


Célia Luiza Petersen Vitello Kalil1; Christine Chaves2; Artur Stramari De Vargas2; Valéria Barreto Campos3
Receipt date: 20/07/2020
Approval date: 07/09/2020
Financial Support: None
Conflict of Interest: None
Study conducted at the Célia Kalil Clinic, Porto Alegre (RS)
The number of evidence supporting the existence of a “gut-skin axis” correlation has grown. There is also a suggestion that the intestinal microbiota modulation may play an essential role in dermatological diseases. Studies have shown that probiotics' oral use can have beneficial effects in treating skin diseases with inflammatory origins such as atopic dermatitis, acne, and others. However, there is no standardization as to what doses or species should be used for the treatments. We provide an overview of the use of probiotics as a treatment for dermatological diseases, focusing on mechanisms of action and clinical results reported in the literature.
Keywords: Probiotics; Skin; Skin diseases
The importance of the human microbiome for health has been extensively researched in the last decade. Studies have shown that the microbiota and the host share a positive dependency, and the disruption in the balance between them can have significant consequences.1 In 2001, the World Health Organization (WHO) defined probiotics as living microorganisms that benefit humans and animals when consumed in adequate quantities.2
The intestinal microbiome strongly influences the host’s immune system by protecting against external pathogens and initiating immunoprotective responses.3 Thus, changes in the intestinal microbiome can lead to the development of inflammatory or autoimmune diseases in organs distant from the intestine, such as the skin.3 A considerable change in the relationship between the microorganisms that inhabit the intestine characterizes the intestinal dysbiosis, as well as the expansion of new bacterial groups, generating an imbalance in the microbiome and possible clinical effects in the human body.4 The number of evidence pointing to a correlation between the disease and intestinal dysbiosis has increased in common inflammatory dermatological diseases, such as atopic dermatitis (AD), acne vulgaris, psoriasis, rosacea, and even melasma (Table 1). Also, there is evidence that some peptide-secreting cells with regulatory function present in the skin, brain, and intestine would have the same embryonic origin in the ectoderm.5 This type of information corroborates and supports the existence of the “skin-gut axis”6 and “gut-brain-skin axis”, considering that the emotional state can influence the individual’s inflammatory state.7 Furthermore, recent research and hypotheses have suggested that the main mechanism by which the skin and the intestine microbiota can affect each other is through modulation of the endocrine and immune system.3
The use of probiotics to manipulate the intestinal flora and thus obtain positive results in organs distant from the intestine, such as the skin, is an old practice. However, there is no standardization regarding which doses or species should be used for treatments. This study aims to overview the use of probiotics as a treatment for dermatological diseases, focusing on mechanisms of action and clinical results reported in the literature.
In April 2020, we researched the PubMed database for publications covering the use of probiotics in the treatment of atopic dermatitis, acne, psoriasis, rosacea, aging, and melasma. Studies explaining the mechanism of action and clinical trials were prioritized, including original articles and reviews or meta-analyzes regarding the topics covered.
Excessive colonization of pathogenic bacteria on the skin due to epidermal barrier dysfunction and immune deregulation that affects patients characterizes the AD.8 There is a reduction in the microbiome’s diversity,8,9 mainly during episodes of worsening of the disease, 9 in addition to the high colonization by bacteria such as Staphylococcus aureus, which is directly related to the severity of the disease.10 In the same direction, effective treatments were associated with the microbiota’s re-colonization and greater diversity of bacteria.8 Evidence suggests a connection between the disease and microbiota dysbiosis, without a specific invading pathogen, in addition to the already known disorders characteristic of atopic dermatitis, such as filaggrin genes mutations and Th-2 response deregulation.9
Modulation of the intestinal microbiota has emerged as an alternative in treating atopic dermatitis since it is related to the clinical disease’s outcome. A study showed that children with eczema associated with IgE have a lower proportion of bifidobacterium species and less microflora’s diversity during childhood.11 Another study revealed that the early colonization of the intestine by Escherichia coli, during the second month of life, could bring long-term health benefits, since a lower incidence of atopic dermatitis was noticed in colonized patients when they reached six years.12
AD treatment in children using probiotics has been widely studied in recent years. Although the results found may be divergent, a recent meta-analysis showed that intestinal modulation in children could reduce the values of Scoring Atopic Dermatitis (SCORAD).13 Still, information about the effective dose, the best time for administration, and which strains are most effective for the treatment remains unclear.14
A literature review assessed different complementary and integrative therapies (CIT) to treat atopic dermatitis in children.15 The study observed that supplementation of probiotics remains the best CIT validated by studies for the childhood AD treatment.
