data analysis used the IBM SPSS program version 25.
The Health Research Ethics Commission of the Faculty of Medicine, Diponegoro University granted the study protocol’s ethical clearance under the No.222/EC/KEPK/FK UNDIP/V/2019.
Study subjects as many as 16 people completed all the series of therapies in this research. Figure 1 shows the number of subjects in the treatment and control group during the study.
The research subjects were 16 melasma individuals: nine presented centrofacial distribution (56.3%), and seven, malar distribution (43.7%). The results of Wood’s lamp examination found a mixed type of melasma in 13 subjects (81.3%), followed by epidermal types in three individuals (18.2%).
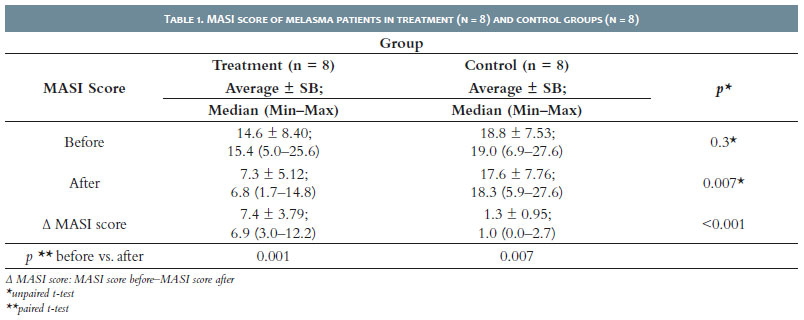
Table 1 presents the MASI analysis scores in both groups, showing decreased MASI scores in both groups.
The average MASI score of the treatment group at the beginning of the research was 14.6 ± 8.40; at the end of the study, it dropped significantly to 7.3 ± 5.12 (p = 0.001; paired t-test). The average MASI score of the control group at the beginning was 18.8 ± 7.53 and also dropped significantly to 17.6 ± 7.76 (p = 0.007; paired t-test).
At baseline, the average of MASI score in the treatment group was 14.6 ± 8.40, lower than the control group’s score, which was 18.8 ± 7.53. However, the statistical test results showed the difference of the MASI score before the treatment was not significant (p = 0.3; unpaired t-test).
The average MASI score after treatment was 7.3 ± 5.12. This score was lower than the average MASI score of the control group, 17.6 ± 7.76. Statistical test results showed that the difference in MASI score after treatment was significant (p = 0.007; unpaired t-test).
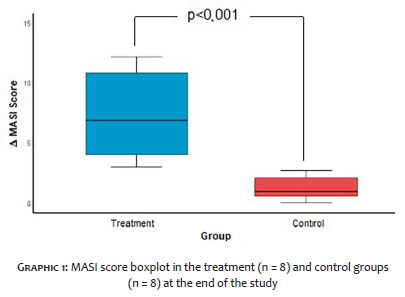
The treatment group’s average MASI score was 7.4 ± 3.79, which was significantly higher than the control group’s MASI score, 1.3 ± 0.95 (p<0.001; unpaired t-test). Graphic 1 shows the average change in MASI scores from before to after treatment.
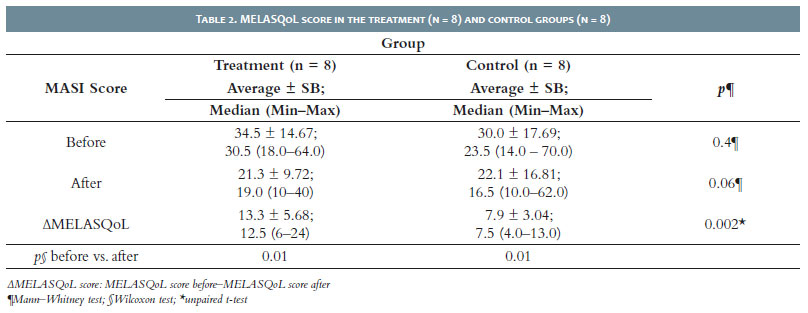
Table 2 presents an analysis of MELASQoL scores in both groups. There was a decrease in MELASQoL scores in both groups. The MELASQoL average score of the treatment group at baseline was 34.5 ± 14.67, and at the end of the study, it dropped significantly to 21.3 ± 9.72 (p = 0.01; Wilcoxon test). The MELASQoL average score of the control group at the beginning was 30.0 ± 17.69; at the end of the study, it dropped significantly to 22.1 ± 16.81 (p = 0.01; Wilcoxon test).
