


Pitila Ramalhoto1; Bianca Viscomi2; Carla de Sanctis Pecora2; Suyan Vasconcelos3; Rossana Vasconcelos4; Nicoli Oliveira5; Carlos David Araújo Bichara6; Ada Trindade de Almeida7
Received on: 25/05/2020
Approved on: 30/05/2020
Financial support: None
Conflict of interest: None
Research performed at private clinics and Dermatology Services in the states of de Janeiro, de São Paulo e de Sergipe, Brazil
The COVID-19 pandemic represents an unprecedented healthy global threat, leading dermatologist surgeons/aestheticians to interrupt or alter clinical practice and adjust to the necessary precautionary methods. This article aims to prepare dermatologists for the upcoming difficulties and precautions for conducting procedures in the midst of coronavirus pandemics, focusing on recommendations and best practices for reopening aesthetic practice while mitigating risks to practitioners, patients, staff, and the general public.
Keywords: COVID-19; Dermatology; Pandemic; Physicians’ office, SARS-CoV-2.
The novel coronavirus (SARS-CoV-2) was first identified in Wuhan, China, in December 2019.1 In March 2020, COVID-19, caused by the novel coronavirus, was officially declared a pandemic by the World Health Organization (WHO), representing an unprecedented global health crisis.2
The main transmission route is via respiratory secretions (aerosols or direct contact). Symptoms can appear two to 14 days after exposure, with an incubation period of four to seven days. The symptoms are fever (98%), anosmia (80%), cough (76%), dyspnea (50%), and myalgia or fatigue (44%), but many patients can be asymptomatic and still transmit the infection.3
Dermatology practice includes clinical, surgical, and cosmetic care. Assuming that aesthetic procedures are considered non-essential and non-emergency, it is imperative to prepare adequately for safe practice in dermatology.3,4
To discuss the safest approach to dermatology practice in this new scenario, a group of Brazilian dermatologists developed a set of safety guidelines for outpatient care based on the guidelines issued by official bodies such as the Brazilian National Health Surveillance Agency (ANVISA) and WHO, as well as scientific publications.5,6
Since asymptomatic individuals can transmit the virus, preparation of the clinical setting must be done carefully, considering every patient as a possible COVID-19 carrier.
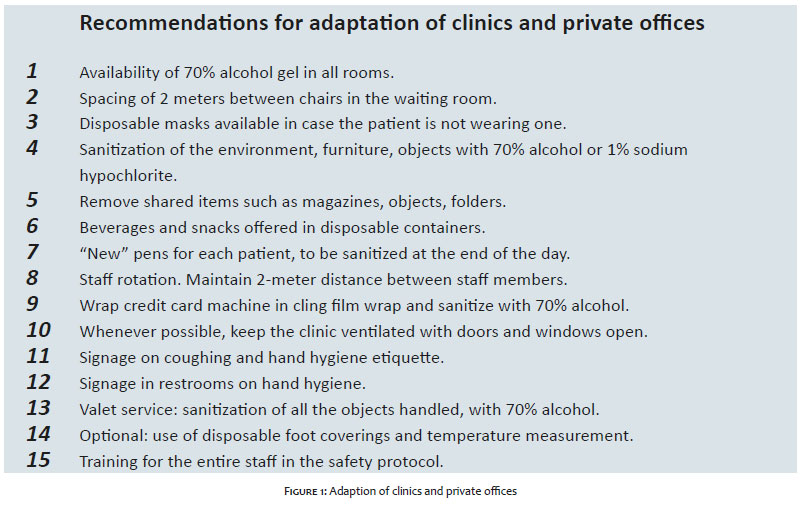
The following measures are essential (Figure 1)1,5,6,7
70% alcohol gel: dispensers at the clinic’s entrance and in all the rooms, allowing easy hand sanitization.
Social distancing: the clinic or office should be prepared to maintain a minimum distance of 1.5 to 2m between persons. Removing or blocking off seats, marks on the floor, and acrylic barriers are some options for implementing this measure.
Disposable masks: all patients should be instructed to appear for their appointments wearing masks. If a patient comes without a mask, one should be provided at the clinic’s entrance and only removed when so requested by the physician.