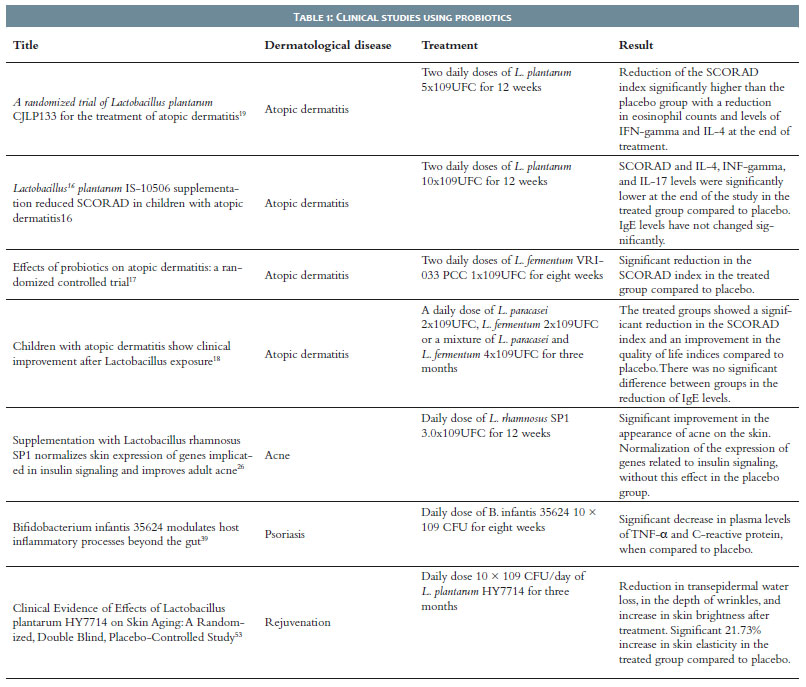
The most robust evidence is related to treatment with Lactobacillus plantarum and Lactobacillus fermentum in children aged 12 months or older. Two different randomized clinical trials evaluated each probiotic, with a duration of 12 months. The studies showed a reduction in SCORAD when administered alone, without other probiotics strains.16-19 The improvement was clinically significant because, on average, an improvement of 8.7 points on the SCORAD scale resulted in an improvement of 1.0 point on the global severity scale. However, although another study on the treatment with L. plantarum has not shown effectiveness.20 Nevertheless, the latter lasted only six weeks while the others lasted 12 weeks, potentially indicating the beneficial effect of longer treatments.
Acne is a dermatological disease related to the pilosebaceous unit. It can manifest itself in an inflammatory form, with papules and pustules, or non-inflammatory, with open or closed comedones. Overproduction of sebum, follicular hyperkeratinization, and increased secretion of pro-inflammatory cytokines characterize the condition.21
Several factors may be related to the onset of the disease. Western carbohydrate diets have a well-established relationship with acne.22 High glucose loads induce insulin and insulin-like growth factor (IGF -1) production, promoting sebocyte and keratinocyte proliferation, and causing the lipids production in the sebaceous glands.23 The Cutibacterium acnes bacteria role in acne’s pathogenesis has been widely studied, although it has not been completely elucidated. Just as the intestinal flora can induce IGF-1,24 it has been shown that C. acnes can stimulate the IGF-1 system/ IGF-1 receptors on the skin.25 Thus, it can be suggested that an imbalance of the intestinal flora may lead to a higher production of sebum and higher colonization of the skin by C. acnes, disturbing the close balance between the skin flora’s members and creating a disease’s synergistic cycle.
