


Ivander Bastazini Junior1; Marina Carrara Camillo Barbosa2
Receipt date: 27/07/2020
Approval date: 29/05/2020
Financial Support: None
Conflict of Interest: None
Study conducted at the Lauro de Souza Lima Institute, Bauru, São Paulo, (SP), Brazil
INTRODUCTION: In the last decades, anticoagulants have become more frequent in the population and younger age groups.
OBJECTIVE: This article aims to address the risk of the most used anticoagulant medications in dermatological surgeries.
METHODS: We reviewed the most common anticoagulant medications.
RESULTS: The pre-surgical consultation performed correctly, emphasizing the patient's clinical history (including renal function in cases of use of new oral anticoagulants), the anatomical site addressed, and the surgical treatment schedule is essential for a satisfactory outcome.
CONCLUSIONS: The use of anticoagulant medications is increasingly common in medical practice. In patients receiving anticoagulant medications, strict adherence to good surgical practices is essential. Special attention to adequate hemostasis of the surgical field, adequate and compressive dressings and postoperative care must be given. The patient should be adequately informed about the most significant risks to which he is subject.
Keywords: Dermatology; Anticoagulants; Surgery
In the last decades, anticoagulant use has become more frequent in the population and younger age groups. This class of drug, which was initially limited to vitamin K inhibitors and acetylsalicylic acid (ASA), grew with the introduction of new antiplatelet agents and new oral anticoagulants (NOAC). These new medications have their pharmacological profile and drug interactions, and they are very different from their predecessors. The dermatological literature on the anticoagulant’s impact on the surgical procedures performed by dermatologists is scarce. Furthermore, the international “guidelines” on anticoagulation are unspecific, considering all procedures as low bleeding risk, which, in the end, can lead to inappropriate conduct in the face of more invasive interventions performed by the dermatological surgeon. This article aims to review of the most used anticoagulant medications and their risks for dermatological surgeries.
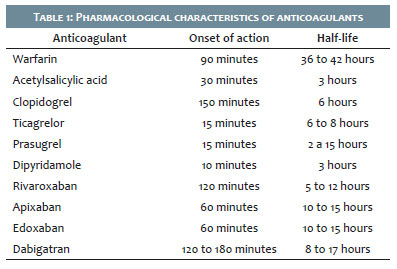
Warfarin is a vitamin K epoxy reductase (VKOR) inhibitor. It starts to act in 90 minutes and has a half-life from 36 to 42 hours (Table 1).1 It has been one of the most widely used anticoagulants for decades. However, due to the narrow therapeutic window and the INR volatility, recent studies showed that only 61% of patients undergoing treatment remained on the desired therapeutic target.2,3 Due to its intense protein binding and metabolism by cytochrome P2C9, many drugs and supplements interfere with its action. Administration of vitamin K or fresh frozen plasma can reverse its effect.
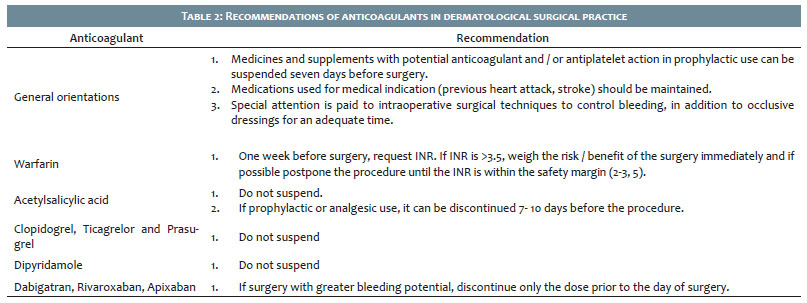
Hemorrhagic events are the most frequent adverse event, and their occurrence is closely linked to INR values, especially when they are higher.4,5 Previous studies suggest that dermatological surgeries can be performed with a lower risk of hemorrhagic complications in patients using warfarin, provided that the INR value is lower3,5 (Table 2), with special attention to intraoperative hemostasis.4 Two other studies assessing patients who underwent surgery with a low bleeding rate using warfarin found a risk of bleeding ranging from 2.28% to 2.5%.5,6
For many years, warfarin suspension and the use of bridging therapies with heparin have been recommended preoperatively. Currently, the literature strongly recommends not using these substitutions for dermatological surgeries due to the increased bleeding risk (9.6% vs. 2.5% while maintaining warfarin) and thromboembolic phenomena.6,7
The acetylsalicylic acid (ASA) is an irreversible inhibitor of cyclooxygenase,1 which hinders platelets from producing thromboxane A2, promoting their aggregation, vasoconstriction, and increased activation.8 It has a rapid onset of action (30-40 minutes) and a short half-life (three hours) (Table 1). The effect is reversible only after platelet renewal. Although some authors have described an increased risk of postoperative bleeding with ASA,9 others found a slight risk (1.42%)6 or did not find increased bleeding when using acetylsalicylic acid and other non-hormonal anti-inflammatory drugs.5,10
Clopidogrel is an irreversible platelet adenosine diphosphate P2Y12 receptor inhibitor, activated after vascular injuries or plaque ruptures. It has an onset of action in two hours and a half-life of six hours.