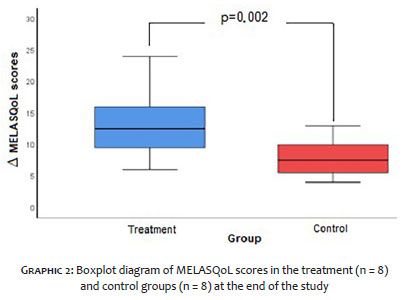
The MELASQoL score of the treatment group was 13.3 ± 5.68, significantly higher than the control group, which was 7.9 ± 3.04 (p = 0.002; unpaired t-test).
Graphic 2 presents the comparison of ¿MELASQoL scores between the treatment and control groups.
Melasma is an acquired hyperpigmentation disorder that is most commonly found in Asian women. Management of melasma is difficult due to the high recurrence rate.17 First-line therapy includes controlling risk factors, using sunscreen, stopping hormonal therapy or photosensitizer drugs, and using topical anti-tyrosine and topical exfoliants. The second-line uses an association of first-line and chemical peels. The third-line is the combination of the first-line with a non-ablative fractional laser or fractional radiofrequency. The fourth-line is the first-line combined with Intense Pulse Light or Q-switch laser.15
Topical therapy is more effective for epidermal melasma. Patients can obtain it at an affordable price, but it requires regular daily use. Procedural treatment, such as chemical peels and micro-needling, can also be used in the epidermal type of melasma. Lasers and other light-based energy are an alternative for dermal and mixed type melasma or recalcitrant melasma. However, the treatment costs are high, and the treatment must be repeated for several months. Thus, the physician must inform the patient before starting the therapy. Systemic therapy can use oral Tranexamic Acid (TA) for dermal or mixed melasma, or melasma resistant to topical treatment. Still, users must be careful with systemic adverse events, including gastrointestinal disorders, menstrual disorders, and the most severe event reported, deep vein thrombosis.2,16
The choice of melasma therapy depends on the melasma type, Fitzpatrick’s skin type, history of previous therapy, and patient expectations. In addition to the patient’s adherence and the treatment costs, melasma therapy also requires a long time because the therapeutic effect is usually seen only after one-two months.8 Combination therapy with topical and procedural preparations is the most widely used melasma therapy option currently, including QS Nd:YAG laser modality combined with topical preparations.11,12
Hydroquinone is the best standard for depigmenting agents for melasma. Nevertheless, long-term hydroquinone can cause exogenous ochronosis.2,5 Other alternative topical therapies not containing hydroquinone are available, for example, tranexamic acid.2 Janney et al. compared 5% TA solution and hydroquinone cream: the combination achieved a 27% MASI decrease in the TA solution group and 5% and 26.7% in the hydroquinone group, with erythema and irritation adverse events found in the hydroquinone group. This study showed that the TA 5% solution effectiveness as melasma therapy was almost the same as hydroquinone.18
Tranexamic acid (trans-4-(aminomethyl) cyclohexane-carboxylic acid) is a synthetic derivative of the amino acid lysine, a competitive inhibitor of activation of plasminogen activator (PA) through reversible interactions at lysine-binding sites. Tranexamic acid (TA) reduces PA activity, thereby preventing the conversion of plasminogen to plasmin.19 Another mechanism of action of tranexamic acid is the melanocyte tyrosinase activity reduction to prevent the binding of plasminogen to keratinocytes, resulting in decreased prostaglandin and arachidonic acids involved in melanogenesis.11,13,18
Tranexamic acid as a therapy for melasma is available in topical, oral, and intradermal injection preparations. Moreover, it can be combined with other therapeutic modalities. Melasma therapy with topical tranexamic acid has minimal adverse events in the form of erythema and irritation, and it is safe for long-term use. 20,21
