


Gisele Viana de Oliveira1; Lara Rodrigues de Morais Gambogi Alvarenga2; Petra Maria de Oliveira Duarte Stuhr3; Thiago A. Cantaruti4; Álida Rosária Silva Ferreira5; Gregory Thomas Kitten6
Received on: 20/02/2020
Approved on: 08/03/2020
Financial support: None
Conflict of interests: None
Study conducted at the Ambulatório de tratamento de Queloides e Cicatrizes hipertróficas, Hospital das Clínicas, UFMG, Belo Horizonte. O ambulatório funciona atualmente no Hospital Mario Penna, Belo Horizonte, MG.
Introduction: Silicone dressings and Triamcinolone injections are known to improve keloids and hypertrophic scars size, erythema, flexibility, and symptoms such as pain and itching. These treatments are non-invasive, inexpensive, and widely used as first or second-line therapy; however, studies comparing them are still lacking.
Objective: To compare silicone dressings, triamcinolone injections, and a combination group, to treat hypertrophic scars, at the same anatomical area, caused by the same mechanism of injury.
Materials and methods: In a prospective study, 12 patients with median-sternotomy scars were randomized into 3 groups (n=4 patients each): group 1, monthly triamcinolone injections; group 2, a combination of silicone dressings and triamcinolone injections; and group 3, silicone dressings. Patients were evaluated in monthly clinical appointments using the Vancouver Scale and the durometer. Immunohistochemistry and confocal microscopy for collagen types I and VI were performed in scar samples. The groups were compared using Kruskal-Wallis and Friedman tests, with p<0,05 indicating significance.
Results: The three treatments were effective in reducing the Vancouver scores. A difference between the three groups was observed at time 2 when triamcinolone was less effective. Group 2 showed an improvement on pigmentation (p = 0,042). Collagens types I and VI presented increased fluorescence throughout the superficial and deep dermis in untreated lesions, which decreased after the treatment. Although the number of patients is limited, this is the first prospective study addressing some of the major bias in scars treatment.
Keywords: Scar; Keloid; Silicone gel; Triamcinolone
Since the first reports on the use of silicone gel dressings in hypertrophic scars and keloids in 19831, several authors have shown that this noninvasive treatment modality improves scar size, pliability, erythema, pain, and itching2 by increasing skin hydration and occlusion3. Since silicone dressings are relatively inexpensive, noninvasive, and have very mild side effects, they have become one of the first-line treatments for keloids and hypertrophic scars.
Intralesional corticosteroid injections are also used to treat keloids and hypertrophic scars, with the first reports in 19604. There are few randomized studies on their use in keloids, but broad medical consensus has led physicians to consider corticosteroid injections as first- or second-line therapy for keloids and hypertrophic scars4. Triamcinolone has been the most commonly used corticosteroid among the several employed for injection in scars4.
Studies on keloid and scar treatment are complicated by several variables5,6, including the lack of a suitable animal model7 and the few objective methods to rate scars that could otherwise be readily available in physicians’ offices and outpatient clinics8. In addition, scars on different sites of the body or caused by different mechanisms of injury are frequently combined in the studies, although the comparison of such lesions may not be appropriate.
This prospective, controlled, randomized, unblinded, singlecenter study aimed to compare the efficacy of silicone dressings versus triamcinolone injections versus both (combination treatment) on keloidal or hypertrophic median sternotomy scars.
The study was approved by the Institutional Review Board of the Federal University of Minas Gerais and registered with the Brazil Platform (protocol number 06580513700005149). A detailed letter on potential study participants was sent to Cardiac Surgery Hospitals in Belo Horizonte, Minas Gerais State, Brazil, as well as to the Brazilian Society of Cardiology, Minas Gerais Regional Chapter.
1. Patient referral. Patients came to our service referred by the cardiology centers that received the invitation letter. Only patients who met the inclusion criteria were accepted for the study. During the first appointment, the study was explained to the patient, who signed a written informed consent form previously approved by the IRB. All patients received assurance that they would be able to follow with new treatment offered by the study’s medical team after the last study appointment at six months, at no cost to the patient.
Inclusion criteria: age 18-80 years at the start of the study; male or female gender; patients who agreed to and signed written consent to participate in the study. Exclusion criteria: pregnancy, severe asthma that could lead to use of corticosteroids for longer than two months; patients who had used intralesional steroids or radiation to treat their keloids; and age under 18 or over 80 years. Only patients who had scars with pain and itching or that were red, raised, and with keloidal features (starting to grow outside the original surgical scar) were accepted for the study. Patients with scars that were not considered hypertrophic or with lesions that were shrinking were not enrolled in the study.