Drugs metabolized by cytochrome P450 interfere with clopidogrel metabolism by decreasing antiplatelet activity (e.g., proton-pump inhibitors).
Some authors describe a 28-fold increased risk of severe bleeding in patients using clopidogrel compared to non-anticoagulants, and a six-fold increased risk compared to patients using acetylsalicylic acid.9 Studies comparing the association of clopidogrel with other antiplatelet agents (ASA) found an eight-fold increased risk of severe bleeding complications, compared to monotherapy.8 Koenen et al., in a prospective multicenter study with 9,154 surgical procedures, found a bleeding risk of 3.57% in individuals taking two anticoagulants (ASA and clopidogrel); 2.13% for the association of ASA and coumarins; and 1.32% for of ASA combined with heparin. Moreover, those not anticoagulated presented a risk of hemorrhagic complications of 0.55%.11
Ticagrelor is a P2Y12 receptor inhibitor with the onset of action (15-30 minutes) and recovery of platelet function (72 hours) faster than clopidogrel. However, some studies suggest a higher risk of hemorrhagic events (central nervous system and gastrointestinal tract). It presents a 6-8 hour half-life (Table 1).8
Prasugrel is another irreversible platelet receptor P2Y12 inhibitor, also with faster action than clopidogrel. It has an onset of action in 15-30 minutes and a half-life of 2-15 hours (Table 1). Its maximum antiplatelet effect occurs within 48 hours, and recovery occurs gradually after two days of medication suspension.8
Dipyridamole is a phosphodiesterase inhibitor used as a coronary vasodilator. It has an antiplatelet effect due to decreased platelet aggregation and vasodilation. As a single agent, it does not increase the risk of bleeding.8
Rivaroxaban is a direct factor Xa inhibitor, reversibly blocking the conversion of prothrombin to thrombin.12 It has an onset of action between two and four hours and a half-life of 5-12 hours (Table 1). Its elimination is mainly renal.8
It is administered in fixed doses and does not require routine control due to predictable pharmacodynamic and pharmacokinetic characteristics.8
There are no specific laboratory tests for monitoring, but, in emergencies, the activated partial thromboplastin time (APTT) and the prolonged prothrombin time (PT) can be used qualitatively to assess Factor Xa inhibitors.1
It undergoes hepatic metabolism through the cytochrome CYP3A4/5 and CYP2J2 pathways, revealing important drug interactions. Azoles, cyclosporins, and erythromycin increase the anticoagulant effects. Phenytoin and rifampicin have the opposite effect, reducing this action. Also, P glycoprotein (P-gp) inhibitors lead to prolonged and increased anticoagulant action (verapamil, amiodarone, and quinidine) due to the competitive inhibition of renal clearance.12
There is no specific antidote, but prothrombin complex concentrate can be administered in emergencies.1 Two new agents for reversing anticoagulant effects are under investigation (andexanet alfa and ciraparantag), the first of which has already been approved by the Food and Drug Administration (FDA) in May 2018.1,13,14
Apixaban is a direct reversible factor Xa inhibitor, whose mechanism of action is identical to rivaroxaban and edoxaban.1,8 It has fast absorption (1-3 hours) and a half-life of 10 to 15 hours (Table 1). Its excretion is renal (25%) and biliary, and cytochrome P 450/3A4 and enzymatic pathway P-gp metabolizes it. Therefore inhibitors of these pathways increase blood levels of the medication (interactions similar to rivaroxaban).1,8 It also does not require routine monitoring, and patients with mild or moderate renal and hepatic dysfunction do not need dose correction. Andexanet alfa recently obtained authorization as a reverse agent from the FDA.1,13
Edoxaban is the newest direct factor Xa inhibitor.1,12 It has an identical mechanism of action to other factor Xa inhibitors. However, cytochrome P 450 poorly metabolizes it, thus reducing the risk of drug interactions.1,12 Furthermore, medicines that are metabolized by the enzymes of the P-gp system interfere with their effectiveness.