Oral supplementation of probiotics can be an adjuvant therapy in acne treatment. A study with humans observed that the consumption of Lactobacillus rhamnosus SP1 3x109 UFC/day improved the acne appearance on the adults’ skin. The therapy could normalize the expression of genes related to insulin signaling, and this change was not seen in the control group.26 Also, a clinical study assessed the synergistic effect of probiotics and minocycline consumption in the treatment of acne compared with the probiotic and antibiotic alone. All groups showed clinical improvement, but the group treated with the association had the lowest number of total lesion, with a significant difference from the other two groups. Also, two patients in the minocycline-treated group had to leave the study because they had vaginal candidiasis, and the probiotic supplementation was an option for possible prevention of adverse events secondary to chronic antibiotic use.27
The use of lactobacilli topically can also be beneficial in reducing acne symptoms. In vitro studies have shown that some probiotics strains can inhibit C. acnes and other non-beneficial species through bacteriocins’ secretion.28 In vitro and in vivo studies with Streptococcus thermophiles demonstrated that the probiotic could increase the production of beneficial lipids in the stratum corneum, such as ceramides, which can retain moisture in the skin,29 and phytosphingosine, which acts against C. acnes.30 Topical probiotics can also act by an immunomodulatory mechanism on keratinocytes and epithelial cells. The Streptococcus salivarius K12 strain was able to inhibit the production of pro-inflammatory cytokines, such as IL-8, in epithelial cells and keratinocytes, most likely by inhibiting the NK-kappa B pathway.31
Psoriasis is an immune-mediated genetic disease that manifests itself in the skin, joints, or nails. It has different clinical manifestation forms, which can be more or less intense, but with typical symptoms such as scaling and plaques on the skin, inflammation, and stiffness of the tissue.32 Although its pathogenesis is not fully understood, Th17 cells and the cytokines produced by them, such as IL-17, IL-22, and IL-23, play critical roles in psoriasis’ pathogenesis. The intestinal microbiome is believed to be involved in the development of psoriasis, as well as in the activation of pro-inflammatory Th17 cells.33 It has been shown that patients with psoriasis and inflammatory bowel disease (IBD), two inflammatory conditions, have a similar pattern of dysbiosis, suggesting the presence of a “gut-microbiome-skin axis” in psoriasis and IBD. The lower presence of symbiotic bacteria, including Lactobacillus spp., Bifidobacterium spp., Faecalibacterium prausnitzii,34 characterize this dysbiosis, as well as the colonization by certain pathobionts, such as Escherichia coli, Salmonella sp., Helicobacter sp., Campylobacter sp., Mycobacterium sp. and Alcaligenes sp.35 Also, S. aureus colonizes more abundantly the skin of psoriasis patients than that of individuals without the disease.36,37 These reduced levels of beneficial bacteria can lead to deleterious consequences, including changes in specific inflammatory proteins and poor regulation of intestinal immune responses that can affect distant organs.
