


André Cesar Antiori Freire Pessanha1; Rebecca Silveira1; Fabianne Hemy Chu2; Beatriz R. Siqueira da Silva Costa2; Maria Gabriela Brandão Carneiro2; Marjorie Sayuri Yoshii3
Received on: 12/04/2020
Approved on: 06/06/2020
Financial support: None
Conflict of interest: None
Study conducted at the Dermatology Service of the Universidade de Mogi das Cruzes, Mogi das Cruzes (SP), Brazil
INTRODUCTION: Basal cell carcinoma (BCC) is the most common malign neoplasm. It corresponds to 70-80% of skin tumors. The diagnosis is made based on clinical suspicion combined with dermoscopy, which also allows defining its limits.
OBJECTIVE: To assess whether clinical and dermoscopic criteria are sufficient for the diagnosis and treatment of primary and well-defined BCC.
MATERIALS AND METHODS: Review of suspected cases of well-defined primary BCC surgically approached by excisional biopsy (3 mm margin) at the Dermatology Service of the University of Mogi das Cruzes (2017 to 2019). The Chi-square test was applied to assess the significance of the margins.
RESULTS: 169 injuries were assessed, with a predominance of women in the 8th decade. The histopathological examination concluded on 141 BCCs. When evaluating the excision margins for BCC cases, there was 95% of free margins (p = 0.0004998).
DISCUSSION: There are common dermoscopic elements between BCC and other neoplasms and benign lesions, which justifies other diagnoses found. The 3 mm surgical margin was accurate for well-defined primary BCCs, speeding up healing time and reduces costs.
CONCLUSION: For clinical-dermatoscopic suspicions of well-defined BCC, an excisional biopsy was effective in the diagnosis and clinical safety margins.
Keywords: Dermatoscopy; Diagnosis; Free margins
Basal cell carcinoma (BCC) is the most common malignant neoplasm in humans. It corresponds to 70-80% of cutaneous tumors. Exposure to ultraviolet radiation (UVR) is its main risk factor. Constitutional risk factors are Fitzpatrick's skin phototypes I and II, freckles in childhood, and family history (30% to 60%). It affects more men than women (probably due to factors of occupational exposure). Still, but studies reveal a recent increase in the proportion of women (odds ratio = 1.5), even under 40 years old. This can be attributed to the higher demand for dermatological care, laser treatments, photo exposure, and the use of tanning beds. BCC incidence has been increasing at a rate of 10% per year. Depletion of the ozone layer and increased longevity are other factors involved.1
Clinically, BCC has the following variants: nodular/ ulcerative (the most common type, located in the head and neck in general), superficial (found in trunk and shoulders), sclerodermiform (the one presenting the worst prognosis, situated in the face in general), pigmented (more frequent in melanoderms), and fibroepithelioma (located in lumbosacral, pubic, and genitocrural regions). Histologically, its variants are solid, adenoid, pigmented, micronodular, sclerodermiform, infiltrative, metatypical (basal squamous). The first three are considered of low risk, while the others present worse prognosis.1
The diagnosis of BCC is based on clinical suspicion. Dermoscopy increases diagnostic accuracy. Test performance studies have shown that dermoscopy, compared to the naked eye, improves sensitivity from 66.9% to 85%. Specificity, on the other hand, increases from 97.2% to 98.2%.2
There is a classification to define BCC as high or low risk. Low-risk tumors are primary tumors, with well-defined margins, low-risk histological subtypes, presented in immunocompetent individuals, without previous radiotherapy or perineural involvement. Any opposite parameter defines the high-risk tumor.3
As for topography, areas L (low risk), M (medium risk), and H (high risk) are defined. L area is composed of limbs and trunk, except for the pre-tibial area, hands, and feet. M area is composed of the forehead, cheeks, scalp, neck, and pre-tibial area. H area is composed of the central region of the face (perioral, chin, nose, periorbital), and temples and ears, hands, feet, and genitalia. Defining the area's risk and tumor’s size of the tumor in each of these areas is determinant to classify it as high or low risk. The low-risk tumor is less than 20mm, if located in an L area, less than 10mm in an M area, and does not affect the H area by definition. Values higher than or equal in the respective areas mentioned or the H area's involvement define the high-risk tumor.3
There are incisional biopsy techniques that can be performed to confirm or exclude the diagnosis: shaving biopsy (more comprehensive, but it can generate perilesional erythema that overestimates the tumor margin a posteriori), and punch biopsy (although without the previous inconvenience, may not incorporate other histological patterns that would modify the lesion risk). Retrospective analyzes also show a 60.9% agreement between pre-surgical biopsies and the result after final excision.3
Given the dermoscopy diagnostic accuracy, which allows the identification of BCC's subclinical structures in apparently healthy skin,4 it is possible to establish its limits, especially if the tumor is well delimited. From these limits, the desired incision margin is implemented. For small tumors (less than 2cm), 3mm to 4mm are usually sufficient to achieve a cure. Recurrence rates over five years are 0.7% to 5% for low-risk lesions.3
The literature is scarce when researching the excisional biopsy method of BCC, given the accuracy of dermoscopy for its diagnosis2 and definition of margins.4
To assess whether clinical and dermoscopic criteria can be sufficient for the resolution in a single surgical procedure (excisional biopsy) for the diagnosis and treatment of primary and well-defined BCC. The secondary objective is to assess the epidemiological profile of these patients.