Sanitization of the environment: staff should be trained in the clinic’s correct sanitization and disinfection processes. The clinic should be cleaned at the beginning and end of the day. Shared areas such as restrooms and consultation and procedure rooms should be cleaned before and after use by each patient. Some methods and substances can be used, such as ultraviolet light, 70% alcohol, sodium hypochlorite solution, and commercial solutions containing these substances.
Removal of shared materials: all material with shared use, such as magazines, newspapers, and pamphlets should be removed from the reception area. Beverages should be served in disposable containers. Pens should be discarded in a recipient for subsequent sanitization, and offered already sanitized.
Decrease the circulation of persons: encouraged by staff rotation, restriction of accompanying persons, and adjustments to appointment scheduling. The authors’ suggestion is a minimum 40-minute interval between consultations, which can be longer in case of aesthetic and surgical procedures.
Ventilated and airy rooms: windows and doors should remain open to disperse suspended viral particles. Whenever possible, rotate consultation rooms to facilitate cleaning.
Signage: orientation on coughing etiquette, hand hygiene, and physical distancing.
Disposable foot coverings and temperature measurement: Before patients enter the clinic, their temperature can be taken and they can be offered disposable foot coverings.
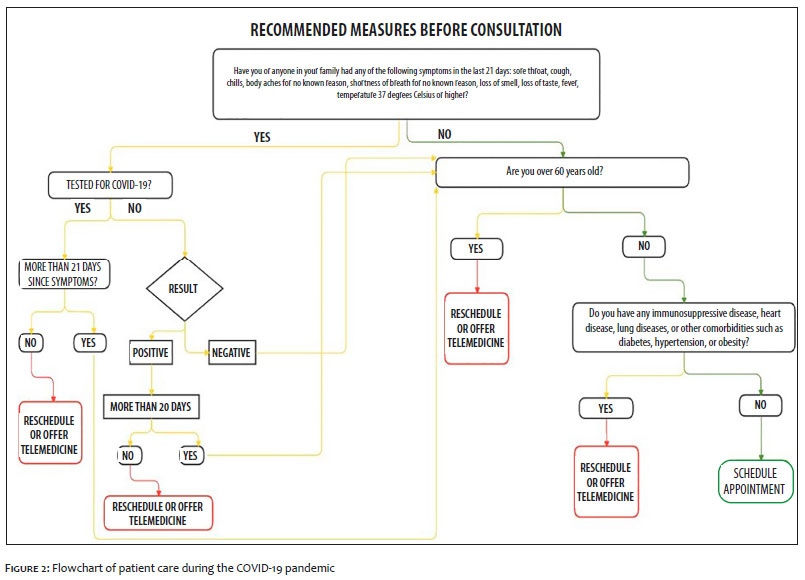
It is essential to adopt clear and transparent communication between the clinic and the patient. With resumption of activities during COVID-19, this will facilitate triage of individuals who are fit to appear at the clinic. It will also create an atmosphere of trust, demonstrating the entire staff’s concern in maintaining the clinic as safe as possible,7 according to the flowchart of care in Figure 2.
Telemedicine should be promoted for medical consultations, definition of treatment protocols, and other clarifications.1,7,8 This will help reduce patient flow, time in the clinic, and risk of infection on route.