Probiotic supplementation can play a significant role in the treatment of psoriasis. One study showed that oral administration of Lactobacillus pentosus GMNL-77 significantly decreased erythematous lesions and epidermal thickening in mice with imiquimod-induced psoriasis when compared to placebo. The treatment significantly reduced mRNA levels of pro-inflammatory cytokines, including tumor necrosis factor-alpha, interleukin (IL)-6 and IL-23/IL-17A. Also, the study found that treatment with Lactobacillus pentosus GMNL-77 also decreased the spleen weight of the group treated with imiquimod and reduced the number of CD4þ T cells producing IL-17 and IL-22 in the spleen.38
Furthermore, a placebo-controlled study showed that supplementation with Bifidobacterium infantis 35624 in patients with psoriasis led to a significant decrease in plasma levels of pro-inflammatory markers, such as TNF-a and C-reactive protein, when compared to placebo.39 A case study observed that supplementation with Lactobacillus sporogens three times daily combined with 10 mg biotin once daily was able to improve a severe case of pustular psoriasis not responsive to steroids, dapsone, and methotrexate.40
The possibility that intestinal bacteria and their products may contribute to the development of skin lesions, such as rosacea, has also been studied. In a clinical study, it was found that patients with inflammatory skin diseases had an imbalanced intestinal microbiome. Rosacea patients had a significantly higher prevalence of small intestinal bacterial overgrowth (SIBO) than patients without the disease. Also, and more importantly, the SIBO eradication induces an almost complete regression of skin lesions in patients with rosacea.41 In a case study, it was seen that the treatment of a patient affected by rosacea on the scalp with low dose doxycycline and Bifidobacterium breve BR03 together with Lactobacillus salivarius LS01 was able to promote improvement in skin and eye symptoms.42 Although more research in this area are necessary, patients can be counseled on measures to maintain a healthy intestinal microbiome, including consumption of a diet rich in fiber (prebiotics) or modulation of intestinal microflora via oral probiotics.
Ultraviolet radiation (UVR) is considered the most potent inducer of extrinsic aging. Studies have shown that exposure to UVR can induce significant changes in the human immune system, such as reducing the number of Langerhans cells, change in their morphology, and their ability to present antigens.43 Also, an increase in immunosuppressive cytokines like IL-10 has already been reported.44 The use of lactobacilli may represent an alternative skin protection to UVR.
A study with mice demonstrated that supplementation with Lactobacillus johnsonii (La1) was able to protect the skin from the harmful effects of UVR, such as a reduction in the number of Langerhans cells and a higher level of IL-10, post-exposure to radiation.45 A study with humans tested, for ten weeks, the oral administration of Lactobacillus johnsonii and 7.2 mg of carotenoids to healthy women, pre-exposed to simulated or natural sunlight. Compared to placebo, dietary supplementation prevented the UVR-induced decrease in Langerhans cell density and accelerated the recovery of immune system homeostasis after exposure to UVR. The comparison of the minimum erythema dose (MED) showed that, in those who received supplementation, MED increased by 20%.46
The study evidenced the association’s benefit, despite requiring the comparison between treatment with carotenoids and isolated probiotics. Another study also assessed the association of carotenoids and probiotics. A study with humans tested the effectiveness in treating melasma with a supplement containing beta-carotene, lycopene, and Lactobacillus johnsonii. The results showed that the treated group had a significant melasma improvement when it evaluated the Taylor scale and the Melasma Area and Severity Index (MASI) scale.47
A study with hairless mice indicated that oral administration of Bifidobacterium breve prevented URV-induced transepidermal water loss compared to mice that received placebo. Also, the administration of B. breve suppressed the URV-induced increase in hydrogen peroxide levels, protein oxidation, and xanthine oxidase activity in the animals’ skin.48 Another study with mice showed that oral administration of Lactobacillus acidophilus reduced the formation of fine lines induced by exposure to UVB radiation. The study attributed this protection to the reduction in the expression of metalloproteinases, such as MMP-1 and MMP-9.49
The use of probiotics can also benefit other aspects related to skin aging. The use of probiotics can influence intrinsic factors, such as genetics, hormonal status, and oxidative metabolic reactions, and extrinsic factors, such as exposure to solar radiation, tobacco, and psychological stress.
Healthy, normal skin exhibits a slightly acidic pH in the range of 4.2 to 5.6, which helps prevent pathogenic bacterial colonization, regulates enzyme activity, and maintains a moisture-rich environment.50 However, after the age of 70, the skin’s pH increases significantly, stimulating the proteases’ activity.51 As probiotic metabolism frequently produces acidic molecules, decreasing the pH of the environment,52 using probiotics could restore the normal pH of the skin and, consequently, return the levels of proteases’ activity to closer to those observed in young and healthy skin.
