


Flávia Alvim Sant’anna Addor1; Sandro Caballero Barbosa2
Received on: 06/12/2019
Approved on: 29/05/2020
Financial support: Glenmark provided the samples and financial support for the development of the study
Conflict of interest: Glenmark's medical manager participated in the review of the protocol and the final text
Study conducted on MEDCIN Research, Osasco (SP), Brazil
INTRODUCTION: Seborrheic dermatitis is a chronic inflammatory disease in areas with a higher concentration of sebaceous glands and the participation of the fungi of the genus Malassezia sp.
OBJECTIVE: To assess the effectiveness of treating moderate to severe seborrheic dermatitis using two shampoo formulations in monotherapy.
METHODS: Patients with moderate to severe seborrheic dermatitis of the scalp, with or without chemically processed hair, were grouped according to the degree of affection and used one of two versions of shampoo monotherapy for four weeks. Relapse after treatment cessation was also evaluated.
RESULTS: There was a significant reduction (p <0.05) of oiliness since the first application. The other signs (erythema and peeling) showed significant improvement for both treatments. Participants also reported a considerable improvement in pruritus, erythema, and peeling. The effect on the hair strands was considered positive with both procedures. After one week of suspension, the relapse rate was considered non-significant (p <0.05).
CONCLUSIONS: Both versions of shampoos were able to promote effective control of moderate to severe seborrheic dermatitis. These formulations also demonstrated not to harm the hair strands, even when chemically processed, a fundamental fact to treatment adherence.
Keywords: Dermatitis Seborrheic; Inflammation; Keratolytic Agents; Malassezia; Sebum
Seborrheic dermatitis (DS) is a chronic superficial inflammatory disease of the skin characterized by erythematous-scaly, itchy areas over areas with a higher concentration of sebaceous glands, such as scalp, face, and ears.1 Its prevalence in the general population is estimated between 3% and 10%, being more frequent in men.2
The scalp is the most frequently affected area, where dry pityriasis desquamation, a condition known as dandruff, is the most common manifestation. Although it is a benign condition, it is a frequent cause of embarrassment, especially when accompanied by other signs of seborrheic dermatitis, such as pruritus and erythema, as it is a visible area.3
Seborrheic dermatitis has an unknown etiology and pathogenesis.1 Nevertheless, it is known as a multifactorial condition that can include environmental factors, such as humidity and solar radiation variation, and lifestyle factors, such as emotional stress and food.2 It is also known that there is a participation of fungi of the genus Malassezia sp., especially the species Malassezia globosa and Malassezia restrita. They cause an inflammatory reaction that appears to be mediated by free fatty acids released from sebaceous triglycerides by fungal enzymes, such as lipases. The Malassezia lipid layer can also modulate the production of pro-inflammatory cytokines by keratinocytes.2
The treatments available for the control of seborrheic dermatitis of the scalp can have antifungal, keratolytic, or anti-inflammatory action. Most of the commercialized treatments contain some active antifungal against Malassezia. Zinc pyrithionate also acts as an antifungal and seborregulator, and salicylic acid has keratolytic action. Topical corticosteroids are also used for their anti-inflammatory action.4
Although seborrheic dermatitis of the scalp can vary in intensity, the first step in therapy, regardless of severity, is adopting an appropriate shampoo, capable of removing excess oil and peeling, and controlling fungal proliferation. Many actives principles have been used for this purpose, usually in association. Among the most studied, are antifungals, such as ciclopirox olamine, and zinc pyrithione,4,5 and keratolytics, such as salicylic acid.5,6,7
However, the shampoo effectiveness depends on the adherence, which, in turn, can be affected if it impairs the appearance of the hair, especially in women. The occurrence of long and processed hair (dyed, straightened) is a reality in our country, and when choosing a shampoo, this question must be considered. In other words, the surfactant (cleaning) system, as well as the introduction of active principles that control inflammation and repair or protect the hair strands, greatly assist treatment adherence. Shampoos with these characteristics promote the control of SD per se and even favor the reduction of other topical drugs, such as corticosteroids.5
Another expected action of shampoo for seborrheic dermatitis is the control of relapses. It should not irritate or dry out the scalp too much, preventing the rebound effect when the use of the product is interrupted.
