


Felipe Bochnia Cerci1,2; Elisa Kubo1
Received on: 20/02/2020
Approved on: 03/03/2020
Research conducted at Centro Especializado da Pele (Cepelle) and Hospital de Clínicas, Universidade Federal do Paraná (UFPR), Curitiba, Brazil.
Financial support: None
Conflict of interests: None
INTRODUCTION: The nose is frequently affected by cutaneous carcinomas. Due to its functional and cosmetic importance, tumors on this location are preferably treated by Mohs micrographic surgery, which provides the highest cure rates. For repairing of surgical defects several options are available, including healing by second intention, primary closure, skin grafts, and flaps. In certain cases, one should consider a combination of methods.
OBJECTIVE: To describe the authors' experience in nasal reconstruction after Mohs surgery and to assess if the number of involved subunits influenced the use of combined repairs.
METHODS: Retrospective study of consecutive cases submitted to Mohs surgery and nasal reconstruction by one of the authors during a 3-year period.
RESULTS: 208 cases were included, and the most common repair method were flaps (n = 82). Combined methods were performed in 44/154 (29%) cases with involvement of only one nasal anatomical subunit and 29/54 (54%) cases with multiple nasal subunits involved.
CONCLUSIONS: The dermatologic surgeon should be familiar with different options for nasal reconstruction. The combination of repair methods was often performed, mainly for wounds that affected more than one nasal subunit.
Keywords: Carcinoma, basal cell; Mohs surgery; Nose neoplasms; Surgical flaps
The nose is one of the facial units most frequently affected by carcinomas of the skin.1 Due to the aesthetic and especially functional importance of the nose, it is crucial to offer patients treatments with lower chances of recurrence. Thus, various guidelines recommend Mohs micrographic surgery (MMS) for cutaneous carcinomas located in this region.2-4 The technique consists of 100% assessment of the surgical margins, compared to examination of around 1% in the conventional excision.5,6 This complete assessment of the margins provided by MMS leads to the highest cure rate in the treatment of carcinomas, and its indication is thus important in noble areas of the face such as the nose.7
Even with MMS, which preserves healthy tissue, many nasal surgical defects are challenging because of the complex local anatomy, with its peculiar three-dimensionality. The priority of nasal restoration should be functional before aesthetic, but the latter should never be overlooked, since postoperative nasal deformities can have significant psychological impact.8 It is thus essential to combine both aspects, functional and aesthetic.
The repair of nasal surgical defects should consider their diameter and depth, the availability of adjacent skin, and the patient's expectations9,10 Numerous options are available, including healing by secondary intention, primary closure, skin grafts, and flaps. A combination of methods should be considered in certain cases.
One of the main factors that influences the choice of reconstruction method is the availability of skin adjacent to the wound. On the nose, this availability is limited in the lower third, formed by the tip, ala, columella, and soft triangles. In the upper thirds (nasal sidewalls and dorsum), the skin usually tends to be less sebaceous and more elastic.
The study aimed to describe the authors' experience with nasal reconstruction after Mohs micrographic surgery and to assess whether the number of affected anatomical subunits influenced the use of combined methods for repair.
This was a retrospective study of consecutive cases submitted to MMS and nasal reconstruction by one of the authors (FBC) from January 2017 to December 2019. The cases were from the private practice and the university hospital where the authors work. The study was approved by the local Institutional Review Board.
Nearly all of the surgeries were performed under local anesthesia with lidocaine and bupivacaine with vasoconstrictor. When necessary, nerve block (external nasal branch of the ethmoidal nerve, supratrochlear, or infraorbital) supplemented the local anesthesia. For larger reconstructions or more anxious patients, oral benzodiazepine (lorazepam) was associated at a dose of 1mg. Antibiotic prophylaxis is a controversial issue11-13, and the authors follow the recommendation by Wright et al., which consists of administering 2g of cephalexin 30 minutes before surgery in cases with higher likelyhood of requiring nasal flaps and/or grafts or for patient's reasons (orthopedic prostheses, immunosuppression, prosthetic heart valves).14 Postoperative antibiotic (cephalexin 500mg every six hours for seven days) was prescribed after complex surgeries, long duration or when cartilage graft was required.
