


Bruna Laís Wedig; Fernando Eibs Cafrune
Received on: 12/11/2019
Approved on: 12/03/2020
Financial support: None
Conflict of interests: None
Study conducted at the Irmandade da Santa Casa de Misericórdia de Porto Alegre, Porto Alegre, RS, Brazil
INTRODUCTION: Lentigo maligna is a subtype of melanoma in situ, which affects sun-exposed areas. On the face, it can have a clinical and dermoscopic appearance similar to several benign pigmented lesions. Differential diagnosis between them is fundamental for the appropriate therapeutic and should be made by histopathological analysis. Excisional biopsy is the gold standard, but in large, unresectable lesions or in difficult anatomical sites, it can have aesthetic or functional implications. In these cases, shave biopsy appears to be a safe and reliable alternative.
OBJECTIVE: To describe an appropriate shave biopsy technique, discuss its results and indications in the outpatient routine of the dermatologist.
METHODS: Sixteen patients with suspected : Lentigo maligna on the face and scalp were selected. Inclusion criteria were older than 18 years, lack of diagnosis and previous treatment, flat lesions larger than 8 mm and suggestive clinical and dermatoscopic signs. The approach performed was shave biopsy.
RESULTS: The diagnosis of : Lentigo maligna was confirmed in 25% of the cases, and a widening of margins presented compatible results in 100% of them.
CONCLUSIONS: Shave biopsy seems to be a suitable alternative for flat lesions without clinical and dermoscopic criteria of vertical growth.
Keywords: Acne Vulgaris; Diclofenac; Inflammation; Hyperpigmentation
The term “melanoma in situ” was first used in 1949 by Lever, but it was only in 1992 that this classification was officially recognized as a diagnostic category for melanomas.1 In melanoma in situ, neoplastic cells are confined to the epidermis and the adnexal epithelium, not exceeding the basal layer of these structures.2
Among the melanomas in situ, lentigo maligna (LM) affects areas of intense sun damage, preferably head and neck, with a peak incidence between 65 and 80 years of age.2 It represents one of the clinical and pathological forms of melanomas in situ and may have a prolonged evolution, up to several decades, before evolving to its invasive form, lentigo maligna melanoma (LMM).3
Lentigo maligna presents, from the clinical point of view, as a macule with irregular, poorly-defined edges, varied pigmentation with asymmetrical distribution, and slow growth.3 Its appearance can be very similar to other pigmented lesions of the face, whether benign, such as seborrheic keratoses and solar lentigo; pre-malignant, such as actinic keratoses; and malignant, such as pigmented basal cell carcinoma. The differentiation between these entities is of great importance for the planning of the therapeutic approach.
Dermoscopy is a non-invasive complementary exam that helps in the differential diagnosis between these lesions. Dermoscopic criteria indicative of LM are rhomboidal structures, irregular pseudonetwork with asymmetrical follicular openings, slate-gray granularity, and blots.3
However, in most cases, the definitive diagnosis of pigmented lesions depends on histopathological analysis. The ideal biopsy technique should be easy and quick (to facilitate generalized application), be associated with minimal morbidity, allow precise staging of lesions considered to be malignant, and do not compromise oncological results in the long term.4 Excisional biopsy is regarded as the gold standard for the possibility of extensively assessing the removed tissue and accurately defining cell atypia and the presence or absence of basement membrane invasion, Breslow index, and other prognostic factors involved in melanocytic neoplasms. However, there are some cases in which it can cause a significant aesthetic and functional damage, as in large, unresectable pigmented lesions and in places that are difficult to approach, such as the face. In these cases, incisional biopsy guided by dermoscopy has been considered as the recommended initial approach.
The incisional punch biopsy is widely used, and its main advantages are its ease of execution and the potential to provide accurate information on the T stage, as it usually extends to subcutaneous fat and encompasses the base of the primary tumor. However, it is generally performed with small punch sizes, 3 mm or 4 mm, and the largest tools available for its performance measure 6 mm to 8 mm. In larger lesions, it may not cover the entire periphery of the injury. Thus, it can lead to diagnostic errors by preventing the analysis of essential criteria such as symmetry, overall size, and circumscription of the tumor, or even underestimating the actual invasion of the tumor by sample error if it does not include the deeper portion of the lesion.4
Incisional biopsy by shaving, or shave biopsy, which is the target of our study, seems to be superior to punch biopsy in the initial evaluation of superficial and extensive pigmented lesions.5 This type of technique is quick and practical and can be performed in the dermatologist’s office under local anesthesia, allowing a higher tissue sampling without compromising functionally or aesthetically.