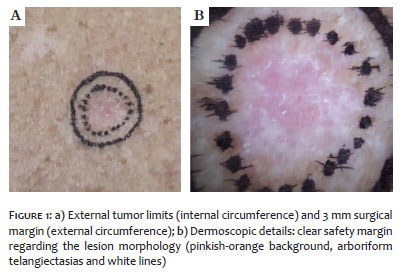
Review of suspected cases of primary, well-limited BCCs (clinical-dermoscopic criteria, using the “Chaos and Clues” algorithm), operated by excisional biopsy (3mm margin from the dermoscopy mark) (Figure 1) at the Dermatology Service of the University of Mogi das Cruzes in the years 2017, 2018 and 2019.
Data collection was based on the information present in the Excel table containing the numbers of patients' medical records, in addition to data such as age, gender, location of lesions, diagnoses found, BCC subtypes, wound closure method, and free margins.
This study had a quantitative nature, descriptive statistical method, anonymous character, exploratory-descriptive approach, and cross-section. We obtained the approval from the Research Ethics Committee (CEP) no: 2,991,936 and Certificate of Presentation for Ethical Appreciation (CAAE) no: 011515118.0.0000.5497.
The dependent variables of interest were the margins of the BCC through the dermatoscope and the anatomopathological examination (AP). The independent variables were: gender, year of collection, age of the patient, location of the BCC through the AP exam, and subtype (AP). As qualitative variables, contingency tables were made, and the chi-square test (c2) was applied with a 95% significance level (20,000,000 bootstraps to estimate the p-value) to verify the relationships between them. Such analyzes were performed in the statistical software R (R Core Team, 2019) with the “gplots” (Warnes et al., 2020) and “corrplot” (Wei & Simko, 2017) packages.
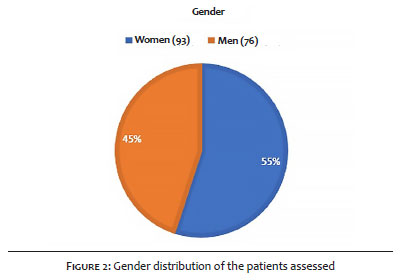
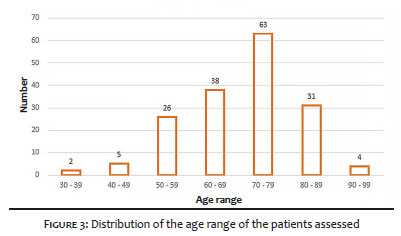
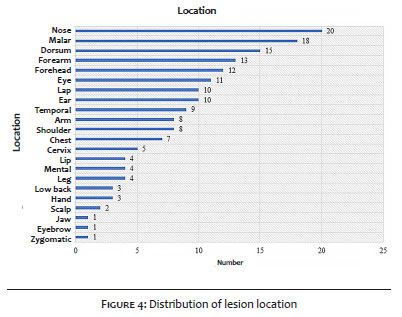
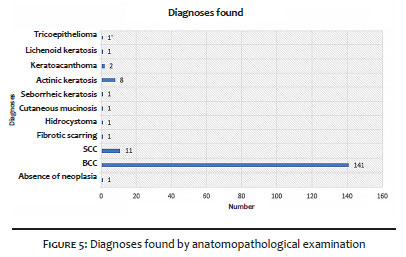
We assessed 169 injuries. Most of the patients were women (55%) (Figure 2). The predominant age group was the 8th decade (37%) (Figure 3). As for the location, 63 lesions (37%) were detected in the H area, 42 (25%) in the M area, and 64 (38%) in the L area (Figure 4). Histopathological examination detected 141 cases of BCC (Figure 5), corresponding to a positive predictive value of 83.4% with the use of dermoscopy.