Data analysis included a review of the photographic documentation and the following data: age, gender, Fitzpatrick skin phototype, tumor characteristics, defect size and number of anatomical subunits involved, number of MMS stages, reconstruction performed, use of antiplatelet agents or anticoagulants, smoking, and postoperative complications.
The nasal subunits were divided into dorsum and nasal sidewalls (upper thirds) and tip, ala, columella, and soft triangles (lower nasal third).15 The reconstruction methods were divided into healing by secondary intention, primary closure, flaps, or graft. When more than one method was used, it was reffered as combined reconstruction. For analysis of the repair methods, we only considered the ones for closure of the nasal subunits. Methods used in adjacent subunits (cheek, for example) were not analyzed together, to avoid biases.
Complications were divided into two groups. Short-term complications were defined as bleeding that required reintervention, hematoma, infection, dehiscence, and flap/graft necrosis (partial or total). Long-term complications were defined as easily noticeable anatomical distortion (e.g., retraction of the nasal rim) and nasal obstruction.
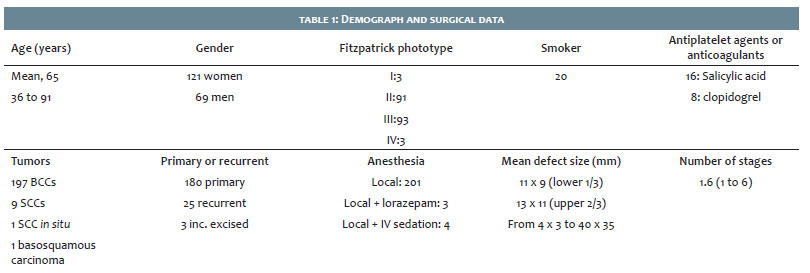
The study included 208 cases from 190 patients. Two other patients were excluded, since they were referred to plastic surgery for reconstruction after MMS. Table 1 shows the demographic and surgical data.
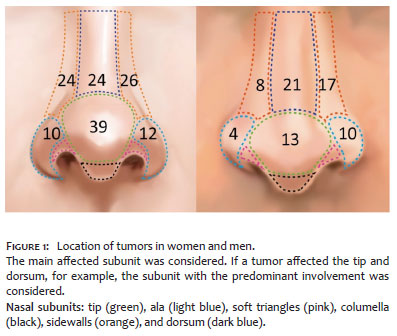
The most primarily affected nasal subunits were the nasal sidewalls (n=75), followed by nasal tip (n = 52), dorsum (n = 45), and ala (n = 36) (Figure 1). In 154 cases, only one nasal subunit was involved, whereas in 54 two or more subunits were affected. In 15 cases, the wound extended to other subunits of the face (cheek=12, apical triangle=1, upper cutaneous lip=1, and eyelid=1). In such cases, the subunits beyond the nose were restored by primary closure or (n=8) by secondary intention (n=7).
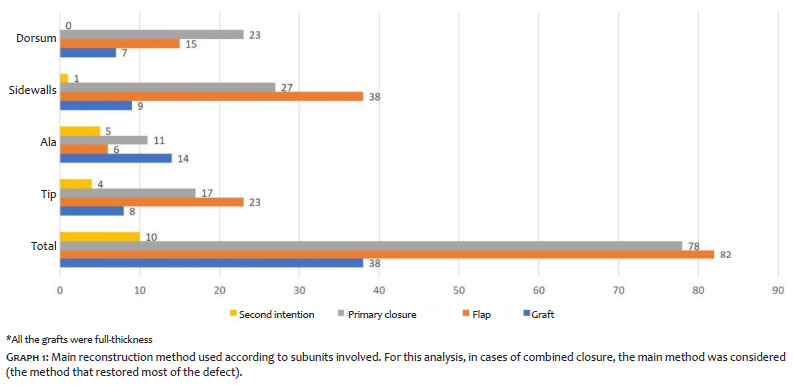
Graph 1 shows the reconstruction methods performed. For the nasal dorsum, primary closure was the most frequently used. Flaps were the most common for the nasal sidewalls and tip, and grafts for the nasal ala. Regarding the flaps, in 82 cases they were the main repair method: rotation (n=21), island pedicle (n=15), transposition (n=14), advancement (n=12), island with lateral pedicle of the nasalis muscle (n=8), interpolation (n=6), and hinge (n=6). Two patients underwent surgical revision. One because of webbing on the inner canthus, treated with Z-plasty; and the other for thinning the flap. In four cases, intralesional steroids were was used with satisfactory results for treatment of "trapdoor".