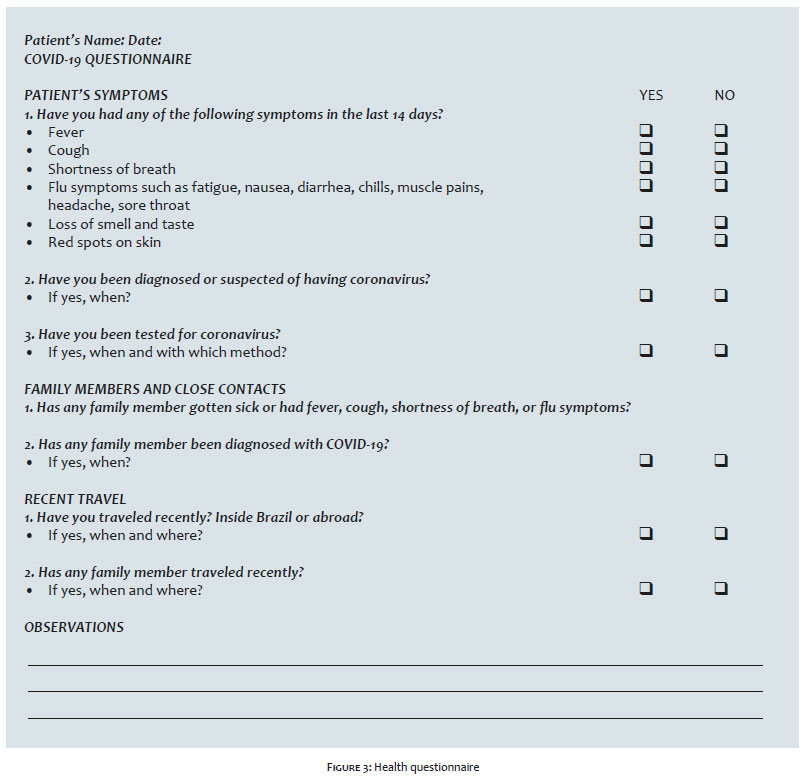
If face-to-face consultation is necessary, the patient should answer a questionnaire in advance on risk situations and COVID-19 symptoms, described in Figure 3.7,8 In case of any symptom, the appointment should be postponed by at least 20 days.
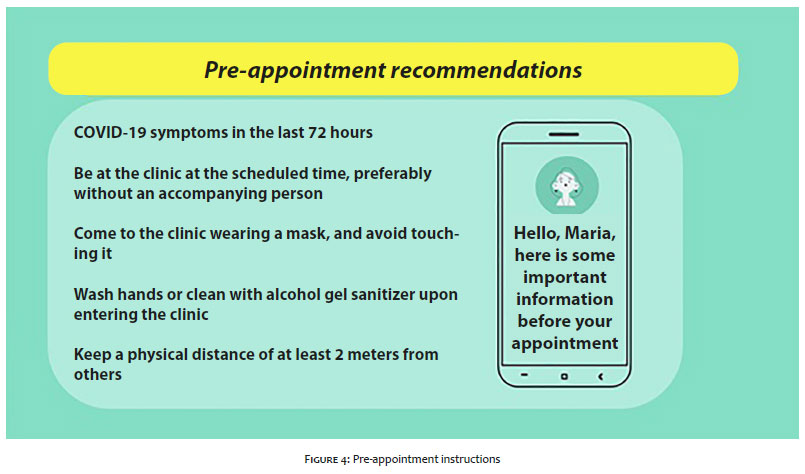
If the individual is fit for a face-to-face consultation, a second contact should be made a day in advance, investigating the appearance of COVID19 symptoms in the patient or family members. If no such symptoms are reported, the person should receive a text message or e-mail with safety instruction, as described in Figure 4.
For patients at high risk for complications of COVID-19, such as the elderly, immunocompromised individuals, and those with cardiac or pulmonary diseases or other comorbidities such as diabetes, hypertension, or obesity, the postponement of non-essential procedures should be considered.7
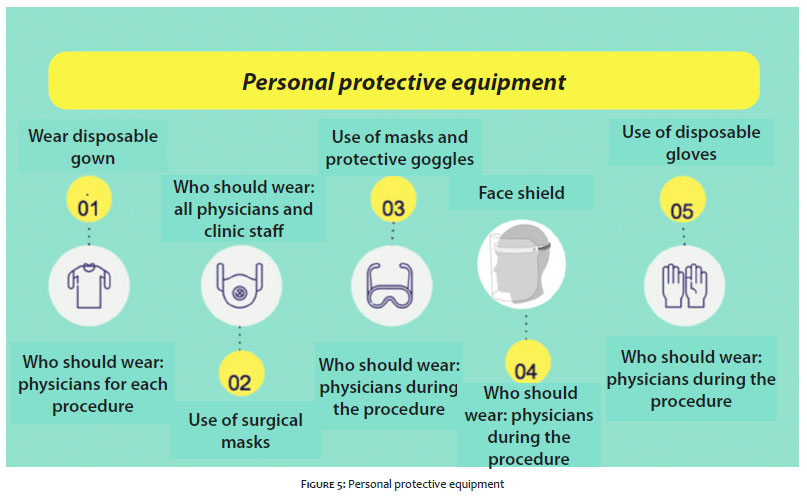
The Brazilian Society of Infectious Diseases recommends wearing a surgical mask while the professional is inside the office, clinic, or hospital, changing the mask regularly. The World Health Organization (WHO) recommends N95 masks. Cloth masks should not be used by health professionals, including physicians and clinical staff, and their use is only allowed for patients (Figure 5).9
During the physical examination or procedure, a disposable gown should be worn, changed after each patient. In situations involving proximity to the patient’s face, the recommendation is to wear an N95 mask and protective goggles or face shield.3 Gloves are only necessary during procedures.3
Recommendations during patient care
Whenever possible, the care should be performed with the windows open to optimize air circulation. The air conditioner may or may not remain on. While taking the patient history, the physician and patient should both be wearing masks.10
Hand washing/sanitization is recommended before and after contact with the patient, and the face should not be touched with contaminated hands.