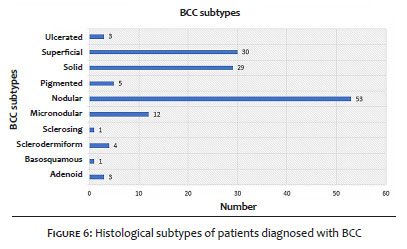
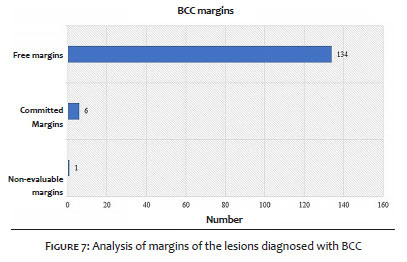
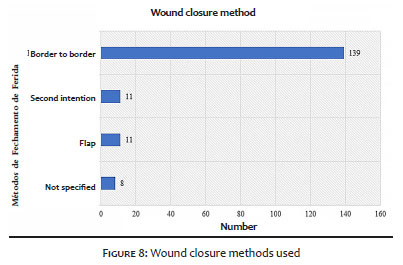
The nodular histological subtype (considering the “solid” variant as a synonym) was the most common finding among BCCs, with 82 cases found (58%) (Figure 6). The following proportion is classified into high x low histological risk subtypes: 21 cases (14.1%) x 120 cases (85%), respectively. Considering the BCC cases, there is an increase to 95% of cases with free margins (134/141) (Figure 7), with statistical significance by the chi-square test (p = 0.0004998). Of the six cases with compromised margins, four were located in the nasal region, one in the chin (in which reconstruction using a skin flap was adopted), and one in the neck. Simple closures (including edge to edge and secondary intention) corresponded to 150 cases (88.7%) (Figure 8).
In this study, 83.4% of suspected cases of BCC were histologically confirmed (Figure 5). Considering other keratinocytic neoplastic lesions (squamous cell carcinoma - SCC, keratoacanthoma - KA, actinic keratosis - AK), this index reaches 95.8% (Figure 5).
This index is defined as a positive predictive value (true-positive/ true - positive + false-positive). Therefore, although there are classic dermoscopic criteria for BCC in some cases, in others there is an overlap of differential diagnoses.
The dermoscopic “Chaos and Clues” method recommends starting the assessment by the “chaos” of the lesion analyzed, suggesting malignancy. From then on, clues are searched for a maximum approximation of the diagnosis. However, there are common elements between BCC and other neoplasms and benign lesions:5 ulceration (BCC x SCC), white lines (BCC x lichenoid keratosis-LK), polymorphic vessels (CBC x seborrheic keratosis-SK x LK), vessels in points/ twisted /serpentine (BCC x scarring), radial vessels (ulcerated BCC x SCC).5 It is important to remember the possibility of lesion collisions such as BCC and SK.6
The 3mm surgical margins were appropriate for well-defined primary BCCs. With adequate logistical management (low-risk stratification, little personal impact of a patient’s scar, simple closing technique, availability for an agile margin enlargement, if necessary), the excisional biopsy in these cases has a positive impact. It can streamline the healing process and reduce the patient’s anguish7 when waiting for a pre-result of the incisional biopsy and surgery, given the stigmatization of cancer. Also, there is a tendency of economic benefit for the assistance service (lower cost of surgical materials and optimized use of the surgical-dermatological sector).8 Considering a small lesion, there would be an additional advantage of performing an excisional biopsy: evaluating of all histological subtypes present in the lesion.