Dabigatran is a direct thrombin inhibitor by constraining factor IIa1 and reversibly blocking the fibrinogen conversion to fibrin.1,8,12 It starts to act in 1-3 hours and has a half-life of 8-17 hours (Table 1). The kidneys excrete it (80%) and, thus, renal dysfunctions can prolong its half-life, being contraindicated in severe renal changes (creatinine clearance <30 ml/min).1,8,12 Cytochrome P does not metabolize it; however, the glycoprotein P (P-gp) inhibitors can raise its plasma levels.
Like other new oral anticoagulants, routine monitoring is unnecessary, but the thrombin time (TT) can be used to infer its effect.1 In emergencies, hemodialysis can be used to reduce its action. More recently, idarucizumab has been approved in Europe as a reversing agent.1,15 Ciraparantag has also been suggested for this purpose.14
The use of anticoagulant medications is increasingly common in medical practice. Consequently, the dermatological surgeon faces daily the need for invasive procedures in patients using one of these medications. In this context, careful preoperative anamnesis focused on daily medications and clinical indications for such use is essential. It’s vital to measure the complexity of the planned procedure, together with the bleeding risk.
There is significant controversy in the literature about the degree of complexity of surgical procedures performed by the dermatologist. However, in general, we must consider those with large detachments and with large tissue movements as procedures with higher bleeding risk. Anatomical location is also directly linked to this risk, with the incidence of bleeding complications in the nose being much more frequent than in other areas of the head and neck region (21% x 6%).16
There are no specific criteria in the dermatological literature on the definition of surgical bleeding. Some authors consider everything from mild events, such as changing the dressing, to severe events, ranging from surgical revision and necrosis to blood transfusion. 11 It can explain different numbers and different interpretations. In general, it is accepted that the risk of bleeding in dermatological surgeries performed on patients who are not using any medication is low, being estimated at approximately 1%.8,11,13 The highest bleeding risk is demonstrated in patients undergoing surgical procedures under the use of anticoagulants.8,11 The literature describes that the association of two or more agents significantly increases hemorrhagic events.8,11,12 However, the increased risk of thromboembolic events associated with discontinuation of anticoagulant medications is well documented.17,18,19 The magnitude of potential events that present high morbidity and mortality dramatically surpasses the risk of hemorrhagic complications at the surgical site in dermatological surgery.
Therefore, the pre-surgical consultation performed properly with an emphasis on the patient's clinical history (including renal function in cases of new oral anticoagulants use), the anatomical location addressed, and the exact surgical schedule treatment is essential for a satisfactory outcome. Whenever feasible, it’s crucial to consider reconstructions with the least possible detachment,18 mainly for complex and riskier areas such as the face. At that time, medications used prophylactically can be discontinued for procedures with higher hemorrhagic potential.
Regarding warfarin, a multicenter study with 9,154 surgical procedures 11 demonstrated the INR value as a significant factor for the bleeding risk in multivariate analysis. In the univariate analysis, the study found that, with a lower INR,1,3 the risk of bleeding was 0.46%; and with a higher INR,1,3 the risk of bleeding increased to 3.7% (p<0.0001).