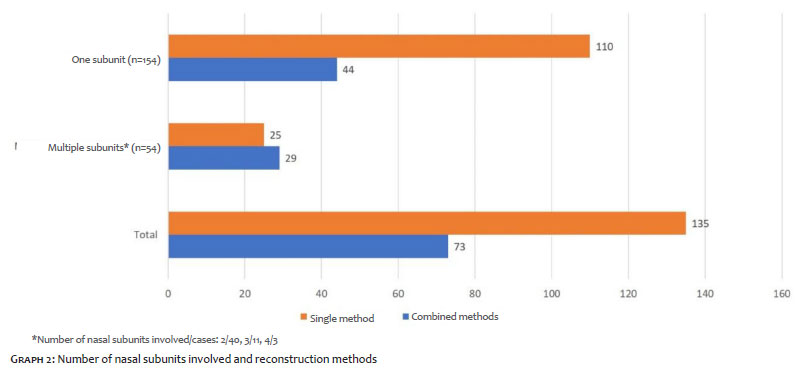
Among the 154 cases with involvement of only one nasal subunit, 110 (71%) were restored with a single method and 44 (29%) with combined methods. Among the cases with multiple nasal subunits involved (n=54), in 29 (54%) a combination of methods was used for closure (Graph 2).
Pre- and postoperative prophylactic antibiotics were used in 104 and 41 cases, respectively. Complications occurred in 6.2% (n=13) of the cases, 12 were short-term and one was long-term. The most common complications were infection (n=4) and partial graft necrosis (n=4), followed by partial flap necrosis (n=3), dehiscence (n=1), and nasal valve disfunction (n=1). Infections were treated with oral antibiotics and healed uneventfully. Partial flap or graft necrosis were managed with local wound care. The patient that presented dehiscence, after early removal of the sutures, healed by secondary intention. The case of nasal valve disfunction due to inadequate flap design evolved with partial improvement and refused surgical revision.
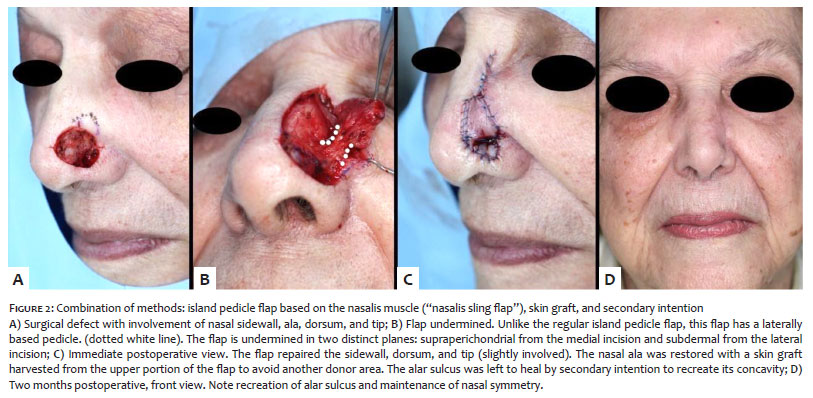
Similarly to previous publications, the current study demonstrated the variety of available options for nasal reconstruction and the frequent need for flaps and grafts, even on the upper thirds of the nose.16-19 It also showed that defects involving multiple nasal subunits were more often repaired with a combination of methods. This is especially true for defects involving the nasal ala and sidewall, where preservation of the alar sulcus is essential for facial symmetry (Figure 2).20,21
The repair choice varied according to the number and to nasal subunits involved. Similarly to previous reports, flaps were the most frequent reconstruction method.17,22
In a study that compared the outcomes of flaps and grafts for nasal restoration, the authors showed that well-designed flaps were more likely to result in superior cosmetic outcome.23