2. Study groups. A random table was generated before the study began. Each patient was randomly assigned to one of the three study arms: group 1. intralesional triamcinolone injections (20 mg/ml), performed once a month for 6 months (total of 6 injections); the injections were performed along the entire scar at 1 cm intervals, at approximately 1-2 mm from the scars surface, with 0.05-0.1 ml per injection site; group 2. a combination group, combining triamcinolone injection and occlusive silicone dressing; group 3. occlusive silicone gel dressing, used 24 hours a day. Patients were advised to keep the silicone sheets on 24 hours a day, 7 days a week, removing the dressings every 7 days during their shower. The silicone sheets were then rinsed with water and left to dry on top of a glass surface for an hour, and then reapplied to the scar. The scar was washed once a week with soap and water during the shower.
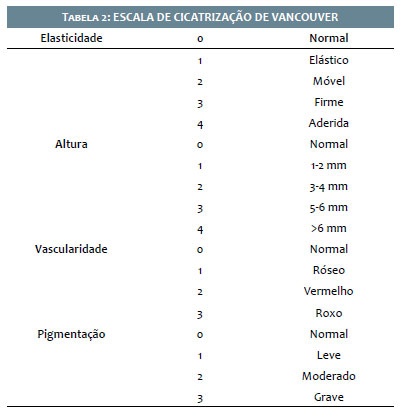
3. Patient evaluation during clinical appointments. Each patient was evaluated in clinical appointments on day one, before receiving any treatments, and then once a month, by the same physician. Patients were asked to come to the hospital after remo-ving the dressings at home. The Vancouver parameters were rated using the modified Vancouver Scar Scale 910. An objective measurement of the pliability was then performed with a durometer (Rex Gauge, 1000, Rex Gauge Company, IL, USA), as described elsewhere 11. The most hypertrophic area of the scar was chosen for evaluation, and that same area was evaluated in each of the monthly appointments. When two areas of the scar were considered clinically very severe and it was unfeasible to choose between them, the mean value for the two scars was used.
4. Silicone group. The silicone dressing (Medgel, Silimed, RJ, Brazil) was applied over the entire scar, as previously described3. Because the dressing is adherent but has no glue (it is not adhesive), it was attached with the help of microporous surgical tape covering the entire silicone dressing and extending 1 cm beyond the dressing on each side. The patient was instructed to keep the dressing in place for the next seven days, without removing it when showering. If patients performed intense phy-sical exercise or felt itching or sweating on the treated area, they were instructed to remove the tape, rinse both the skin and the silicone sheet, and place the dressing back on 2-3 hours later. Patients received the physicians telephone number in order to contact the medical team whenever necessary. After seven days, the patient removed the dressing during the shower, rinsed both the dressing (with cold water) and the scar area, and replaced the dressing. According to the manufacturers package insert, the product was expected to last 2 to 4 months. Since patients appeared for monthly appointments, the silicone dressing was replaced whenever it changed color, appeared dirty, or lost its adherent properties. After 3 months, if the dressing began to deteriorate and release small fragments, it was also replaced.
5. Triamcinolone injections. Triancil® (20 mg/ml, Apsen Laboratory) was administered in monthly injections along the entire scar at 1-centimeter intervals. An insulin needle was used, connected to a 1 ml insulin syringe, and a total volume of 0.050.1 ml was injected in each injection site. Areas that improved over time did not receive subsequent injections. Patients that developed itching after the injections received oral prednisolone 20 mg, 4 hours prior to the next procedure.
6. Biopsy, immunohistochemistry, and confocal microscopy for collagen types I andVI: A 3 mm skin biopsy was performed on patients that agreed to the procedure (one patient from each group). Biopsies were performed on the same patient at baseline (before treatment) and at the 6-month appointment (last study day). The specimen was collected, rinsed with saline solution, and placed in a cold cryo-substitute solution (80% methanol/20% DMSO) in vials that were submersed in dry ice, as previously described (12). After deparaffinization and rehydration, three consecutive sections, 5 micrometers thick, were blocked for one hour with 1% bovine serum albumin (Vector Laboratories, Burlingame, CA) and incubated overnight at 4oC with a polyclonal primary antibody for collagen I or collagen VI at a dilution of 1:200 (Rockland Immunochemicals®, PA). On the following day, Alexa Fluor 488 conjugated goat anti-rabbit IgG was used as secondary antibody (Molecular Probes®, Eugene, OR) and cell nuclei were labelled with 4,6-diamidino-2-phenylindole (DAPI) (Molecular Probes®, Carlsbad, CA). The images were captured with a confocal laser scanning microscope (Zeiss 880META®, Oberkochen, Germany) at 16 bits and analyzed in the gray-scale range of 0-255 using Image Tool® 3.0 Software. Images were captured at 40X magnification and analyzed by an expert morphologist, trained in both immunohistochemistry and confocal skin collagen images, and who was also blind to the study groups.