This study aimed to assess two new formulations of shampoos to control seborrheic dermatitis with differentiated vehicles, in which the anti-inflammatory and antifungal actions are associated with the innovative proposal to prevent capillary damage and recurrences while still maintaining an optimal profile of efficacy and tolerability from the first application.
This is a prospective, randomized, blind study conducted at a Private Clinical Research Center (MEDCIN Research, MEDCIN Group - Osasco, SP). An independent ethics committee approved the study protocol (CAAE: 08031319.0.0000.5514 and 08033219.2.0000.5514), including the free and informed consent form.
We invited 133 patients of both sexes, between 18 and 60 years old, with clinical features of seborrheic dermatitis of the scalp classified as moderate to severe, without treatments for three months after inclusion. Patients using anti-inflammatories, immunosuppressants, antifungals, and antibiotics were excluded, as well as pregnant women and lactating mothers.
The determination of the degree of seborrheic dermatitis in patients was made based on a clinical evaluation by a dermatologist, using the classification Adherent Scalp Flaking Score (ASFS)8 in which: 0 = no flaking, 2 = very mild flaking, 4 = mild flaking, 6 = moderate flaking, 8 = severe flaking, and 10 = very severe flaking. Only those with grades above 6 were included. Erythema intensity (absent/ mild/moderate/intense) and symptoms of pruritus (absent/ mild/moderate/intense) were also evaluated.
From this inclusion, they were grouped, according to the peeling score, in two groups: Group 1, with score 06, to use Shampoo 1 in monotherapy (Celamina Zinco®), and Group 2, with scores 8-10, to use Shampoo 2 in monotherapy (Celamaina Ultra®).
Within both groups, patients were also included, in a balanced way, according to their type of hair:
• Hair subjected to straightening;
• Hair subjected to dye;
• Unprocessed blond hair (virgin);
• Hair not fitting fit the above criteria (other shades, including white, without processing, etc.).
This measure aimed to make each group represent more reliably the varieties of hair processing and textures that we currently find, mainly in women.
All were instructed not to wash their hair for two days and attend the Center on the third day, for the following evaluations.
Oil reduction after the first application
The patients of both groups were acclimated for the collection of sebumetric measurements, with Sebumeter® SM 815 equipment (Courage & Khazaka), which measures the sebum content on the capillary surface, in previously standardized areas: right and left frontoparietal region. Then, each half-head was washed randomly: one side with the treatment product of its respective group (Celamina Zinco® and Celamina Ultra®), and the control frontoparietal region with no application of cleaning agents, being washed only with water.
After washing, the hair dried naturally, and subsequent measurements were taken in the treated area and in control area at 2, 3, 4, 6, and 8 hours after the single application.
For assessment of Celamina Ultra® and Celamina Zinco® shampoos effect over time, participants were instructed to use the products in their homes, using them to wash their hair twice a week. The method of use was oriented as described: apply the shampoo to wet hair, massaging the scalp until obtaining an abundant foam, then wait for it to act for five minutes and rinse.
Reduction of scaling under conditions of use
For assessment of the shampoo's effect in terms of scaling reduction, on the first visit, before washing the hair at the Center, patients were referred for standardized scalp scaling collection. This collection was performed with a standardized comb, passed through the hair of the frontoparietal area 10 times in a row. This material was collected in a standardized dark plate and photographed (Canon T3i digital camera), also in a standardized way, for image analysis (Image software Pro®) of the scale area.
This procedure was repeated 24 hours after the first use of the product and two and four weeks after the start of use of shampoos.
Reduction of pruritus and erythema under conditions of use
Patients in both study groups were asked to answer a questionnaire about pruritus. They were assessed for investigation of adverse events within 24 hours, two weeks, and four weeks after the start of the study.
Cosmetic effect on the hair
Patients in both study groups were asked to answer a questionnaire about the effects of using shampoos in monotherapy, considering their cosmetic effects on the hair strands (shine, combability, and other hair qualities). This questionnaire was applied after the first washing with the products and was repeated four weeks after continuous use.
Relapse prevention
After four weeks of use and data collection, the patient received a neutral shampoo sample and was instructed not to use any other product for a week. Patients returned at the end of this period, performing a new clinical, sebumetric evaluation, and photographic record of the scaling, in the same previous models, to assess a possible relapse.