This study aims to describe the proper shave biopsy technique, discuss its results and indications for the initial approach on pigmented lesions on the face in the outpatient routine of the dermatologist.
This is a pilot study. Sixteen patients were selected at the Dermatology outpatient clinics of the Santa Casa de Misericórdia in Porto Alegre between May and October 2019 with suspected lentigo maligna on the face and scalp. The lesions were previously assessed by dermoscopy, and the criteria used for the selection included patients aged over 18 years old, without previous diagnosis and treatment, with the presence of flat pigmented lesions, larger than 8 mm, and with dermoscopic signs suggestive of LM.
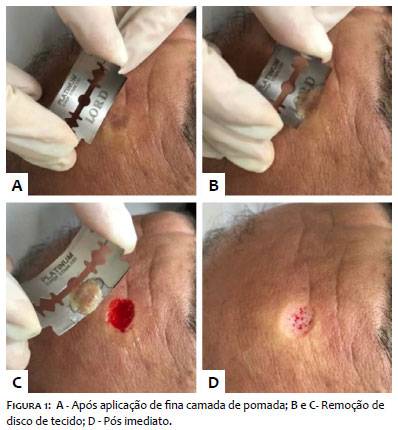
The biopsy technique used was deep shaving or shave biopsy, as shown below (Figure 1). The technique consists of asepsis, infiltration of local anesthetic, application of a thin layer of ointment on the lesion to firm the tissue (due to the availability in our service, we used mupirocin), followed by the removal of a disc of tissue using a scalpel or curved razor blade. It produced a sample extending to the upper dermis or the mid-dermis, depending on the angle of the blade. Hemostasis was performed with the application of aluminum chloride and a compressive dressing for 24 hours.
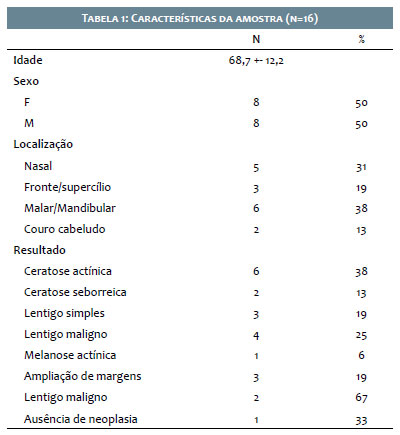
Our study selected 16 patients aged 36 to 87 years, with flat-pigmented lesions on the face and scalp suggestive of lentigo maligna. All of them underwent the shave biopsy. Table 1 summarizes the results.
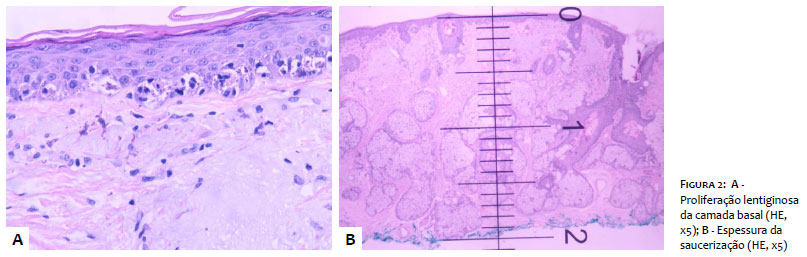
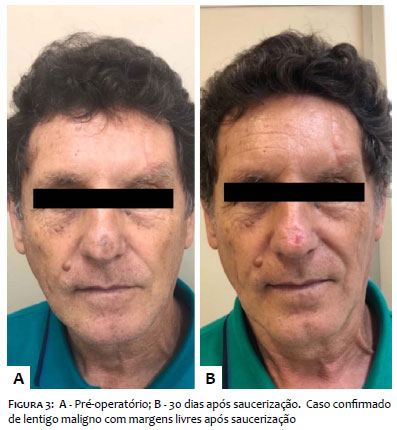
The diagnosis of lentigo maligna was confirmed in 4 patients. Of these, 3 underwent margin enlargement, and post-enlargement histopathology was compatible with the initial diagnosis in all cases. The fourth patient is undergoing clinical follow-up, as he presented deep and peripheral margins free of lesion already in the initial approach. Figure 2 represents the histopathological diagnosis, and Figure 3 illustrates the postoperative evolution, with a satisfactory aesthetic result.