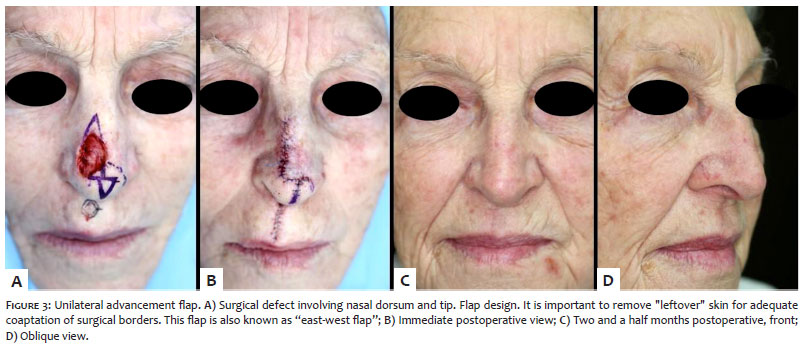
The nasal dorsum, due to the greater elasticity of adjacent areas (glabella and nasal sidewalls), was restored with primary closure or flap in 85% of cases. Figure 3 illustrates an excellent option of an advancement flap for this site, also known as the "east-west flap".24 When performing a vertical primary closure on the nasal dorsum, the standing cones should be long to reduce the risk of uneven levels between the sutured area and upper and lower adjacent areas.25 Although hard to notice from a front view this unevenness is easily noticed from side view.
For the nasal sidewall, flaps and primary closure were the most frequently used, a finding consistent with the literature.17,26 Figure 2 illustrates a combined repair for a defect affecting multiple subunits, the main one the left nasal sidewall. For flaps that recruit tissue from the cheek, two details deserve attention. The first is the maintenance of the nasofacial sulcus, especially when using lateral advancement flaps. This can be performed by fixing the deep portion of the flap on the nasofacial sulcus. Another detail is to adequately thin island pedicle flaps, since the nasal sidewall is much thinner than the cheek.
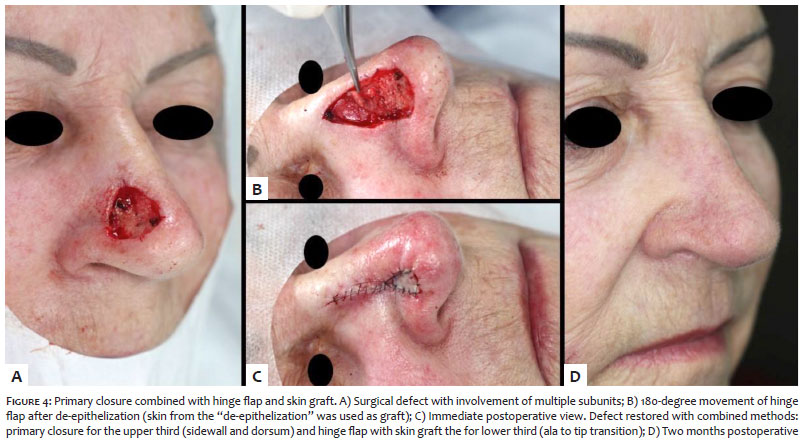
For the nasal tip, flaps and primary closure were the most common repair method. Among the flaps, the rotation was the most frequently performed. It allows incisions to be hidden between subunits (sidewall and dorsum, or nasofacial sulcus). The disadvantage is that this flap requires long incisions and significant undermining for adequate mobility and avoidance of nasal tip distortion. Another frequently used option was a variation of the Burow's graft, which consists on the combination of primary closure and a hinge flap and graft (both from the Burow's triangle)27, similar to the method illustrated in figure 4.