Hands should be washed with soap and water or cleaned with 70% alcohol, which are capable of dissolving the lipid membrane of the virus and inactivate it.3,10,11 If soap and water are used, hands should be washed for approximately one minute. When 70% alcohol gel is used, the hand hygiene should last approximately 20 seconds.
The exam table should be covered with disposable sheets, which should be removed and discarded after use by each patient, always maintaining proper care to avoid self-contamination. All the equipment and instruments that may have been used in direct contact with the patient should be sanitized with 70% alcohol.3,11
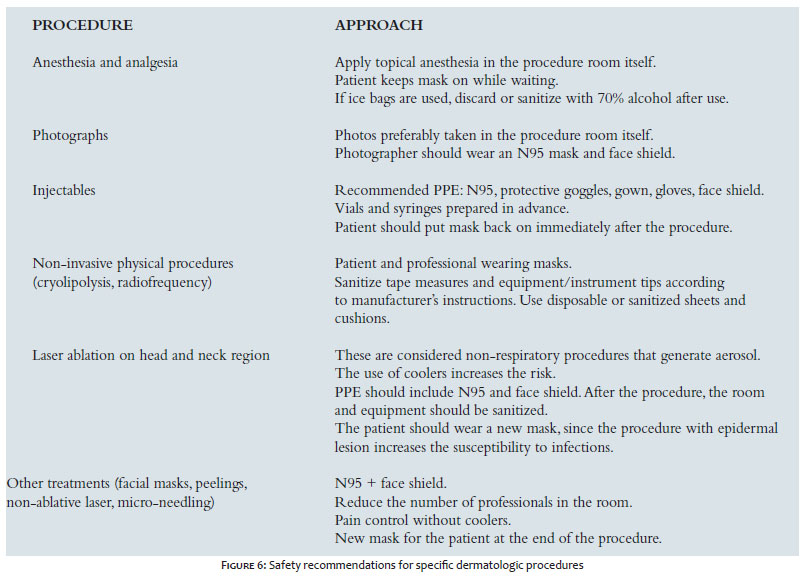
During physical examination, the patient’s mask may be removed to examine the face and oral mucosa.10 Since there is risk of transmission via droplets at this moment, we suggest the use of protective goggles or a face shield, besides an N95 surgical mask, to increase protection.5,6,10 Figure 6 includes safety recommendations for specific dermatologic procedures.
After each consultation, all the surfaces touched by the patient or accompanying person should be sanitized with 70% alcohol or 1% sodium hypochlorite, including the exam table, chair, scale, sphygmomanometer, thermometer, etc. 3,10,11
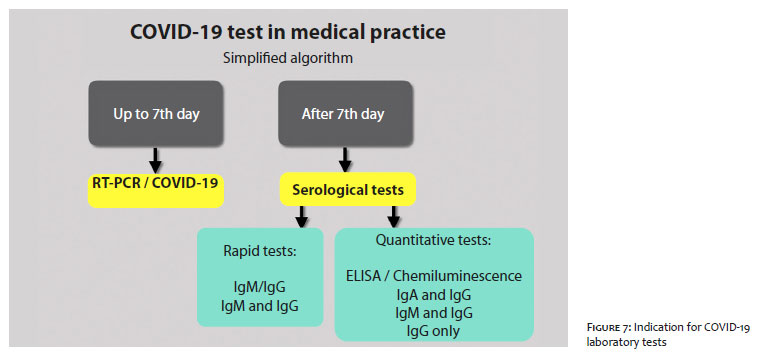
COVID-19 tests can be classified as follows:
Test for the virus: RT-PCR/COVID-19.