A clinical study, controlled by placebo, assessed patients between 41 and 59 years, who had dry skin and wrinkles. The study showed that the administration of 1×1010 CFU/day of Lactobacillus plantarum HY7714 significantly suppressed the loss of transepidermal water, reduced the depth of wrinkles, and increased the skin brightness after three months of treatment compared to day zero. Furthermore, at the end of the study, the group’s skin elasticity treated with probiotics increased by 21.73%, with a significant difference in relation to the placebo group.53 These data suggest that the use of probiotics may work as a nutricosmetic (Table 1).
The balance or imbalance of the human’s microbiome can produce effects in different body organs, such as the skin and the intestine. Various dermatological diseases, usually with inflammatory factors involved, end up responding to the imbalance or modulation of the intestinal microbiota significantly. It occurs mainly due to the suppression or activation of the immune system caused by the modulation of cytokine production and activation of the body’s defense cells, which interferes with the disease’s pathophysiology.
Probiotic supplementation to treat dermatological diseases has been studied for many years. Although it is seen mainly as a complementary therapy in clinical practice, the use of probiotics alone can present a positive result. When combined with conventional therapy, it manages to improve the clinical outcome of the treatment further. Also, its use reduces the adverse events of more aggressive therapies, such as systemic antibiotics. With clear benefits, concrete results have emerged more and more with the growing number of studies on this subject. However, there are still gaps in knowledge and information that need to be better understood, such as the best strains to be used, the effective doses, or best dosing schedule.
Célia Luiza Petersen Vitello Kalil | 0000-0002-1294-547X
Approval of the final version of the manuscript; preparatio0n and writing of the manuscript; critical literature review; critical revision of the manuscript.
Christine Chaves | 0000-0001-8861-6499
Approval of the final version of the manuscript; preparation and writing of the manuscript; critical literature review; critical revision of the manuscript.
Artur Stramari de Vargas | 0000-0001-5773-8039
Approval of the final version of the manuscript; preparation and writing of the manuscript; critical literature review; critical revision of the manuscript.
Valéria Barreto Campos | 0000-0002-3350-8586
pproval of the final version of the manuscript; preparation and writing of the manuscript; critical literature review; critical revision of the manuscript.
1. Szántó M, Dózsa A, Antal D, Szabó K, Kemény L, Bai P. Targeting the gut-skin axis-Probiotics as new tools for skin disorder management? Exp Dermatol. 2019;28(11):1210-8.
2. Health and nutritional properties of probiotics in food including powder milk with live lactic acid : report of a Joint FAO/WHO expert consultation on evaluation of health and nutritional properties of probiotics in food including powder milk with live lactic acid ; Amerian Co\0301rdoba Park Hotel, Co\0301rdoba, Argentina, 1-4 October 2001. [Rome]: FAO/WHO; 2001.
3. Kosiewicz MM, Zirnheld AL, Alard P. Gut microbiota, immunity, and disease: a complex relationship. Front Microbiol. 2011;2:180
4. Weiss GA, Hennet T. Mechanisms and consequences of intestinal dysbiosis. Cell Mol Life Sci. 2017;74(16):2959-77.
5. Teitelman G, Joh TH, Reis DJ. Linkage of the brain-skin-gut axis: islet cells originate from dopaminergic precursors. Peptides. 1981;(2 Suppl 2):157-68.
6. O'Neill CA, Monteleone G, McLaughlin JT, Paus R. The gut-skin axis in health and disease: a paradigm with therapeutic implications. Bioessays. 2016;38(11):1167-76
7. Arck P, Handjiski B, Hagen E, Pincus M, Bruenahl C, Bienenstock J, et al. Is there a 'gut-brain-skin axis'? Exp Dermatol. 2010;19(5):401-5.
