


Francisco Ronaldo Moura Filho1; Gabriela Della Ripa Rodrigues Assis2; Livia Sampaio Pereira1; Thais Helena Buffo1; Hamilton Ometto Stolf1,3
Received on: 10/12/2019
Approved on: 10/02/2020
Financial support: None
Conflict of interests: None
Study conducted at the Universidade Estadual de Campinas, Campinas (SP), Brazil
Isolated keloid treatment has variable and often unsatisfactory results. The combination of therapies has proven to be an effective alternative mainly for recalcitrant cases. Surgical excision and immediate postoperative electron beam irradiation is an effective alternative in healing and reducing the recurrence rate of these lesions. The authors describe a patient with recalcitrant bulky keloid who had a good therapeutic outcome.
Keywords: Ear; Keloid; Radiotherapy
Keloids are benign lesions resulting from a posttraumatic fibrous proliferation of the skin. They result from excessive deposition of collagen in the extracellular matrix during the healing process. Morphologically, they are characterized by cellular hyperplasia due to the presence of intrinsically normal polyclonal fibroblasts that respond to an abnormal extracellular signal. Such injuries can be disfiguring and cause physical discomforts such as pain, burning, and itching. Also, they can restrict movement and form local fistulas after repeated infections and, consequently, affect the patient’s quality of life.1, 2
Isolated surgical treatment has a high recurrence rate, around 50-80%, which makes the use of adjuvant therapies necessary. The most used are cryotherapy, laser therapy, compression, and intralesional injection of corticosteroids, with variable results. Currently, a treatment established in resistant or refractory keloids is surgical excision followed by electron beam radiotherapy (RT). Recurrence rates for the first year are as low as 10% in some cases, and a typical protocol is excision followed by the first radiotherapy session, with ten or more subsequent sessions. Dosage and timing differ between teams and institutions.2, 3
The use of electron RT adjuvant to surgical treatment is based on the fact that, once the keloid is formed, it is not radiosensitive. Under these circumstances, the fibrous tissue will undergo little or no change with irradiation. However, fibroblasts from recent scars are highly radiosensitive.1, 3 We report the case of a recalcitrant keloid in which surgical treatment with adjuvant electron beam RT was employed successfully.
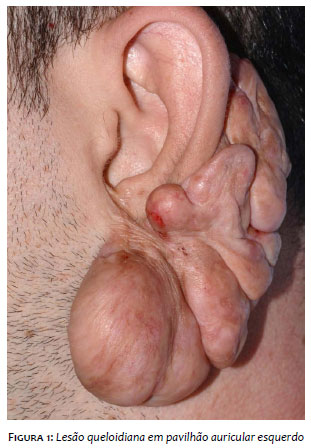
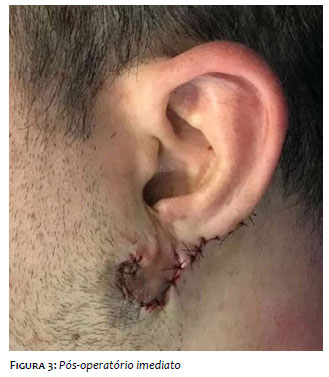
A 31-year-old man presented a large keloid lesion, approximately 15cm in the longest axis, originating from the left auricle and occupying the entire ipsilateral retroauricular portion (Figures 1 and 2). The condition began when he was 11 years old after trauma. The patient reported that he had already undergone several treatments, including five primary closure surgical approaches, two electrocoagulation surgeries and secondary intention closure, and beta-therapy after one of the surgical approaches at 14 years of age. Among the surgical procedures, he performed infiltrations with intralesional corticosteroids, and, despite the numerous treatments, he presented recurrence with progressive growth. In April 2018, he underwent a new surgical approach with a total lesion excision (Figure 3).
We opted for therapeutic complementation with electron beam RT, which started in the immediate postoperative period. The parameters used were: electron beam generated by a linear accelerator, 9 MeV energy (millions of electron volts = electron beam energy unit), 208 um/time, 100 source-to-surface distance (SSD), use of cone 10 for field delimitation, 100 cm source-to-surface distance, and daily dose of 200 centiGrays (cGy). Ten applications were performed, with a total dose of 2,000 cGy, and the sessions were distributed over two weeks, daily, except on weekends.
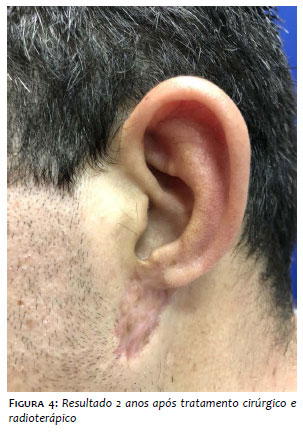
As an adverse event, the patient presented with beard and hair alopecia in the irradiated area, with complete repilation after the end of the sessions. The patient remains in follow-up, with good aesthetic and functional results and no evidence of relapse after 1 year of therapy (Figure 4).