Syed et al.4 reported a bleeding risk of 60% with INR >3.5 and 27% for INR <3.5. However, the withdrawal of warfarin increases the risk of thromboembolism, in addition to the rebound hypercoagulability state observed when it is interrupted.8 Bridging therapies with heparin are a common practice in moments of warfarin suspension. However, there is an extensive demonstration of increased bleeding events,6,8,20,21 and currently it is not advised in dermatological surgery.22 It is currently considered that INR <3 does not contraindicate the dermatological surgery, even those with more complex reconstructions such as flaps or grafts.8,18,25 If the INR is >3, it is suggested to postpone the surgery until the INR can be within the safety margin.8,18
The use of clopidogrel increases the risk of hemorrhagic events with data ranging from 2.86% to 9%.9 Acetylsalicylic acid increased the risk from 1.42% to 2-3%.8,9 Other authors have not found an increased risk of bleeding with the ASA use compared to controls.5,10 The risk of severe ischemic events and even death with the interruption of these medications is abundant.18,23 Therefore, it is currently recommended not to interrupt medication in patients on antiplatelet monotherapy,5,8,18 except for those with exclusively preventive indication.8 In such cases, they should be suspended seven to 10 days before the surgery date. In cases of a combination of two antiplatelet agents and procedures with a higher bleeding potential, one should evaluate the possibility of operating after the patient is on monotherapy.11 If not possible, the surgical procedure is performed without interrupting the medications.24
Regarding the new oral anticoagulants, we need to consider three main factors in the pre-surgical evaluation: the extent of the surgical procedure, the bleeding risk, and the patient's renal function. The bleeding risk is similar to that of warfarin. Some guidelines, such as the European Heart Rhythm Association (EHRA), consider unnecessary to interrupt NOAC in superficial surgery in patients with normal kidney function (Table 2).12,25 For more aggressive surgeries, it is recommended to interrupt the medication 24 hours before the procedure and not restart it before one hour after the procedure, due to predictability and short half-lives.11,24 In patients with creatinine clearance <30 ml/minute, the medication interruption time should be longer.1
Strict adherence to good surgical practices is essential in patients receiving anticoagulant medications, paying particular attention to adequate hemostasis of the surgical field, proper compressive dressings, and postoperative care. It’s also important to properly inform the patient about the highest risks they are subject to.
Ivander Bastazini Junior| 0000-0003-0300-1263
Statistical analysis; approval of the final version of the manuscript; study design and planning; preparation and writing of the manuscript; data collection, analysis, and interpretation; active participation in research orientation; intellectual participation in propaedeutic and/or therapeutic conduct of studied cases; critical literature review; critical revision of the manuscript.
Marina Carrara Camillo Barbosa | 0000-0001-8906-0242
Statistical analysis; approval of the final version of the manuscript; study design and planning; preparation and writing of the manuscript; data collection, analysis, and interpretation; active participation in research orientation; intellectual participation in propaedeutic and/or therapeutic conduct of studied cases; critical literature review; critical revision of the manuscript.
1. Erdoes G, De Arroyabe BML, Bolliger D, et al. International consensus statement on the peri-operative management of direct oral anticoagulants in cardiac surgery. Anaesthesia 2018;73:1535-45.
2. Mearns ES, Kohn CG, Song JS, et al. Meta-analysis to assess the quality of international normalized ratio control and associated outcomes in venous thromboembolism patients. THhrombosis Research 2014; 134: 310-19.
3. Schein JR, White CM, Nelson WW, et al. Vitamin K antagonista use: evidence of the difficulty of achieve and maintaining target INR range and subsequent consequences. Thrombosis Journal 2016; 14: 14.
4. Syed S, Adams BB, Liao W, et al. A prospective assessment of bleeding and international normalized ratio in warfarin-anticoagulated pacientes having cutaneous surgery. J Am Acad Dermatol 2004; 51: 955-57.
5. Dixon AJ, Dixon MP, Dixon JB. Bleeding complications in skin cancer surgery are associated with warfarin but not aspirin therapy. Br J Surg 2007; 94: 1356-60.
6. Siegal D, Yudin J, Kaatz S, et al. Periprocedural heparina bridging in patients receiving vitamin K antagonists: systematic review and meta-analysis of bleeding and thromboembolic rates. Circulation 2012; 126: 1630-39.
7. Nast A, Ernst H, Rosumeck S, et al. Risk of complications due to anticoagulation during dermatosurgical procedures: a sytematic review and meta-analysis. J Eur Acad Dermatol Venereol 2014: 28: 1603-09.