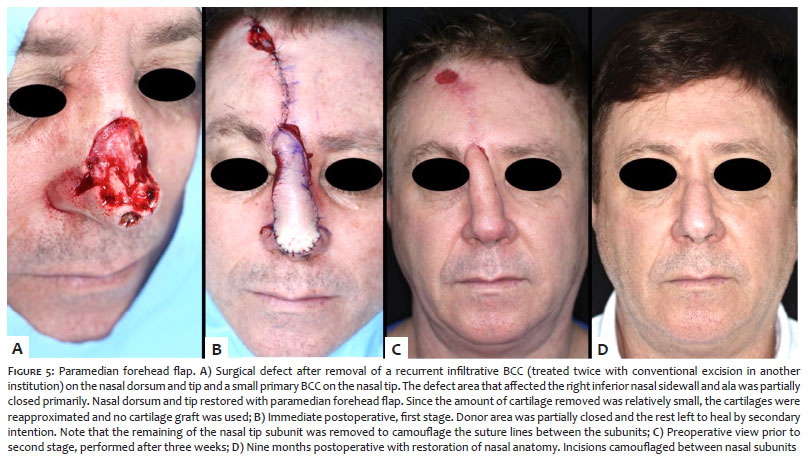
For extensive and deep defects of the nasal tip (in some cases with involvement of the dorsum), the paramedian forehead flap was performed (Figure 5), allowing adequate restoration of the nasal anatomy, as described in the literature.9, 28-30
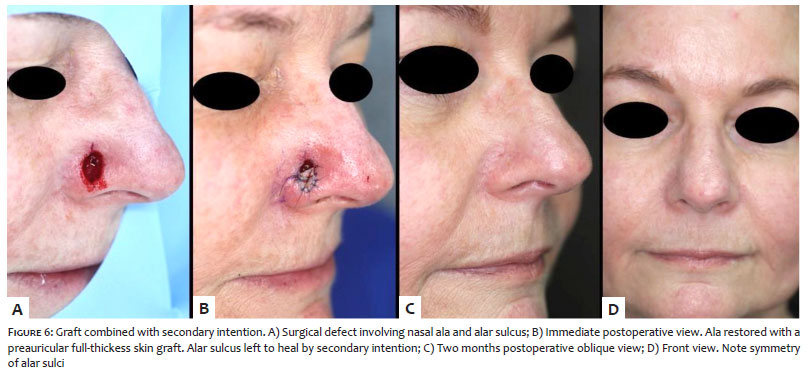
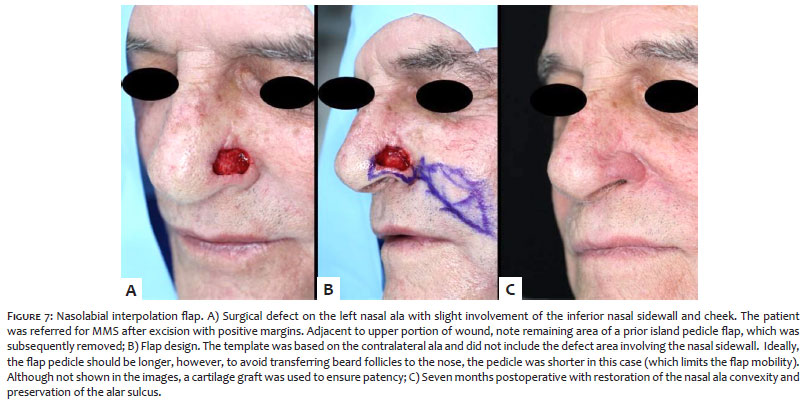
The nasal ala was the only subunit where graft was the main repair method despite numerous described flaps from the ala itself.31,32 Because of the lack of support and the fact that the ala is a free margin, any minimal flaw when designing flaps from the ala itself can cause local distortion. For this reason, this author usually prefers grafts for small defects 33 and secondary intention when the alar sulcus is involved, or a combination of both (Figure 6). Primary closure can be useful for small alar defects, mainly those located on the medial portion of the ala adjacent to the tip. On the central or lateral portion, even small primary closures can cause collapse because of the vector that "pushes the ala inward". In the current study, secondary intention was one of the repair methods in 50% of the defects that involved the ala to some extent. The areas left to heal by secondary intention were mostly adjacent to the alar sulcus, a well-established practice in the literature.34 Single-stage transposition flaps tend to obliterate the alar sulcus, causing easily noticeable asymmetry. Therefore, in cases with extensive involvement of the ala, the nasolabial interpolation flap (with cartilage graft) was performed (Figure 7). The technique requires two stages, however it allows recreating the entire alar subunit, besides preserving the alar sulcus.28,35,36
Almost all the surgeries (97%) were performed under local anesthesia, which is consistent with the literature from the United States, where MMS is performed on a large scale and only on extremely rare occasions under sedation.37-39 Local anesthesia is the safest method for the patient, since MMS can take hours.5,39-42 It is essential to use established techniques to reduce discomfort from local anesthesia on every patient.