The analysis of the data suggests that the shave biopsy appears to be a safe and reliable alternative in the initial approach of flat-pigmented lesions with suspected melanoma in situ. Histopathological analysis after margin enlargement confirmed the initial diagnosis or didn’t find residual neoplasia in 100% of the cases, a fundamental data for the safety of using the technique since one of the main concerns of this type of approach is the underestimation of the Breslow index by transection of the tumor base.6
These results are in line with those was seen by Pariser et al.7 in their study, which assessed the quality of the materials collected by excisional, punch, deep, and superficial shaving biopsies, with considerable superiority of the material obtained by deep shave biopsy in comparison to punch and superficial shave biopsies, and certainty of histological diagnosis similar to cases submitted to excision.5
Also, the results of our study confirmed that several benign pigmented lesions are part of the differential diagnosis of melanoma, and reinforce the relevance of more conservative initial approaches in prime areas to reduce functional and/or aesthetic sequelae.
Excisional biopsy with narrow margins is the most appropriate initial approach for pigmented lesions suspected of lentigo maligna. Although, it is not practical for most cases of extensive injuries since it requires more time and cost to be performed, in addition to technical difficulties for professionals without experience in advanced dermatological surgery. Incisional biopsies are routinely performed on large pigmented lesions, located in prime areas or by professionals who are not specialized in surgery, or who do not have a favorable environment for the appropriate excision of the lesion. Shave biopsy appears to be an adequate technical alternative for flat lesions without evidence of vertical growth. In addition to being performed quickly and having excellent aesthetic results, it presents an adequate tissue sample, diagnostic accuracy, and the possibility of safety assessment of the deep margins of flat lesions.
I thank the professors, colleagues, and patients who made this work possible.
Bruna Laís Wedig | ORCID 0000-0003-1143-7462
Statistical analysis; approval of the final version of the manuscript; data collection, analysis, and interpretation; preparation and writing of the manuscript; critical literature review; critical revision of the manuscript.
Fernando Eibs Cafrune | ORCID 0000-0002-6645-0122
Approval of the final version of the manuscript; study design and planning; data collection, analysis, and interpretation; active participation in research orientation; intellectual participation in propaedeutic and/or therapeutic conduct of studied cases; critical literature review; critical revision of the manuscript.
1. Gomes CS, Barroso IFGP, Dutra TBS, Obadia DL, Fracaroli TS. Lentigo maligna on the face: a challenging conduct. Rev Bras Oftalm. 2017;76(3):161-4.
2. Wainstein AJA, Belfort FA. Melanoma: prevenção, diagnóstico, tratamento e acompanhamento. 2nd ed. São Paulo: Atheneu; 2014.
3. Samaniego E, Redondo P. Lentigo maligno. Actas Dermosifiliogr. 2013;104(9):757-75.
4. Zager JS, Hochwald SN, Marzban SS, Francois R, Law KM, Davis AH, et al. Shave Biopsy Is a Safe and Accurate Method for the Initial Evaluation of Melanoma. J Am Coll Surg. 2011;212(4): 454-60.
5. Mir M, Chan CS, Khan F, Krishnan B, Orengo I, Rosen T. The rate of melanoma transection with various biopsy techniques and the influence of tumor transection on patient survival. J Am Acad Dermatol. 2012;68(3):452-8.
6. Swetter SM, Tsao H, Bichakjian CK, Curiel-Lewandrowski C, Elder DE, Gershenwald JE, et al. Guidelines of care for the management of primary cutaneous melanoma. J Am Acad Dermatol. 2019;80(1):208-250. Epub 2018 Nov 1.
7. Pariser RJ, Divers A, Nasser A. The relationship between biopsy technique and uncertainty in the histopathologic diagnosis of melanoma. Dermatol Online J. 1999;5(2):4.
 All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773
All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773



 Read in Portuguese
Read in Portuguese
 Portuguese PDF
Portuguese PDF
 Print
Print
 Send this article by email
Send this article by email
 How to cite this article
How to cite this article
 Submit a comment
Submit a comment
 Mendeley
Mendeley
 Pocket
Pocket
{kind=link}
{kind=link}
{kind=link}
{kind=link}