Statistics. The data were submitted to a normality test and detected as non-parametric distribution. The three groups were compared using the Kruskal-Wallis test, and the evaluation from baseline to 6 months was performed with the Friedman test. Significance for all tests was p< 0.05.
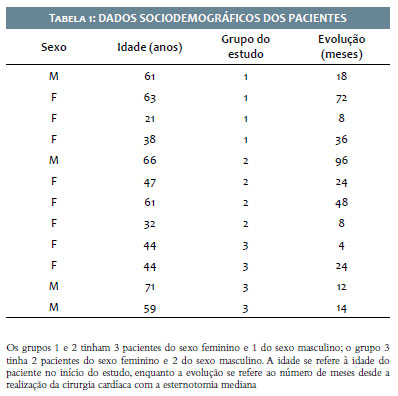
Twelve patients who met the inclusion criteria were en-rolled in the study, four in each group. Patients 1-14 were randomly assigned to the 3 study groups. At that point, group 1 had only 2 patients, so the last 2 patients enrolled in the study were assigned to group 1. All patients were seen monthly and completed the study. Groups 1 and 3 had 1 male and 3 female patients, while group 2 had 2 male and 2 female patients. 33.3% of the study patients were males, and 66.7% were females (Table 1. Patient Demographics). The keloids were located on the chest. The mechanism of injury that had led to keloid formation was cardiac surgery. Table 1 shows the study participants’ demographics.
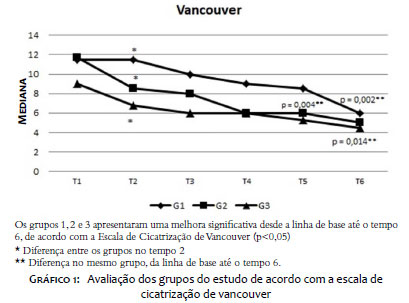
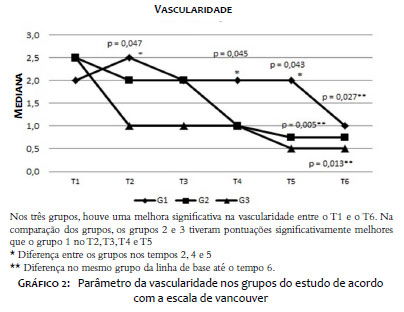
Vancouver Scar Scale (Table 2). According to the Vancouver Scar Scale, all the groups improved from baseline to 6 months (p < 0.05): Group 1 (p = 0.002), Group 2 (p = 0.004), and Group 3 (p = 0.014 - Graph 1). When the three groups are compared at each time point, groups 2 and 3 showed more improvement than group 1, mainly in terms of vascularity (at times 2, 4, and 5, there was a statistically significant difference between group 1, which had higher degrees of vascularity, and groups 2 and 3, with lower vascularity- Graph 2).
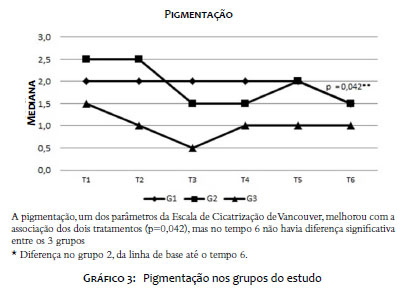
Pigmentation. Evaluation over time showed that group 2 improved significantly in the pigmentation parameter (p = 0.042) (Graph 3).
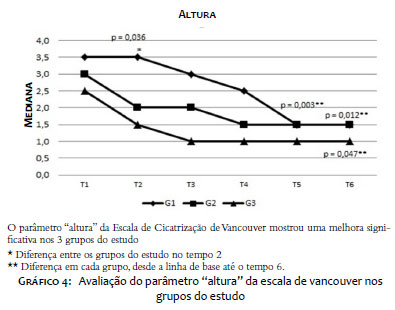
Scar height. When the three study groups were compared at each of the timepoints, group 1 showed the worst improvement at time 2, when compared to groups 2 and 3 (p=0.036). Analysis over time showed significant reduction in scar height in the three groups- group 1 (p = 0.003), group 2 (p = 0.012), and group 3 (p = 0.047) (Graph 4).