One limitation of the current study is its retrospective design. However, the data from each surgery were uploaded into a database immediately after the procedure. Long-term data were uploaded after follow-up visits. These measures minimize possible retrospective study biases. Another limitation is that the study is based on a surgeon's preference, which can vary significantly, as reported by Alam et al. 43
Finally, the authors are not proponents of cookbook formulas such as "defects up to 1.5cm on the nasal tip should be closed with a bilobed flap" etc.44 The authors recommend careful evaluation of each defect and each nose. Same size defects on different nasal tips can be repaired by completely different methods according to local characteristics.45 Therefore, more important than memorizing algorithms is to become familiar with different repair methods and flap biomechanics. This does not mean that surgeons should always do a distinct reconstruction for every case, but that they have a reasonable range of options.
Dermatologic surgeons should be familiar with the different options for nasal reconstruction. The combination of repair methods was frequently performed, mainly for defects involving more than one nasal subunit.
Felipe Bochnia Cerci | ORCID 0000-0001-9605-0798
Statistical analysis, approval of the final version of the manuscript, study conception and planning, elaboration and writing of the manuscript, data collection, analysis, and interpretation, effective participation in orientation of the research, intellectual participation in the propaedeutic and/or therapeutic conduct of the cases, critical review of the literature, critical revision of the manuscript.
Elisa Kubo | ORCID 0000-0001-7096-4372
Approval of the final version of the manuscript, study conception and planning, data collection, analysis, and interpretation, effective participation in orientation of the research, critical review of the literature, critical revision of the manuscript.
1. Scrivener Y, Grosshans E, Cribier B. Variations of basal cell carcinomas according to gender, age, location and histopathological subtype. Br J Dermatol. 2002;147(1):41-7.
2. Work Group, Invited Reviewers, Kim JYS, Kozlow JH, Mittal B, Moyer J, et al. Guidelines of care for the management of basal cell carcinoma. J Am Acad Dermatol. 2018;78(3):540-59.
3. Telfer NR, Colver GB, Morton CA, British Association of Dermatologists. Guidelines for the management of basal cell carcinoma. Br J Dermatol. 2008;159(1):35-48.
4. Bichakjian CK, Olencki T, Aasi SZ, Alam M, Andersen JS, Berg D, et al. Basal Cell Skin Cancer, Version 1.2016, NCCN Clinical Practice Guidelines in Oncology. J Natl Compr Canc Netw. 2016;14(5):574-97.
5. Tolkachjov SN, Brodland DG, Coldiron BM, Fazio MJ, Hruza GJ, Roenigk RK, et al. Understanding Mohs Micrographic Surgery: A Review and Practical Guide for the Nondermatologist. Mayo Clin Proc. 2017;92(8):1261-71.
6. Kimyai-Asadi A, Goldberg LH, Jih MH. Accuracy of serial transverse cross-sections in detecting residual basal cell carcinoma at the surgical margins of an elliptical excision specimen. J Am Acad Dermatol. 2005;53(3):469-74.
7. Ad Hoc Task Force, Connolly SM, Baker DR, Coldiron BM, Fazio MJ, Storrs PA, et al. AAD/ACMS/ASDSA/ASMS 2012 appropriate use criteria for Mohs micrographic surgery: a report of the American Academy of Dermatology, American College of Mohs Surgery, American Society for Dermatologic Surgery Association, and the American Society for Mohs Surgery. J Am Acad Dermatol. 2012;67(4):531-50.
8. Sobanko JF, Sarwer DB, Zvargulis Z, Miller CJ. Importance of physical appearance in patients with skin cancer. Dermatol Surg. 2015;41(2):183-8.
9. Boyd CM, Baker SR, Fader DJ, Wang TS, Johnson TM. The forehead flap for nasal reconstruction. Arch Dermatol. 2000;136(11):1365-70.
10. Chi JJ, Rosenberg A, Hahn S, Piccirillo JF, Politi M, Kallogjeri D, et al. Patient Concerns About Nasal Reconstruction After Mohs Surgery and Implications for Shared Decision Making. JAMA Otolaryngol Head Neck Surg. 2018;144(12):1180-1.