The laser is one of the most critical therapeutic instruments in the dermatology field, including melasma.22 Traditional QS laser (high fluence) is effective for pigmented lesions treatment through selective targets for melanin. However, several studies have shown some adverse events, including hyperpigmentation, hypopigmentation, and melasma recurrence.5 The new variant of the QS Nd: YAG laser is called low-fluence or sub-thermolytic. The laser is the same but with lower fluence than traditional QS. Low-fluence therapy mostly uses a wavelength of 1064 nm, which penetrates deeper into the dermis, avoiding damage to the epidermis, and can be used on darker skin.23 Sub-thermolytic therapy is based on the theory that pigment disorders occur through photoacoustic mechanisms that damage the melanin pigment, whereas keratinocytes and melanocytes are protected from the damage.24 Low-fluence laser causes minimal thermal damage, decreases the number of melanosomes (especially stage IV melanosomes), not damaging the melanocytes, but lowering its volume and dendrites.25 Nevertheless, there is still damage that accompanies QS sub-thermolytic therapy, but this damage is reported to be less than that caused by traditional photothermal therapy.15,26
Low-fluence Q-switched Nd:YAG laser is used as a therapy for melasma, despite the reported transient response and adverse events including erythema, edema, hypopigmentation spots, recurrence, and hyperpigmentation rebound. The literature recommends this laser not to be used in too many sessions (>6–10 times) or too often (intervals every week) to avoid adverse events.27
In this study, the treatment group’s MASI score was significantly lower than before the treatment (p<0.001). The study’s results are consistent with the research conducted by Ebrahimi et al. in 50 melasma patients. The study compared a TA 3% solution with hydroquinone solution 3% combined with dexamethasone 0.01%, and showed a significant decrease in MASI scores in both groups.28 Other studies conducted by Atefi et al. in 60 melasma patients compared those who received TA 5% topical to those who received hydroquinone 2%. The research showed a more significant decrease in the TA group’s MASI score, proving that topical TA can reduce the MASI scores, being effective and safe as a melasma therapy with minimal adverse events compared to hydroquinone.11,29
MASI scores in the control group after treatment were significantly lower than before treatment. Research conducted by Suh et al. on 23 melasma individuals treated with a low-fluence QS Nd:YAG 1064-nm laser every week for ten weeks showed a significant decrease in MASI score at week seven (7.57 ± 2.91) and week 10 (9.15 ± 2.74) compared to before treatment (14.15 ± 1.47), with a p-value <0.05.30 Another study conducted by Kar found a significant reduction in MASI score of 47.93% (p<0.05) in group A that received low-fluence QS Nd:YAG 1064-nm laser therapy, followed by 40.44% (p<0.05) in group B, which received Glycolic Acid peeling therapy, and 20.81% (p<0.05) in group C, which received high-fluence QS Nd:YAG 1064-nm laser therapy. Most adverse events were found in group C.17 Thus, low-fluence QS Nd:YAG 1064-nm laser is effective for melasma.
Statistical test results of MASI score of the treatment group were significantly higher than the control group (p<0.001; unpaired t-test). Research conducted by Laothaworn et al. used MASI scores and showed a significant decrease in the treatment group combination of low-fluence QS Nd:YAG 1064 nm and TA 3% cream since four weeks after the first laser, and this continued to decline until final observation.12
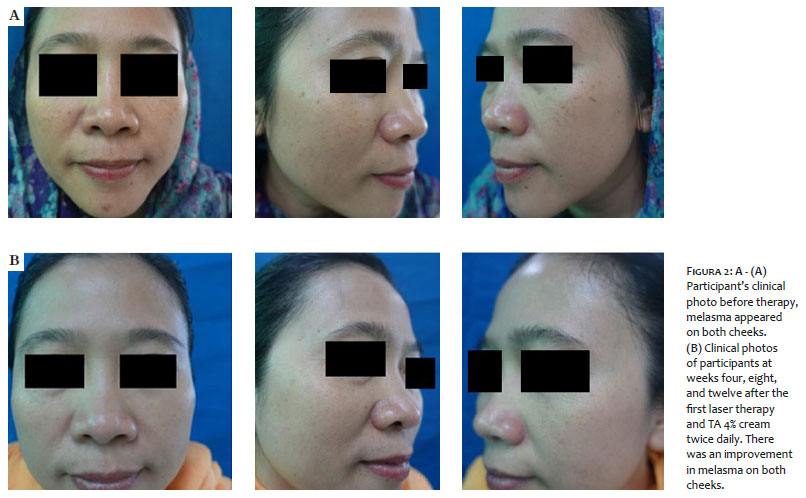
This study conducted low-fluence QS Nd:YAG 10640-nm laser three times at 4-week intervals. The TA 4% cream was applied morning and afternoon for three consecutive months and stopped one day after the laser therapy administration. Participants got some clinical photos before and after treatment with TA 4%, shown in Figure 2 and Figure 3. Previous research had proven the effectiveness of low-fluence QS Nd:YAG 1064-nm laser therapy and topical tranexamic acid for melasma. A research conducted by Laothaworn et al. evaluated the use of tranexamic acid 3% cream and low-fluence QS Nd:YAG 1064-nm laser combination.12
This study also assessed the MELASQoL score to see how melasma affected the patients’ quality of life.31 Significant decreases in MELASQoL scores were found in the treatment group after treatment (p=0.01). A substantial reduction in the MELASQoL score was also found in the control group after treatment (p=0.01). The statistical test results of the MELASQoL score in the treatment group were significantly greater than those in the control group (p = 0.002; unpaired t-test), (Figure 2 and 3).