8. Brown DG, Wilkerson EC, Love WE. A review of traditional and novel oral anticoagulante and antiplatelet therapy fos dermatologists and dermatologic surgeons. J Am Acad Dermatol 2015;72:254-34.
9. Cook-Norris RH, Michaels JD, Weaver AL, et al. Complications of cutaneous surgery in patients taking clopidogrel containing anticoagulation. J Am Acad Dermatol 2011; 65:584-91.
10. Billingsley EM, Maloney ME. Intraoperative and postoperative bleeding problem in patients taking warfarin, aspirin and nonsteroiddal antiinflammatory agentes. A prospective study. Dermatolol Surg 1997; 23: 381-83; discussion 385-85.
11. Koenen W, Kunte C, Hartmann D, et al. Prospective multicentre cohort study on 9154 surgical procedures to assess the risk of postoperative bleeding - a DESSI study. J Eur Acad Dermatol Venereol 2017;31:724-31.
12. Munson CF, Reid AJ. Novel oral antocoagulants in plastic surgery. J Plast Reconstr Aesthet Surg. 2016;69(5):585-93.
13. Siegal DM, Curntte JT, Connolly SJ, et al. Andexanet alfa for the reversal of fator Xa inhibitor activity. N engl J Med. 2015;373:2413-24.
14. Ansell JE. Universal, class-specific and drug-specific reversal agentes for the new oral anticoagulants. J Thromb thrombolysis. 2016;41:248-52.
15. Pollack CV Jr, Reilly PA, Eikelboom J, et al. Idarucizumb for dabigatran reversal. N Engl J Med. 2015;373:511-20.
16. Eichhorn W, Barsukov E, Al-Dam A, et al. POstoperative bleeding risk for cutaneous surgery in the head and neck regiion with continued phenprocoumon therapy. J Craniomaxillofac Surg.2014;42:608-11.
17. Kovich O, Otley CC. Thrombotic complications related to discontinuation of warfarin and aspirin therapy perioperatively for cutaneous operation. J Am Acad Dermatol.2003;48:233-7.
18. Amici JM. Don"t stop antithrombotics for cutaneous surgery: just do it now! Br J Dermatol.2015;172:555-56.
19. Amici JM, Rogues AM, Lasheras A, et al. A Prospective study of the incidence of complications associated with dermatological surgery. Br J Dermatol. 2005;153:967-71.
20. Birnie DH, Healey JS, Wells GA, et al. Pacemaker or defibrillator surgery without interruption of anticoagulation. N Engl J Med. 2013;368:2084-93.
21. Di Biase L, Burkhardt JD, Santangeli P, et al. Periprocedural stroke and bleeding complications in patients undergoing cateter ablation of atrial fibrillation with diffrent anticoagulation management: results from the Role of Coumadin in preventing thromboembolism in atrial fibrillation patients unbdergoing cateter ablation ramdomized trial. Circulation. 2014;129:2638-44.
22. Eisenstein DH. Anticoagulation management in the ambulatory surgical setting. AORN J. 2012;95:510-21.
23. Mayer K, Bernlochner I, Braun S, et al. Aspirin treatment and outcomes after percutaneous coronary interventions: results of the ISAR-ASPI Registry. J Am Coll Cardiol. 2014;64:863-71.
24. Sporbeck B, Georges Bechara F, Hafner HM, et al. S3 guidelines for the management of anticoagulation in cutaneous surgery. J Dtsch Dermatol Ges. 2015;13:346-56.
25. Doherty JU, Gluckman TJ, Hucker WJ, et al. 2017 ACC expert consensus decision pathway for periprocedural management of anticoagulation in patients with nonvalvular atrial fibrillation: a reporto f the american college of cardiology clinical expert consensus document task force. J Am Coll Cardiol. 2017;69:871-98.
 All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773
All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773



 Read in Portuguese
Read in Portuguese
 Portuguese PDF
Portuguese PDF
 Print
Print
 Send this article by email
Send this article by email
 How to cite this article
How to cite this article
 Submit a comment
Submit a comment
 Mendeley
Mendeley
 Pocket
Pocket
{kind=link}
{kind=link}