Despite having essential characteristics for low-risk BCC, many lesions were in the H area (Figure 4). Even five of the six lesions with margin involvement were found in this region. Also, this study doesn't mention the lesions' dimension to classify them as high or low risk. Even in high-risk lesions, this excisional biopsy method is considered interesting with some caveats: small and well-defined lesions in H area, reconstruction method that does not generate significant anatomical distortion (edge-to-edge or secondary intention) and the availability for early re-approach, with the appropriate technique (example: Mohs micrographic surgery in the H area) if the margins are compromised.
The result of less aggressive histological types (85%) composing most of the results confirms the clinical-histological correlation for most well defined cases.
The preponderance in women (against the data in the literature, which, however, points to an upward incidence in women) suggests a current gender survey for low-risk tumors or general BCC epidemiology. It was observed that the face, even with well-defined lesions, is an area of significant involvement (46% of biopsied lesions), with a higher emphasis on the nasal region.
For very limited clinical-dermoscopic suspicions of BCC, excisional biopsy with a 3 mm margin proved effective in terms of diagnosis and safety margins.
André Cesar Antiori Freire Pessanha | ORCID: 0000-0001-9806-4245
Treatment and monitoring of patients; data collection; critical literature review; preparation and writing of the manuscript.
Rebecca Silveira | ORCID: 0000-0001-7164-4717
Treatment and monitoring of patients; data collection; critical literature review; preparation and writing of the manuscript.
Fabianne Hemy Chu | ORCID: 0000-0001-7070-4570
Statistical analysis; study design and planning; preparation and writing of the manuscript; data collection, analysis, and interpretation.
Beatriz Rodrigues Siqueira da Silva Costa | ORCID: 0000-0001-7911-7735
Statistical analysis; study design and planning; preparation and writing of the manuscript; data collection, analysis, and interpretation.
Maria Gabriela Brandão Carneiro | ORCID: 0000-0002-2009-9568
Statistical analysis; study design and planning; preparation and writing of the manuscript; data collection, analysis, and interpretation.
Marjorie Sayuri Yoshii | ORCID: 0000-0002-7086-1119
Statistical analysis; study design and planning; preparation and writing of the manuscript; data collection, analysis, and interpretation.
1. Chinem VP, Miot HA. Epidemiologia do carcinoma basocelular. An Bras Dermatol. 2011;86(2):292-305.
2. Reiter O, Mimouni I, Gdalevish M, Marghoob AA, Levi A, Hodak E, et al. The diagnostic accuracy of dermoscopy for basal cell carcinoma: a systematic review and meta-analysis. J Am Acad Dermatol. 2019;80(5):1380-8.
3. Cameron MC, Lee E, Hibler BP, Giordano CN, Barker CA, Mori S, et al. Basal cell carcinoma: contemporary approaches to diagnosis, treatment, and prevention. J Am Acad Dermatol. 2019;80(2):321-39.
4. Lallas A, Apalla Z, Ioannides D, Argenziano G, Castagnetti F, Moscarella E, et al. Dermoscopy in the diagnosis and management of basal cell carcinoma. Future Oncol. 2015;11(22):2975-84.
5. Rosendahl C, Cameron A, Tschandl P, Bulinska A, Zalaudek I, Kittler H. Prediction without pigment: a decision algorithm for non-pigmented skin malignancy. Dermatol Pract Concept. 2013;4(1):59-66.
6. Kurihara Y, Furue M. Occult basal cell carcinoma arising in seborrheic keratosis. Case Rep Dermatol. 2019;11(1):48-5.
7. Caddick J, Green L, Stephenson J, Spyrou G. The psycho-social impact of facial skin cancers. J Plastic Reconstr Aesthet Surg. 2012;65(9):e257-Mudigonda T, Pearce DJ, Yentzer BA, Williford P, Feldman SR. The economic impact of non-melanoma skin cancer: a review. J Natl Compr Canc Netw. 2010;8(8):888-96.
 All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773
All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773



 Read in Portuguese
Read in Portuguese
 Portuguese PDF
Portuguese PDF
 Print
Print
 Send this article by email
Send this article by email
 How to cite this article
How to cite this article
 Submit a comment
Submit a comment
 Mendeley
Mendeley
 Pocket
Pocket
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}