Of the 133 recruited patients, 96 were selected according to the inclusion and exclusion criteria, entering group 1 or group 2, according to the intensity of seborrheic dermatitis (score). Group 1 started with 48 patients and ended with 44 patients; four were discontinued for reasons unrelated to the study (violation of the protocol, failure to attend evaluations), and their data were not considered. Group 2 also started with 48 patients, ending with 47. In this group, only one patient had his data excluded due to violation of the protocol. The mean age was 42.4 years for group 1 and 48 years for group 2. Regarding gender, the study was completed with 76% of female patients and 24% of male patients in both groups.
No patient, in both groups, reported worsening of the condition or other adverse events, related or not to the use of the products, throughout the study.
Effectiveness assessment
Step 1: Immediate effect
Oil reduction after the first application
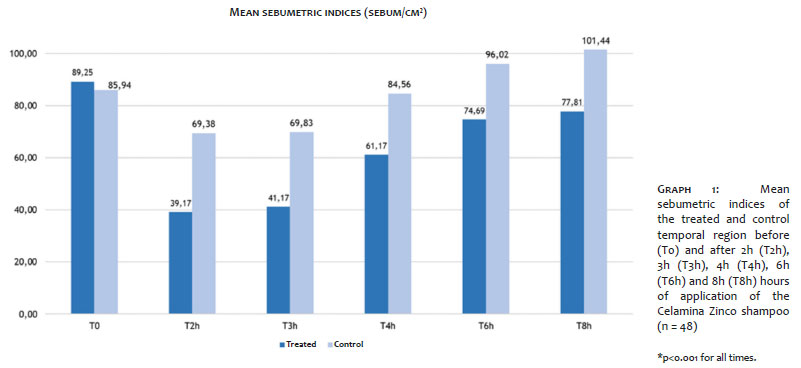
Group 1: Celamina Zinco® (moderate SD)
As shown in graph 01, there was a significant reduction in sebumetry at all times of assessment, statistically significant (p<0.001) when compared to the control area.
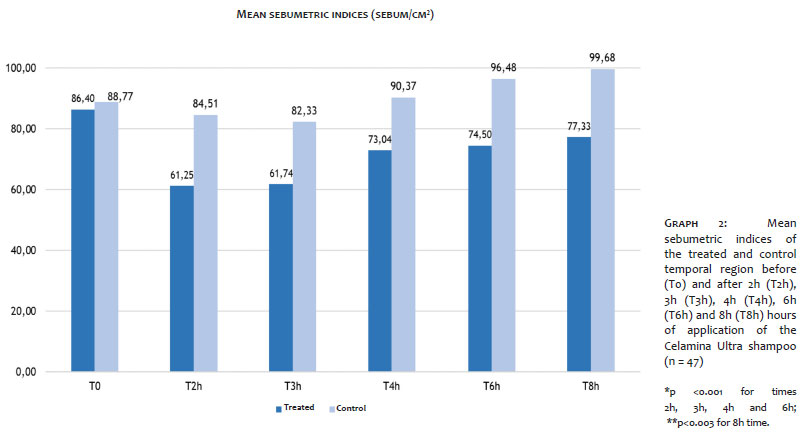
Group 2: Celamina Ultra® (intense SD)
As shown in graph 02, there was also a significant reduction in sebumetry at all times of assessment, statistically significant (p<0.001) when compared to the control area:
Ultra (n=47) *p<0,001 for times 2h, 3h, 4h, and 6h;
**p<0,003 for time 8h.
Both treatments demonstrated effective oil control within 8 hours after the first use of the products.
Both treatments also demonstrated effective oil control at all collection times, up to 8 hours after a single application.
Step 2: Effect on time
Reduction of scaling under conditions of use
Group 1: Celamina Zinco® (moderate SD)
The quantification of scales by image analysis showed a decrease of 54.5% of scales (p<0.001) after two weeks of using the product in monotherapy, which progressed to 74.7% (p<0.001) in four weeks of use.
In the subjective evaluation, 79.5% of the patients reported significant improvement in scaling after the first application. After four weeks of use, 88.6% of patients reported a substantial improvement.
Group 2: Celamina Ultra® (intense SD)
The quantification of scales by image analysis showed a reduction of 64.7 [FA2] [FA4]% of scales (p<0.001) after two weeks using the product as monotherapy, which remained at 62.5% (p <0.001) after four weeks of use.