Two subjects in this study complained of redness after the laser action, but the redness disappeared within 20–30 minutes after a cold compress. Based on Suh et al.’s research, 23 study subjects who received low-fluence QS Nd:YAG 1064-nm laser therapy had transient erythema and no other serious adverse events.30
MASI and MELASQoL scores in the treatment group decreased significantly compared to the control group. This study concluded that the TA 4% cream effectively reduced the MASI and MELASQoL scores in melasma patients treated with low-fluence QS Nd:YAG 1064-nm laser.
Observations in this study were only carried out within 12 weeks due to time constraints. Thus, we couldn’t observe the long-term effects of combination therapy of low-fluence QS Nd:YAG 1064-nm laser and TA 4% cream. We suggest future studies to use tools to measure pigment depth more objectively, with longer observation times.
Dhesi Ariembi | 0000-0002-0835-2938
Data collection, analysis, and interpretation; active participation in research orientation; intellectual participation in propaedeutic and/or therapeutic conduct of studied cases; critical literature review; critical revision of the manuscript.
Retno Indar Widayati | 0000-0002-5529-1963
Statistical analysis; approval of the final version of the manuscript; intellectual participation in propaedeutic and/or therapeutic conduct of studied cases; critical literature review.
Diah Adriani Malik | 0000-0003-0268-0655
Statistical analysis; approval of the final version of the manuscript; study design and planning; active participation in research orientation.
1. Lapeere H. Hipomelanosis and hypermelanosis. In: Goldsmith LA, Katz SI, Gilchrest BA, Paller AS, Leffell DJ, Wolff K, editors. Fitzpatrick's dermatology in general medicine. New York: Mc Graw Hill; 2012. p. 804-25.
2. Ogbechie-Godec OA, Elbuluk N. Melasma: an up-to-date comprehensive review. Dermatol Ther (Heidelb). 2017;7(3):305-18.
3. Serena NB, Bruce Smoller G. An overview on melasma. J Pigment Disord. 2015;2(10).
4. Handel AC, Miot LDB, Miot HA. Melasma: a clinical and epidemiological review. An Bras Dermatol. 2014;89(5):771-82.
5. Kauvar ANB. The evolution of melasma therapy: targeting melanosomes using low-fluence Q-switched neodymium-doped yttrium aluminium garnet lasers. Semin Cutan Med Surg. 2012;31(2):126-32.
6. Chatterjee M, Vasudevan B. Recent advances in melasma. Pigment Int. 2014;1(2):70.
7. Soepardiman. Kelainan pigmen [Pigment disorders]. In: Menaldi SL, Bramono K, Infriatmi W, Menaldi SL, Bramono KIW, editors. Ilmu penyakit kulit dan kelamin [Skin and venereal disease]. Jakarta: Fakultas Kedokteran Universitas Indonesia; 2015. p. 342-51.
8. Damevska K. New aspects of melasma/novi aspekti melazme. Serbian J Dermatol Venereol. 2014;6(1):5-18.
9. Asditya A, Sukanto H, Staf D, Fungsional M, Kesehatan I, Kedokteran F, et al. Studi retrospektif¿: profil pasien melasma [Retrospective study: profile of melasma patients]. BIKKK. 2017;29:220-8.
10. Novarina RM, Sukanto H. Gambaran dermoskopi dan lampu wood pada melasma (The description of dermoscopy and wood's lamp on melasma). BIKKK Periodic Dermatol Venereol. 2017;29:8-15.