Antibody or serological tests: for detection of IgM, IgA, IgG, which can be performed by various methods, such as ELISA, chemo fluorescence, and immunofluorescence.
In medical practice, thus far there is no consensus on the testing protocol for COVID-19.12
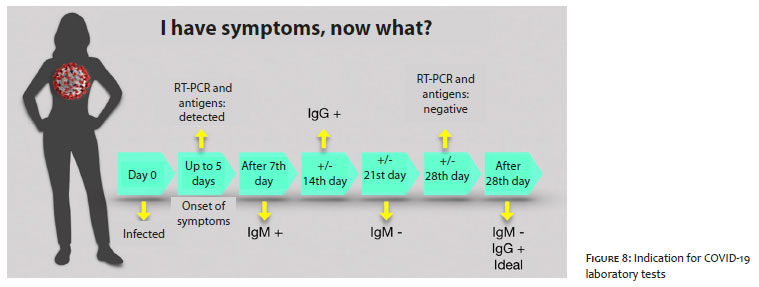
A positive test is highly suggestive of COVID-19, while a negative test does not rule out the disease. Patients and health professionals should assume they have the disease if they have signs or symptoms, even if they test negative.13
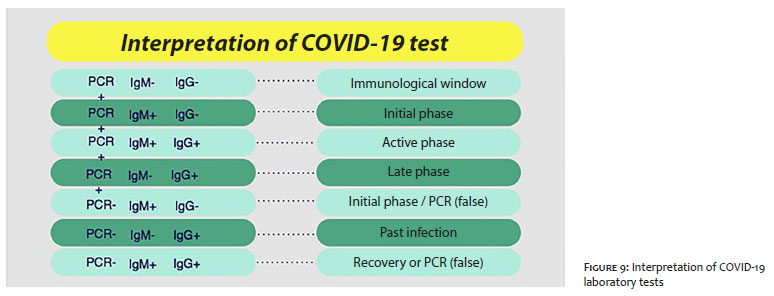
Indication for COVID-19 testing should follow figures 7 and 8, while Figure 9 shows the lab tests’ interpretation.
The COVID-19 pandemic has raised unimaginable challenges.14-16 Constant discovery of new information means that health professionals face the additional challenge of keeping up-to-date with the best practices.
Adaptations must be made to mitigate risks and guaranguarantee safety for the patient and all professionals involved.
Pitila Ramalhoto | 0000-0002-4359-7607
Contribution to the article: Approval of the final version; conception and planning of the study; elaboration and writing of the manuscript; data collection, analysis, and interpretation; critical review of the literature.
Bianca Viscomi | 0000-0001-9909-258X
Contribution to the article: Approval of the final version; conception and planning of the study; elaboration and writing of the manuscript; data collection, analysis, and interpretation; critical review of the literature.
Carla de Sanctis Pecora | 0000-0002-0711-281X
Contribution to the article: Approval of the final version; conception and planning of the study; elaboration and writing of the manuscript; data collection, analysis, and interpretation; critical review of the literature.
Suyan Vasconcelos | 0000-0003-3109-8613
Contribution to the article: Approval of the final version; conception and planning of the study; elaboration and writing of the manuscript; data collection, analysis, and interpretation; critical review of the literature.
Rossana Vasconcelos | 0000-0002-6185-1840.
Contribution to the article: Approval of the final version; conception and planning of the study; elaboration and writing of the manuscript; data collection, analysis, and interpretation; critical review of the literature.
Nicoli Oliveira | 0000-0001-6540-0898.
Contribution to the article: Approval of the final version; conception and planning of the study; elaboration and writing of the manuscript; data collection, analysis, and interpretation; critical review of the literature.
Carlos David Araújo Bichara | 0000-0002-7107-3640.