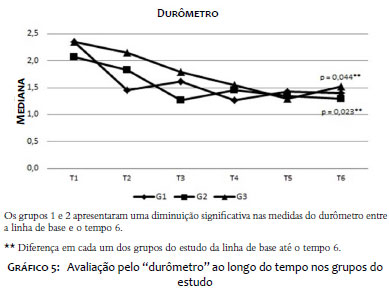
Durometer. From baseline to 6 months, group 1 (p = 0.044) and group 2 (p = 0.023) showed a significant decrease in the durometer grades, while no difference was seen in group 3. When the three groups were compared at each study time, no significant differences were observed (Graph 5).
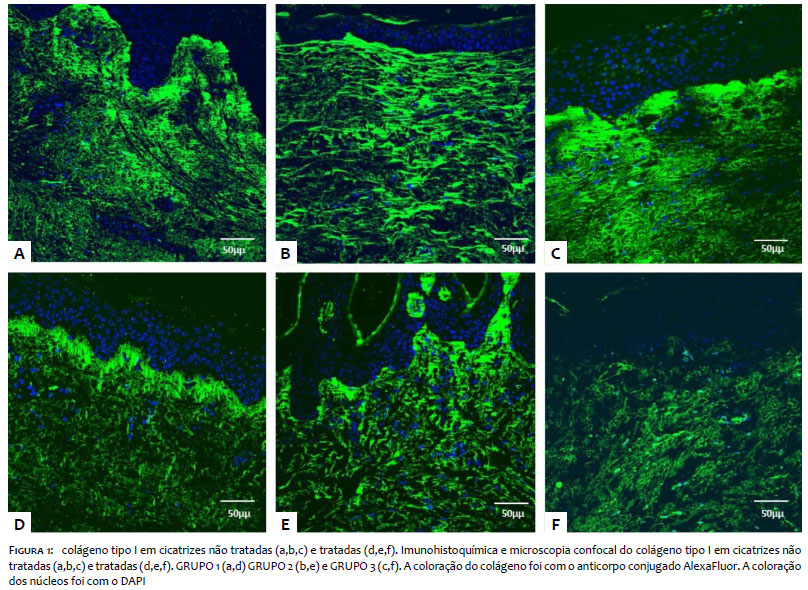
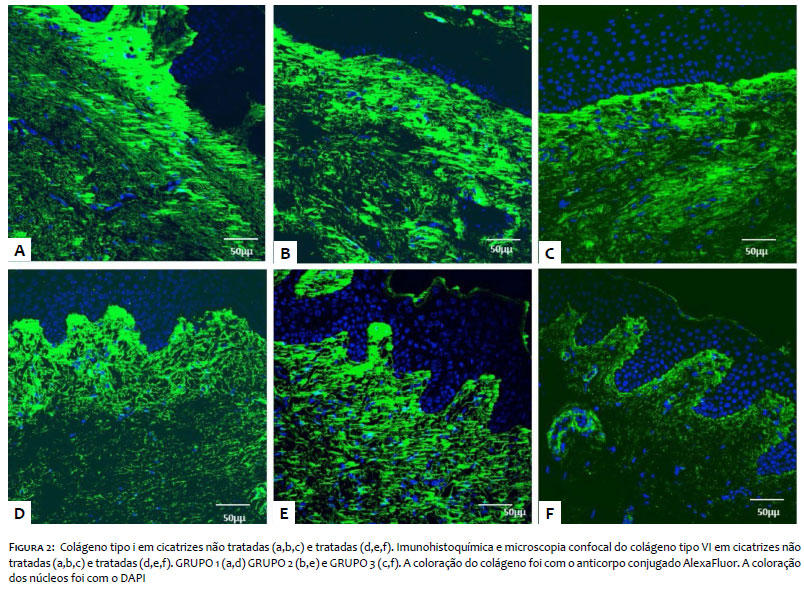
Immunohistochemistry. Type I collagen. Although there were 4 patients in each group, only one patient from each group agreed to submit to skin biopsy. The 3-mm skin biopsy was performed before the treatment started and was repeated in the same patient at 6 months. Type I collagen was distributed throughout the dermis, with stronger expression seen in the upper dermis. When the scar was treated, type I collagen expression decreased throughout the dermis, mainly in deeper layers, and greater contrast was seen in treated scars in the upper and lower layers. Less variation was seen in untreated scars, suggesting that type VI collagen deposition may increase in deeper layers of untreated keloids (Figure 1). Type VI collagen. Type VI collagen distribution occurred throughout the dermis, following a similar distribution pattern to that seen in type I collagen. However, type VI collagen expression appeared to be stronger in the upper dermis of untreated scars, when compared to type I Collagen, and greater variation was seen between the upper and lower dermal layers (Figure 2).