In the subjective evaluation, 91.5% of the patients reported significant improvement of the scaling right after the first application. After four weeks of use, 97.87% of the patients reported significant improvement.
Both treatments demonstrated control of pityriasis scaling of the scalp, in the prescribed regimen (twice/week) in monotherapy.
Group 1: Celamina Zinco® (moderate SD)
The improvement in pruritus and erythema was reported by 86.36% of patients shortly after the first application. The improvement in pruritus was maintained with the use of the product in monotherapy twice a week, with this improvement reported by 95.45% of patients after four weeks of use.
Group 2: Celamina Ultra® (intense SD)
Improvement in pruritus and erythema was reported by 97.87% of patients shortly after the first application. The improvement in pruritus was maintained with the use of the product in monotherapy twice a week, and this improvement was reported by 93.62% of patients after four weeks of use.
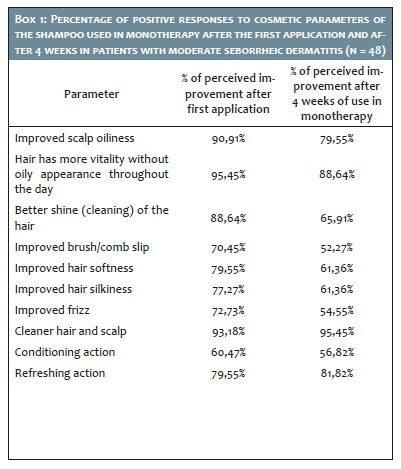
Group 1: Celamina Zinco® (moderate SD)
Box1 shows the subjective results obtained from the questionnaire submitted to the study participants, to assess the cosmetic effect of the products on the hair strands after the first application and prolonged use (four weeks).
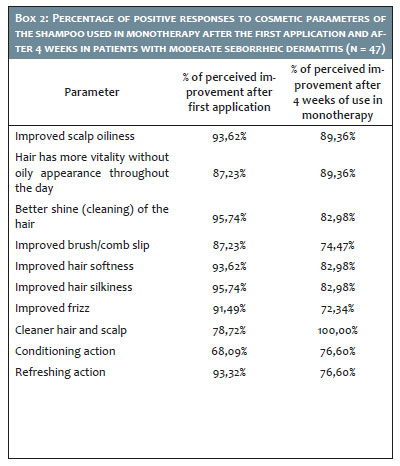
Group 2: Celamina Ultra® (intense SD)
Box 2 shows the subjective results obtained from the questionnaire submitted to the study participants to assess the cosmetic effect of the products on the hair strands after the first application and prolonged use (four weeks).
This study considered relapse as any of the signs and symptoms related to seborrheic dermatitis: pruritus, scaling, and erythema.
Group 1: Celamina Zinco® (moderate SD)
After suspending the use of the products under evaluation, participants were instructed to clean the scalp with a neutral shampoo. After seven days of shampoo removal, it was observed that the percentage of relapse subjectively assessed was 13.6% in the group; regarding pruritus, 9% reported worsening when compared to the period of continuous use of the product.
Compared to the last evaluation after four weeks of use, the increase in possible relapses was not statistically significant (p <0.05).
Regarding the quantitative evaluation of the scaling, it remained 17.7% lower than in the initial measurement, differing significantly from the period before treatment (p<0.001) and without significant difference from the analysis obtained after four weeks of use. These data demonstrate that the product's action in moderate seborrheic dermatitis persisted statistically significant even after a week of shampoo suspension.
Group 2: Celamina Ultra® (intense SD)
In the assessment of seven days after suspension of the shampoo under evaluation, the percentage of relapse subjectively assessed was 14.9% in the group; regarding pruritus, 4% reported worsening when compared to the period of continuous use of the product.
Compared to the last evaluation after four weeks of use, the observed increase was not statistically significant (p<0.05).
Regarding the quantitative evaluation of the scaling, it remained 31.8% lower than in the initial measurement, differing significantly from the period before treatment (p<0.001) and with no significant difference from the analysis obtained after four weeks of use.
These data demonstrate that the product's action on intense seborrheic dermatitis persisted statistically significant even after a week of shampoo suspension.
Although it is a dermatosis with benign evolution, the patient's quality of life with seborrheic dermatitis can suffer a great negative impact due to the embarrassment caused by the itching, the visible lesions on the scalp, and the scaling itself that is also visible on the hair and clothes.9
Adequate hygiene products, popularly known as anti-dandruff shampoos, can provide relief from itching and scaling, being adjuvant to pharmacological treatment, regardless of the intensity of the condition.