Contribution to the article: Data collection, analysis, and interpretation; critical review of the literature.
Ada Trindade de Almeida | 0000-0002-4054-2344
Contribution to the article: Approval of the final version; conception and planning of the study; elaboration and writing of the manuscript; data collection, analysis, and interpretation; critical review of the literature.
1. Kaye K, Paprottka F, Escudero R, Casabona G, Montes J, Fakin R, et al. Elective, non-urgent, procedures and aesthetic surgery in the wake of SARS–COVID-19: considerations regarding safety, feasibility and impact on clinical management. Aesthetic Plast Surg. 2020 14:1-29.
2. Al-Benna S. Availability of COVID-19 information from national and international aesthetic surgery society websites. Aesth Plast Surg. 2020;12:1-4.
3. Jindal A, Noronha M, Mysore V. Dermatological procedures amidst COVID-19: when and how to resume. Dermatol Ther. 2020;12:e13561.
4. Kapoor KM, Chatrath VC; Boxley SG; Nurlin I, Snozzi P, Demosthenes N, et al. COVID-19 Pandemic: consensus guidelines for preferred practices in an aesthetic clinic. Dermatologic Therapy. Epub 2020 May 16.
5. Anvisa [Internet]. Orientações para serviços de saúde: medidas de prevenção e controle que devem ser adotadas durante a assistência aos casos suspeitos ou confirmados de infecção pelo novo coronavírus (Sars-Cov-2). 2020. [cited 2020 Maio 8]. Available from: http://www.portal.anvisa.gov.br
6. WHO [Internet]. Novel Coronavirus (COVID-19) Dashboard. [acessed 2020 jun 7]. Available from: https://www.who.int/.
7. Dover JS, Moran ML, Figueroa JF, Furnas H, Vyas JM, Wiviott LD, et al. A path to resume aesthetic care: executive summary of project AesCert guidance supplement-practical considerations for aesthetic medicine professionals supporting clinic preparedness in response to the SARS-CoV-2 outbreak. Facial Plast Surg Aesthet Med. 2020;22(3):125-151.
8. Euclides Cavalcanti. COVID-19: a physician practice guide to reopening. In.: American Medical Association [Internet]. 2020. [cited 2020 May 21]. Available from: https://www.ama-assn.org/delivering-care/public-health/covid-19-physician-practice-guide-reopening
9. Weissmann L, Cunha AC, Chebabo A, Michelin L, Bandeira ACA, Domingos de Oliveira PR, et al. Nota de esclarecimento (Uso de máscaras na pandemia de COVID-19) [Cited 2020 Apr 2]. In.: Sociedade Brasileira de Infectologia [Internet]. Available from: https://www.infectologia.org.br/
10. Recomendações de Cuidados para Consultórios Médicos do Hospital Sírio-Libanês. https://www.hospitalsiriolibanes.org.br. Abr 2020.
11. Türsen Ü, Türsen B, Lotti T. Coronavirus-days in dermatology. Dermatol Ther. 2020:e13438.
12. Bachelet V. Do we know the diagnostic properties of the tests used in COVID-19? A rapid review of recently published literature Medwave 2020;20(3):e7891
13. Beeching NJ, Fletcher TE, Beadsworth MBJ. COVID-19: testing times. BMJ 2020;369:m1403
14. David Bichara. COVID-19: marcadores sorológicos. Goiás: PUC; 2020.
15. Sociedade Brasileira de Dermatologia [Internet]. Orientações da Sociedade Brasileira de Dermatologia sobre o uso de equipamentos de proteção individual (EPIs) aos profissionais da área da saúde [cited 2020 Apr 21]. Available from: https://www.sbd.org.br
16. Anvisa [Internet]. Protocolo de manejo clínico do novo coronavírus (COVID-19) na atenção primária à saúde [cited 2020 May 4]. Available from: https://portalarquivos2.saude.gov.br
 All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773
All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773



 Read in Portuguese
Read in Portuguese
 Portuguese PDF
Portuguese PDF
 Print
Print
 Send this article by email
Send this article by email
 How to cite this article
How to cite this article
 Submit a comment
Submit a comment
 Mendeley
Mendeley
 Pocket
Pocket
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}