11. Saleh K, Schmidtchen A. Surgical site infections in dermatologic surgery: etiology, pathogenesis, and current preventative measures. Dermatol Surg. 2015;41(5):537-49.
12. Barbieri JS, Fix WC, Miller CJ, Sobanko JF, Shin TM, Howe N, et al. Variation in prescribing and factors associated with the use of prophylactic antibiotics for Mohs surgery: A single-institution retrospective study. Dermatol Surg. 2019. Epub 2019 Oct 1.
13. Rossi AM, Mariwalla K. Prophylactic and empiric use of antibiotics in dermatologic surgery: a review of the literature and practical considerations. Dermatol Surg. 2012;38(12):1898-921.
14. Wright TI, Baddour LM, Berbari EF, Roenigk RK, Phillips PK, Jacobs MA, et al. Antibiotic prophylaxis in dermatologic surgery: advisory statement 2008. J Am Acad Dermatol. 2008;59(3):464-73.
15. Thornton JF, Griffin JR, Constantine FC. Nasal reconstruction: an overview and nuances. Semin Plast Surg. 2008;22(4):257-68.
16. Rohrich RJ, Griffin JR, Ansari M, Beran SJ, Potter JK. Nasal reconstruction--beyond aesthetic subunits: a 15-year review of 1334 cases. Plast Reconstr Surg. 2004;114(6):1405-16; discussion 1417-9.
17. Padoveze EH, Cernea SS. Reconstruction of nasal defects after tumor excision through Mohs micrographic surgery. Surg Cosmet Dermatol 2013;5(2):116-120.
18. Wollina U, Bennewitz A, Langner D. Basal cell carcinoma of the outer nose: overview on surgical techniques and analysis of 312 patients. J Cutan Aesthet Surg. 2014;7(3):143-50.
19. Cerci FB. Versatility of advancement flaps for nasal reconstruction following Mohs` micrographic surgery. An Bras Dermatol. 2018;93(5):719-22.
20. Cerci FB. Usefulness of the subunit principle in nasal reconstruction. An Bras Dermatol. 2017;92(5 Suppl 1):159-62.
21. Burget GC, Menick FJ. The subunit principle in nasal reconstruction. Plast Reconstr Surg. 1985;76(2):239-47.
22. Weathers WM, Koshy JC, Wolfswinkel EM, Thornton JF. Overview of nasal soft tissue reconstruction: keeping it simple. Semin Plast Surg. 2013;27(2):83-9.
23. Jacobs MA, Christenson LJ, Weaver AL, Appert DL, Phillips PK, Roenigk RK, et al. Clinical outcome of cutaneous flaps versus full-thickness skin grafts after Mohs surgery on the nose. Dermatol Surg. 2010;36(1):23-30.
24. Goldberg LH, Alam M. Horizontal advancement flap for symmetric reconstruction of small to medium-sized cutaneous defects of the lateral nasal supratip. J Am Acad Dermatol. 2003;49(4):685-9.
25. Wesley NO, Yu SS, Grekin RC, Neuhaus IM. Primary linear closure for large defects of the nasal supratip. Dermatol Surg. 2008;34(3):380-4; discussion 384-5.
26. Konofaos P, Alvarez S, McKinnie JE, Wallace RD. Nasal Reconstruction: A Simplified Approach Based on 419 Operated Cases. Aesthetic Plast Surg. 2015;39(1):91-9.
27. Fader DJ, Wang TS, Johnson TM. Nasal reconstruction utilizing a muscle hinge flap with overlying full-thickness skin graft. J Am Acad Dermatol. 2000;43(5 Pt 1):837-40.
28. Cerci FB. Comparison of paramedian forehead flap with nasolabial interpolation flap for nasal reconstruction after Mohs micrographic surgery. Surg Cosmet Dermatol. 2018;10(3):2016-24.
29. Cerci FB, Nguyen TH. Paramedian forehead flap for complex nasal defects following Mohs micrographic surgery. Surg Cosmet Dermatol. 2014;6(1):17-24.