Nowadays, formulations of anti-dandruff shampoos use combinations of anti-inflammatory, antifungal, keratolytic, and anti-seborrheic active principles, which interfere with the natural history of acne, and can have a sparing effect on drugs such as topical corticosteroids.
This review article demonstrates that ciclopirox olamine, a known antifungal agent, provides clinical and symptom improvement in rinse formulations when compared to placebo and can reduce relapses up to 12 weeks after the initial treatment phase; although zinc pyrithione has fewer studies, it also demonstrates significant effectiveness against placebo in the control of seborrheic dermatitis, due to its seborregulatory action.2
Its fungistatic effect for Malassezia is widely used. The combination of both active principles promotes a synergy that demonstrated superiority in the antifungal effect over topical ketoconazole.10
Salicylic acid, intended for more scaly conditions, promotes a keratolytic effect by improving scaling, being used in both lotions and shampoos.11
The combination of several classes of active principles is one of the options that produce greater effectiveness and less chance of relapses.12
Although the combination of active principles is crucial for the effectiveness in reducing the signs of dermatitis and preventing relapses, care in formulating the vehicle is essential. They must be specially developed for the particularities of seborrheic dermatitis, such as:
a) an irritated scalp: the association of mild surfactants should not interfere with the skin barrier;
b) hair with chemical processing, such as hair subjected to straightening or dye, whose damaged cortex is more susceptible to the eventual dryness of surfactants to remove the oil from the strands.
The chance of adhering to treatment depends directly on the quality of the vehicle, especially in women. In these patients, the predominance of processed and long hair aggravates dryness and trichotillosis, requiring effective cleansing, but not aggressive to the strands.13
The main element of a shampoo is the surfactant molecule, also called detergent molecule. It is a chemical class with an apolar or hydrophobic portion, capable of binding to sebum lipids and other oily impurities, and a polar or hydrophilic part, which interacts with water, allowing the product to be removed and rinsed. Currently, a tendency to achieve a cleaning efficacy without harming the hair is the association of surfactants with silicones and lipids, minimizing the aggression to the strands.14
In both groups studied, the surfactant system associated with panthenol and tocopherol seems to have exerted an effective cleansing without irritating the scalp. While panthenol assumes a moisturizing role for the scalp and conditioning for the hair,15 tocopherol is an antioxidant, protecting hair and scalp from environmental oxidative stress.16 In the shampoo intended for group 2 (Celamina Ultra®), the presence of olive oils provides a conditioning effect with a mild effect, no leaving residues on the hair and not compromising the cleanliness,17 while the shea butter, in addition to conditioning action, has anti-inflammatory properties.18
The results obtained here in both groups, using Celamina Zinco® or Celamina Ultra® shampoos in monotherapy, demonstrated effective control of moderate to severe seborrheic dermatitis in all its signs: seborrhea, desquamation, and erythema, in addition to pruritus, the most prevalent symptom. The dosage of only twice a week was sufficient to improve oiliness and flaking. The residual effect evaluated positively after a week of suspension of the product, demonstrated the action on the mechanisms of seborrheic dermatitis, reducing its recurrence, even in monotherapy.
The positive assessment on the immediate effect and over time on the hair strands showed comfort of use, improving the softness and combability, reducing oil without drying the hair, in both groups.
Both versions of shampoos studied, combining active principles with proven efficacy with vehicles that do not harm the skin barrier or the hair shaft, were able to promote effective control of the signs and symptoms of moderate to severe seborrheic dermatitis. These formulations have also demonstrated that they do not harm the hair strands, even when processed, providing comfort during use, which is considered fundamental to treatment adherence.
Flávia Alvim Sant’anna Addor | 0000-0003-1851-7342
Study design and planning; preparation and writing of the manuscript; active participation in research orientation; critical literature review; critical revision of the manuscript.
Sandro Caballero Barbosa | 0000-0002-2759-457X
Approval of the final version of the manuscript; study design and planning; data collection, analysis, and interpretation; critical revision of the manuscript.