8. Petersen EBM, Skov L, Thyssen JP, Jensen P. Role of the gut microbiota in atopic dermatitis: a systematic review. Acta Derm Venereol. 2019;99(1):5-11.
9. Yamazaki Y, Nakamura Y, Núñez G. Role of the microbiota in skin immunity and atopic dermatitis. Allergol Int. 2017;66(4):539-44.
10. Clausen ML, Agner T, Lilje B, Edslev SM, Johannesen TB, Andersen PS. Association of disease severity with skin microbiome and filaggrin gene mutations in adult atopic dermatitis. JAMA Dermatol. 2018;154(3):293-300.
11. Abrahamsson TR, Jakobsson HE, Andersson AF, Björkstén B, Engstrand L, Jenmalm MC. Low diversity of the gut microbiota in infants with atopic eczema. J Allergy Clin Immunol. 2012;129(2):434-40,440.e1-2.
12. Orivuori L, Mustonen K, de Goffau MC, Hakala S, Paasela M, Roduit C, et al. High level of fecal calprotectin at age 2 months as a marker of intestinal inflammation predicts atopic dermatitis and asthma by age 6. Clin Exp Allergy. 2015;45(5):928-39.
13. Huang R, Ning H, Shen M, Li J, Zhang J, Chen X. Probiotics for the treatment of atopic dermatitis in children: a systematic review and meta-analysis of randomized controlled trials. Front Cell Infect Microbiol. 2017;7:392.
14. Yang W, Tu R, Hu Y, He T, Zhang W, Gu L, et al. Probiotics supplement for the prevention of eczema in children: study protocol for a meta-analysis and systematic review. Medicine (Baltimore). 2019;98(34):e16957.
15. Adler-Neal AL, Cline A, Frantz T, Strowd L, Feldman SR, Taylor S. Complementary and integrative therapies for childhood atopic dermatitis. Children (Basel). 2019;6(11):121.
16. Prakoeswa CRS, Herwanto N, Prameswari R, Astari L, Sawitri S, Hidayati AN, et al. Lactobacillus plantarum IS-10506 supplementation reduced SCORAD in children with atopic dermatitis. Benef Microbes. 2017;8(5):833-40.
17. Weston S, Halbert A, Richmond P, Prescott SL. Effects of probiotics on atopic dermatitis: a randomised controlled trial. Arch Dis Child. 2005;90(9):892-7.
18. Wang IJ, Wang JY. Children with atopic dermatitis show clinical improvement after Lactobacillus exposure. Clin Exp Allergy. 2015;45(4):779-87.
19. Han Y, Kim B, Ban J, Lee J, Kim BJ, Choi BS, et al. A randomized trial of Lactobacillus plantarum CJLP133 for the treatment of atopic dermatitis. Pediatr Allergy Immunol. 2012;23(7):667-73.
20. Yang HJ, Min TK, Lee HW, Pyun BY. Efficacy of probiotic therapy on atopic dermatitis in children: a randomized, double-blind, placebo-controlled trial. Allergy Asthma Immunol Res. 2014;6(3):208-15.
21. Bhate K, Williams HC. Epidemiology of acne vulgaris. Br J Dermatol. 2013;168(3):474-85.
22. Melnik BC. Akne und Ernährung. Der Hautarzt. 2013;64(4):252-62.
23. Deplewski D, Rosenfield RL. Role of hormones in pilosebaceous unit development. Endocr Rev. 2000;21(4):363-92.
24. Yan J, Herzog JW, Tsang K, Brennan CA, Bower MA, Garrett WS, et al. Gut microbiota induce IGF-1 and promote bone formation and growth. Proc Natl Acad Sci USA. 2016;113(47):e7554-e63.