30. Jellinek NJ, Nguyen TH, Albertini JG. Paramedian forehead flap: advances, procedural nuances, and variations in technique. Dermatol Surg. 2014;40(Suppl 9):S30-42.
31. Guzman AK, Bhatt MD, Sobanko JF, Etzkorn JR, Shin TM, Cosulich MT, et al. Intrasubunit V-Y Muscle Sling Myocutaneous Island Advancement Flap for Small Defects Isolated to the Nasal Ala. Dermatol Surg. 2019. Epub 2019 Oct 1.
32. Neltner SA, Papa CA, Ramsey ML, Marks VJ. Alar rotation flap for small defects of the ala. Dermatol Surg. 2000;26(6):543-6.
33. Tan E, Mortimer N, Salmon P. Full-thickness skin grafts for surgical defects of the nasal ala - a comprehensive review, approach and outcomes of 186 cases over 9 years. Br J Dermatol. 2014;170(5):1106-13.
34. Pipitone MA, Gloster HM, Jr. Repair of the alar groove with combination partial primary closure and second-intention healing. Dermatol Surg. 2005;31(5):608-9.
35. Cerci FB, Nguyen TH. Nasolabial interpolation flap for alar reconstruction after Mohs micrographic surgery. Surg Cosmet Dermatol 2014;6(2):113-20.
36. Nguyen TH. Staged cheek-to-nose and auricular interpolation flaps. Dermatol Surg. 2005;31(8 Pt 2):1034-45.
37. Feng H, Feng PW, Geronemus RG. Diversity in the US Mohs Micrographic Surgery Workforce. Dermatol Surg. 2019. Epub 2019 Aug 6.
38. Albertini JG, Wang P, Fahim C, Hutfless S, Stasko T, Vidimos AT, et al. Evaluation of a Peer-to-Peer Data Transparency Intervention for Mohs Micrographic Surgery Overuse. JAMA Dermatol. 2019. Epub 2019 May 5.
39. Alam M, Ibrahim O, Nodzenski M, Strasswimmer JM, Jiang SI, Cohen JL, et al. Adverse events associated with mohs micrographic surgery: multicenter prospective cohort study of 20,821 cases at 23 centers. JAMA Dermatol. 2013;149(12):1378-85.
40. Merritt BG, Lee NY, Brodland DG, Zitelli JA, Cook J. The safety of Mohs surgery: a prospective multicenter cohort study. J Am Acad Dermatol. 2012;67(6):1302-9. Epub 2012 Aug 11.
41. Locke MC, Davis JC, Brothers RJ, Love WE. Assessing the outcomes, risks, and costs of local versus general anesthesia: A review with implications for cutaneous surgery. J Am Acad Dermatol. 2018;78(5):983-8.e4.
42. Alam M, Schaeffer MR, Geisler A, Poon E, Fosko SW, Srivastava D. Safety of Local Intracutaneous Lidocaine Anesthesia Used by Dermatologic Surgeons for Skin Cancer Excision and Postcancer Reconstruction: Quantification of Standard Injection Volumes and Adverse Event Rates. Dermatol Surg. 2019;42(12):1320-1324.
43. Alam M, Helenowksi IB, Cohen JL, Levy R, Liègeois N, Mafong EA, et al. Association between type of reconstruction after Mohs micrographic surgery and surgeon-, patient-, and tumor-specific features: a cross-sectional study. Dermatol Surg. 2013;39(1 Pt 1):51-5.
44. Vasilakis V, Nguyen KT, Klein GM, Brewer BW. Revisiting Nasal Reconstruction After Mohs Surgery: A Simplified Approach Based on the Liberal Application of Local Flaps. Ann Plast Surg. 2019;83(3):300-4.
45. Chen EH, Johnson TM, Ratner D. Introduction to flap movement: reconstruction of five similar nasal defects using different flaps. Dermatol Surg. 2005;31(8 Pt 2):982-5.
 All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773
All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773



 Read in Portuguese
Read in Portuguese
 Portuguese PDF
Portuguese PDF
 Print
Print
 Send this article by email
Send this article by email
 How to cite this article
How to cite this article
 Submit a comment
Submit a comment
 Mendeley
Mendeley
 Pocket
Pocket
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}