1. Aschoff R, Kempter W, Meurer M. Seborrheic dermatitis. Hautarzt. 2011;62(4):297-307.
2. Naldi L, Diphoorn J. Seborrhoeic dermatitis of the scalp. BMJ Clin Evid. 2015:1713. Epub 2015 May 27.
3. Smith SA; Baker AE; Williams JH. Effective treatment of seborrheic dermatitis using a low dose, oral homeopathic medication consisting of potassium bromide, sodium bromide, nickel sulfate, and sodium chloride in a double-blind, placebo-controlled study. Altern Med Rev. 2002;7(1):59-67.
4. Barak-Shinar D, Green LJ. Scalp seborrheic dermatitis and dandruff therapy using a herbal and zinc pyrithione-based therapy of shampoo and scalp lotion. J Clin Aesthet Dermatol. 2018;11(1):26-31.
5. Draelos ZD, Kenneally DC, Hodges LT, Billhimer W, Copas M, Margraf C. A comparison of hair quality and cosmetic acceptance following the use of two anti-dandruff shampoos. J Investig Dermatol Symp Proc. 2005;10(3):201-4.
6. Bailey P, Arrowsmith C, Darling K, Dexter J, Eklund J, Lane, A. A double-blind randomized vehiclecontrolled clinical trial investigating the effect of ZnPTO dose on the scalp vs. antidandruff efficacy and antimycotic activity. Int J Cosmet Sci. 2003;25(4):183-8
7. Ratnavel RC, Squire RA, Boorman GC. Clinical efficacies of shampoos containing ciclopirox olamine (1.5%) and ketoconazole (2.0%) in the treatment of seborrheic dermatitis. J Dermatolog Treat. 2007;18(2):88-96.
8. Bacon RA, Mizoguchi H, Schwartz JR. Assessing therapeutic effectiveness of scalp treatments for dandruff and seborrheic dermatitis, part 1: a reliable and relevant method based on the adherent scalp flaking score (ASFS). J Dermatolog Treat. 2014;25(3):232-6.
9. Chen SC, Yeung J, Chren MM. Scalpdex: a quality-of-life instrument for scalp dermatitis. Arch Dermatol. 2002;138(6):803-7.
10. Roques C, Brousse S, Panizzutti C. In vitro antifungal efficacy of ciclopirox olamine alone and associated with zinc pyrithione compared to ketoconazole against Malassezia globosa and Malassezia restricta reference strains. Mycopathologia. 2006;162(6):395-400.
11. Squire RA, Goode K. A randomised, single-blind, single-centre clinical trial to evaluate comparative clinical efficacy of shampoos containing ciclopirox olamine (1.5%) and salicylic acid (3%), or ketoconazole (2%, Nizoral) for the treatment of dandruff/seborrhoeic dermatitis. J Dermatolog Treat. 2002;13(2):51-60.
12. Sampaio ALSB, Mameri ACA, Vargas TJS, Ramos-e-Silva M, Nunes AP, Carneiro SCS. Dermatite Seborreica. An Bras Dermatol. 2011;86(6):1061-74.
13. Draelos ZD. Essentials of hair care often neglected: hair cleansing. Int J Trichology. 2010;2(1):24-9.
14. Abraham LS, Moreira AM, Moura LH, Gavazzoni MFR; Addor FAS. Tratamentos estéticos e cuidados dos cabelos: uma visão médica (parte 2). Surg Cosmet Dermatol. 2009;1(4):178-85
15. Madnani N, Kaleem K. Hair cosmetics. Indian J Dermatol, Venereol, and Leprol. 2013;79(5):654.
16. Zulli F, Belser E, Neuenschwander MP, Mibelle RM. Antioxidants from grape seeds protect hair against reactive oxygen species. Personal Care. 2001:65-7.
17. Cecatto OS, Scatolin DAB. O uso da oliva em formulações cosméticas. Medicina e Saúde. 2018;1(1):61-71.
18. Vorster, Abby. New inspiration and innovation: hair care. South African Pharmaceutical and Cosmetic Review. 2013;40(9):36-40.
 All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773
All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773



 Read in Portuguese
Read in Portuguese
 Portuguese PDF
Portuguese PDF
 Print
Print
 Send this article by email
Send this article by email
 How to cite this article
How to cite this article
 Submit a comment
Submit a comment
 Mendeley
Mendeley
 Pocket
Pocket
{kind=link}
{kind=link}
{kind=link}
{kind=link}