25. Isard O, Knol AC, Ariès MF, Nguyen JM, Khammari A, Castex-Rizzi N, et al. Propionibacterium acnes activates the IGF-1/IGF-1R system in the epidermis and induces keratinocyte proliferation. J Invest Dermatol. 2011;131(1):59-66.
26. Fabbrocini G, Bertona M, Picazo Ó, Pareja-Galeano H, Monfrecola G, Emanuele E. Supplementation with Lactobacillus rhamnosus SP1 normalises skin expression of genes implicated in insulin signalling and improves adult acne. Benef Microbes. 2016;7(5):625-30.
27. 27. Jung GW, Tse JE, Guiha I, Rao J. Prospective, randomized, open-label trial comparing the safety, efficacy, and tolerability of an acne treatment regimen with and without a probiotic supplement and minocycline in subjects with mild to moderate acne. J Cutan Med Surg. 2013;17(2):114-22.
28. Bowe WP, Filip JC, DiRienzo JM, Volgina A, Margolis DJ. Inhibition of propionibacterium acnes by bacteriocin-like inhibitory substances (BLIS) produced by Streptococcus salivarius. J Drugs Dermatol. 2006;5(9):868-70.
29. Di Marzio L, Cinque B, De Simone C, Cifone MG. Effect of the lactic acid bacterium Streptococcus thermophilus on ceramide levels in human keratinocytes in vitro and stratum corneum in vivo. J Invest Dermatol. 1999;113(1):98-106.
30. Pavicic T, Wollenweber U, Farwick M, Korting HC. Anti-microbial and -inflammatory activity and efficacy of phytosphingosine: an in vitro and in vivo study addressing acne vulgaris. Int J Cosmet Sci. 2007;29(3):181-90.
31. Cosseau C, Devine DA, Dullaghan E, Gardy JL, Chikatamarla A, Gellatly S, et al. The commensal Streptococcus salivarius K12 downregulates the innate immune responses of human epithelial cells and promotes host-microbe homeostasis. Infect Immun. 2008;76(9):4163-75.
32. Boehncke WH, Schön MP. Psoriasis. Lancet. 2015;386(9997):983-94.
33. Tan L, Zhao S, Zhu W, Wu L, Li J, Shen M, et al. The Akkermansia muciniphila is a gut microbiota signature in psoriasis. Exp Dermatol. 2018;27(2):144-9.
34. Scher JU, Ubeda C, Artacho A, Attur M, Isaac S, Reddy SM, et al. Decreased bacterial diversity characterizes the altered gut microbiota in patients with psoriatic arthritis, resembling dysbiosis in inflammatory bowel disease. Arthritis Rheumatol. 2015;67(1):128-39.
35. Eppinga H, Sperna Weiland CJ, Thio HB, van der Woude CJ, Nijsten TE, Peppelenbosch MP, et al. Similar depletion of protective faecalibacterium prausnitzii in psoriasis and inflammatory bowel disease, but not in hidradenitis suppurativa. J Crohns Colitis. 2016;10(9):1067-75.
36. Ng CY, Huang YH, Chu CF, Wu TC, Liu SH. Risks for Staphylococcus aureus colonization in patients with psoriasis: a systematic review and meta-analysis. Br J Dermatol. 2017;177(4):967-77.
37. Chang HW, Yan D, Singh R, Liu J, Lu X, Ucmak D, et al. Alteration of the cutaneous microbiome in psoriasis and potential role in Th17 polarization. Microbiome. 2018;6(1):154.
38. Chen YH, Wu CS, Chao YH, Lin CC, Tsai HY, Li YR, et al. Lactobacillus pentosus GMNL-77 inhibits skin lesions in imiquimod-induced psoriasis-like mice. J Food Drug Anal. 2017;25(3):559-66.
39. Groeger D, O'Mahony L, Murphy EF, Bourke JF, Dinan TG, Kiely B, et al. Bifidobacterium infantis 35624 modulates host inflammatory processes beyond the gut. Gut Microbes. 2013;4(4):325-39.