11. Atefi N, Dalvand B, Ghassemi M, Mehran G, Heydarian A. Therapeutic effects of topical tranexamic acid in comparison with hydroquinone in treatment of women with melasma. Dermatol Ther (Heidelb). 2017;7(3):417-24.
12. Laothaworn V, Juntongjin P. Topical 3% tranexamic acid enhances the efficacy of 1064-nm Q-switched neodymium-doped yttrium aluminum garnet laser in the treatment of melasma. J Cosmet Laser Ther. 2018;20(6):320-5.
13. Batory M, Rotsztejn H. Topical Formulations and intradermal injections of tranexamic acid in the treatment of hyperpigmentation - A review. Lett Drug Des Discov. 2018;15(2):212-8.
14. Ayuthaya PKN, Niumphradit N, Manosroi A, Nakakes A. Topical 5% tranexamic acid for the treatment of melasma in asians: a double-blind randomized controlled clinical trial. J Cosmet Laser Ther. 2012;14(3):150-4.
15. Trivedi MK, Yang FC, Cho BK. A review of laser and light therapy in melasma. Int J Womens Dermatol. 2017;3(1):11-20.
16. Rodrigues M, Pandya AG. Melasma: clinical diagnosis and management options. Australas J Dermatol. 2015;56(3):151-63.
17. Kar HK, Gupta L, Chauhan A. A comparative study on efficacy of high and low fluence Q-Switched Nd:YAG laser and glycolic acid peel in melasma. Indian J Dermatol Venereol Leprol. 2012;78(2):165-71.
18. Janney MS, Subramaniyan R, Dabas R, Lal S, Das NGS. A randomized controlled study comparing the efficacy of topical 5% tranexamic acid solution versus 3% hydroquinone cream in melasma. J Cutan Aesthet Surg. 2019;12(1):63-7.
19. Zhang L, Tan WQ, Fang QQ, Zhao WY, Zhao QM, Gao J, et al. Tranexamic acid for adults with melasma: a systematic review and meta-analysis. Biomed Res Int. 2018;2018:1683414.
20. George A. Tranexamic acid: an emerging depigmenting agent. Pigment Int. 2016;3(2):66.
21. Laothaworn, Deeanandlarp, Pattaraarchachai, Juntongjin. Effect of adjuvant tranexamic acid on melasma-a pilot study. Thai J Pharm Sci. 2016;40:184-7.
22. Haley D, Pratt O. Basic principles of lasers. Anaesth Intensive Care Med. 2017;18(12):648-50.
23. Jordão JM, Rebellato PRO. Energy-based devices for treatment of melasma. J Surg Dermatol. 2017;2(T1):130-8.
24. Tse TW, Hui E. Tranexamic acid: an important adjuvant in the treatment of melasma. J Cosmet Dermatol. 2013;12(1):57-66.
25. Cho HH, Choi M, Cho S, Lee JH. Role of oral tranexamic acid in melasma patients treated with IPL and low fluence QS Nd:YAG laser. J Dermatol Treat. 2013;24(4):292-6.
26. Park YW, Yeo UC. Mottled hypopigmentation from laser toning in the treatment of melasma: a catastrophic or manageable complication? Med Lasers. 2015;4(2):45-50.
27. Bevec Fotona T. Treating melasma with sub-thermolytic Q-Switched Nd:YAG. J LAHA 2011;2011(1):53-5.
28. Ebrahimi BNF. Topical tranexamic acid as a promising treatment for melasma. J Res Med Sci. 2014;19(8):753-7.
29. McKesey J, Tovar-Garza A, Pandya AG. Melasma treatment: an evidence-based review. Am J Clin Dermatol. 2020;21(2):173-225.
30. Lieu TJ, Pandya AG. Melasma quality of life measures. Dermatol Clin. 2012;30(2):269-80.
31. Suh KS, Sung JY, Roh HJ, Jeon YS, Kim YC, Kim ST. Efficacy of the 1064-nm Q-switched Nd:YAG laser in melasma. J Dermatolog Treat. 2011;22(4):233-8
 All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773
All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773



 Read in Portuguese
Read in Portuguese
 Portuguese PDF
Portuguese PDF
 Print
Print
 Send this article by email
Send this article by email
 How to cite this article
How to cite this article
 Submit a comment
Submit a comment
 Mendeley
Mendeley
 Pocket
Pocket
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}