There are several treatments available for keloids, and all of them alone have high recurrence rates, including surgical treatment that presents rates close to 100% in some studies. Among the adjuvant treatments employed, radiotherapy is highly effective, less likely to recur, and one of the primary forms used are brachytherapy and electron beam therapy.1-5
The biological action of irradiation on fibroblasts is inhibition of proliferation and stimulation of differentiation of these cells.6
Adjuvant RT modalities for operated keloids are: conventional X-ray,7 beta-therapy,1 single dose RT,8 and electron beam RT.9 Electron beam RT is superior to traditional X-ray irradiation for the treatment of keloids due to better tissue dose distribution.7
There is no consensus as to the best modality to be used or the total dose to be employed. Studies of meta-analysis and systematic review indicate that the most effective total doses of radiotherapy would be between 20 and 40 gray (Gy) (in the reported case the total dose was 20 Gy) and that there is proximity to recurrence rates between brachytherapy (12% in one year) and electron beam therapy (9% in one year), but this would have fewer adverse events such as hyperchromia and telangiectasia.1- 5
A comparative study between electron beam radiotherapy and beta-therapy following keloid surgery with 10-year follow-up showed better electron beam efficacy (77% good and optimal for electron therapy versus 46%). % for beta-therapy) and this result is attributed to better radiation dose distribution in the tissues with the electron beam.1
Among the RT modalities, the electron beam is the only one that allows a more homogeneous distribution, considering the irregularity of the lesion depth. When the electron beam comes from linear accelerators, a better energy distribution occurs, being more suitable for each thickness to be irradiated.10
The association of surgery and radiotherapy with the electron beam in the immediate postoperative period proved to be a well-tolerated therapeutic modality, with minimal undesirable events, and no, corroborating some cases in the literature.
We thank Dr. Antônio Carlos Zuliani de Oliveira for conducting the radiotherapy and joint follow-up of the case with the Dermatology Service.
Francisco Ronaldo Moura Filho | ORCID 0000-001-8275-9384
Approval of the final version of the manuscript; preparation and writing of the manuscript; intellectual participation in propaedeutic and/or therapeutic conduct of studied cases; critical literature review; critical revision of the manuscript.
Gabriela Della Ripa Rodrigues Assis | ORCID 0000-0001-5236-2554
Preparation and writing of the manuscript; active participation in research orientation; intellectual participation in propaedeutic and/or therapeutic conduct of studied cases.
Livia Sampaio Pereira | ORCID 0000-0003-1317-6104
Preparation and writing of the manuscript; active participation in research orientation; intellectual participation in propaedeutic and/or therapeutic conduct of studied cases; critical literature review.
Thais Helena Buffo | ORCID 0000-0002-6833-7596
Approval of the final version of the manuscript; preparation and writing of the manuscript; intellectual participation in propaedeutic and/or therapeutic conduct of studied cases; critical literature review; critical revision of the manuscript.
Hamilton Ometto Stolf | ORCID 0000-0003-4867-0276
A of the final version of the manuscript; preparation and writing of the manuscript; intellectual participation in propaedeutic and/or therapeutic conduct of studied cases; critical literature review; critical revision of the manuscript.
1. Oliveira Júnior B, Lastoria JC, Pereira HR, Silveira LVA, Oliveira LP, Stolf HO. Estudo comparativo entre o tratamento radioterápico com elétrons e betaterapia, após cirurgia de queloides. Surgical & Cosmetic Dermatology. 2009;1(2):53-57.
2. Duan Q, Liu J, Luo Z, Hu C. Postoperative brachytherapy and electron beam irradiation for keloids: A single institution retrospective analysis. Mol Clin Oncol. 2015;3(3):550-554.
3. Capel AV, Palop JV, Olive AP, Fernandez ASR. Adjuvance in refractory keloids using electron beams with a spoiler: Recent results. Rep Pract Oncol Radiother. 2014;20(1):43-49.
4. Mankowski P, Kanevsky J, Tomlinson J, Dyachenko A, Luc M. Optimizing Radiotherapy for Keloids: A Meta-Analysis Systematic Review Comparing Recurrence Rates Between Different Radiation Modalities. Ann Plast Surg. 2017;78(4):403-411.
5. Shen J, Lian X, Sun Y, Wang X, Hu K, Hou X, et al. Hypofractionated electron-beam radiation therapy for keloids: retrospective study of 568 cases with 834 lesions. J Radiat Res. 2015;56(5):811-817.
6. Trott KR. Therapeutic effects of low radiation dose. Strahlenther Onkol. 1994;170(1):1-12.
7. Maarouf M, Schleicher U, Schmachtenberg A, Ammon J. Radiotherapy in the management of keloids. Clinical experience with electron beam irradiation and comparison with X-ray therapy. Strahlenther Onkol. 2002;178(6):330-5.
8. Ragoowansi R, Cornes PG, Moss AL, Glees JP. Treatment of keloids by surgical excision and immediate postoperative single-fraction radiotherapy. Plast Reconstr Surg. 2003;111(6):1853-9.
9. Akita S, Akino K, Yakabe A, Imaizumi T, Tanaka K, Anraku K, et al. Combined surgical excision and radiation therapy for keloid treatment. J Craniofac Surg. 2007;18(5):1164-9.
10. Oliveira Júnior B, Schellini SA, Lastória JC, Carvalho LR, Stolf HO, Oliveira ALP. Tratamento de queloides usando radioterapia pós-operatória com elétrons: estudo comparativo e randomizado com dois esquemas. Surgical & Cosmetic Dermatology. 2013;5(1):16-26.
 All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773
All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773



 Read in Portuguese
Read in Portuguese
 Portuguese PDF
Portuguese PDF
 Print
Print
 Send this article by email
Send this article by email
 How to cite this article
How to cite this article
 Submit a comment
Submit a comment
 Mendeley
Mendeley
 Pocket
Pocket
{kind=link}
{kind=link}
{kind=link}
{kind=link}