40. Vijayashankar M, Raghunath N. Pustular psoriasis responding to Probiotics - a new insight. Our Dermatology Online. 2012;3:326-9.
41. Parodi A, Paolino S, Greco A, Drago F, Mansi C, Rebora A, et al. Small intestinal bacterial overgrowth in rosacea: clinical effectiveness of its eradication. Clin Gastroenterol Hepatol. 2008;6(7):759-64.
42. Fortuna MC, Garelli V, Pranteda G, Romaniello F, Cardone M, Carlesimo M, et al. A case of Scalp Rosacea treated with low dose doxycycline and probiotic therapy and literature review on therapeutic options. Dermatol Ther. 2016;29(4):249-51.
43. Seité S, Zucchi H, Moyal D, Tison S, Compan D, Christiaens F, et al. Alterations in human epidermal Langerhans cells by ultraviolet radiation: quantitative and morphological study. Br J Dermatol. 2003;148(2):291-9.
44. Vink AA, Strickland FM, Bucana C, Cox PA, Roza L, Yarosh DB, et al. Localization of DNA damage and its role in altered antigen-presenting cell function in ultraviolet-irradiated mice. J Exp Med. 1996;183(4):1491-500.
45. Guéniche A, Benyacoub J, Buetler TM, Smola H, Blum S. Supplementation with oral probiotic bacteria maintains cutaneous immune homeostasis after UV exposure. Eur J Dermatol. 2006;16(5):511-7.
46. Bouilly-Gauthier D, Jeannes C, Maubert Y, Duteil L, Queille-Roussel C, Piccardi N, et al. Clinical evidence of benefits of a dietary supplement containing probiotic and carotenoids on ultraviolet-induced skin damage. Br J Dermatol. 2010;163(3):536-43.
47. Fabiana Braga França Wanick FBFW, Beatrix Sabóia Zink BSZ, Raquel Ferreira Lopes RFL. Avaliação da eficácia do licopeno, beta-caroteno e Lactobacillus johnsonii no tratamento de manutenção do melasma durante o verão: um estudo comparativo. Surg Cosmet Dermatol. 2011;3(4):297-301.
48. Ishii Y, Sugimoto S, Izawa N, Sone T, Chiba K, Miyazaki K. Oral administration of Bifidobacterium breve attenuates UV-induced barrier perturbation and oxidative stress in hairless mice skin. Arch Dermatol Res. 2014;306(5):467-73.
49. Im AR, Kim HS, Hyun JW, Chae S. Potential for tyndalized Lactobacillus acidophilus as an effective component in moisturizing skin and anti-wrinkle products. Exp Ther Med. 2016;12(2):759-64.
50. Elias PM, Feingold KR. Skin barrier. New York: Taylor & Francis; 2006.
51. Hachem JP, Crumrine D, Fluhr J, Brown BE, Feingold KR, Elias PM. PH directly regulates epidermal permeability barrier homeostasis, and stratum corneum integrity/cohesion. J Invest Dermatol. 2003;121(2):345-53.
52. Cinque B, Palumbo P, Torre C, Melchiorre E, Corridoni D, Miconi G, et al. Probiotics in aging skin. In: Farage M.A., Miller K.W., Maibach H.I., editors. Textbook of Aging Skin. Berlim: Springer; 2017. p. 811-20.
53. Lee DE, Huh CS, Ra J, Choi ID, Jeong JW, Kim SH, et al. Clinical evidence of effects of lactobacillus plantarum HY7714 on skin aging: a randomized, double blind, placebo-controlled study. J Microbiol Biotechnol. 2015;25(12):2160-8.
 All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773
All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773



 Read in Portuguese
Read in Portuguese
 Portuguese PDF
Portuguese PDF
 Print
Print
 Send this article by email
Send this article by email
 How to cite this article
How to cite this article
 Submit a comment
Submit a comment
 Mendeley
Mendeley
 Pocket
Pocket
{kind=link}