Silicone dressings improved scar pliability when applied to the scar tissue 12-24 hours a day for 6 months (3). The scar tissue became softer, allowing better diffusion of intralesional steroids (13). There is a lack of controlled studies in scars, comparing silicone dressings to other treatments. In some studies, other methods were associated, such as excision and triamcinolone injections (8, 13, 14, 15 e 16), thus making it difficult to evaluate the effect of the silicone itself (17). In order to address this issue, we designed a study with previously untreated patients who only used each study groups specific treatment. There is widespread agreement that silicone dressings promote hypertrophic scar/keloid improvement by increasing hydration and occlusion (3). Other possible mechanisms of action in the improvement of keloids with silicone include limiting skin stretching during healing (18) and increasing temperature, hydration, and oxygen tension (19). We have previously shown that occlusive dressings, including silicone and non-silicone sheets, lead to complete or partial improvement of physical parameters in scars and keloids. (3). The low cost and very low risk of side effects have led der-matologists to consider silicone and non-silicone dressings as first-line treatment for keloids and hypertrophic scars (3). We believe that the protocol for silicone gel dressing can also positively impact the outcome, since we found that scars treated with silicone sheets applied 24 hours a day, 7 days a week (dressings were only removed once a week to wash the skin and scar area) showed better outcomes (data not shown).
Corticosteroids have been used since 1960 to treat keloids and scars (4), and triamcinolone is the most commonly used corticoid for this purpose (4). Corticosteroids can inhibit collagen synthesis by reducing inflammation and fibroblast proliferation and increasing hypoxia (20). Steroids also reduce plasma protease inhibitors, allowing collagen degradation (21). They also increase basic fibroblast growth factor (bFGF) and decrease transforming growth factor-® (TGF-HI1) by dermal fibroblasts, endogenous vascular endothelial growth factor (VEGF), and insulin-like growth factor-1 (IL-1) (4). Roques & Teot (2008) suggest three mechanisms to explain how corticosteroids improve keloids: suppression of inflammation and cell migration; vasoconstriction; and antimitotic effect on keratinocytes and fibroblasts (4). The scars response to intralesional steroids varies from 50% to 100%, with recurrence rates ranging from 9% to 50% (22). There is no consensus among clinicians regarding the dose, frequency, and duration of treatment. Adverse effects include hypopigmentation, skin and subcutaneous tissue atrophy, telangiectasias, ulcerations, and Cushings syndrome (4). Robles et al. (2007) recommend triamcinolone acetonide at concentrations ranging from 10 to 40 mg/mL, in monthly injections (23). A review in 2016 evaluated the efficacy of corticosteroid injections in keloids and hypertrophic scars, comparing the technique to other treatment modalities such as silicone gel, verapamil, and antineoplastic drugs (24). Our study showed that triamcinolone injections alone were less effective in the initial treatment, as measured by vascularity. However, at 6 months, no significant differences were observed when lesions treated with triamcinolone were compared to silicone dressings. When triamcinolone injections were associated with silicone sheets, no significant improvements were identified in our study (although we call attention to the studys small sample size).
The Vancouver Scar Scale was the first attempt to standardize scar assessment by different observers. Pigmentation, pliability, height, and vascularity were scored, and the sum of the scores was higher in more hypertrophic scars (4). The Vancouver scale became a generally accepted clinical scar assessment tool in most scar treatment centers (5). Several attempts have been made to improve the scoring system, adding objectivity to scale parameters (4,6,7). In the current study, we added the durometer assessment. ‘‘Pliability’’, a term that refers to the elastic texture of the skin and scar, is one of its parameters. To assess pliability, the observer must touch the skin or scar surface, limiting its use only for clinical assessments (4). The durometer has been shown to adequately correlate with Vancouver pliability scores (11). We found that the durometer is affordable and easy to handle, due to its small size. Durometers have been used to assess the skins hardness in leg ulcers, morphea, and scleroderma (25, 26).
Immunohistochemistry with confocal laser scanning microscopy has several advantages over scanning electron microscopy and conventional optical microscopy. Single tissue layer scanning eliminates the errors that occur in regular fluorescence microscopy as the result of variations in the thickness of histological sections. It allows for a precise evaluation of collagen distribution in skin layers and helps understand differences in expression among the various layers (12).
Type I collagen is a cellular matrix protein dermal collagen seen in the dermis of normal skin and scars. We have previously shown that its expression is increased in more hypertrophic scars (12, 27) when compared to normal skin and non-hypertrophic scars. Non-hypertrophic scars display type I collagen expression that is more similar to normal skin. In the present study, notwithstanding the small sample size, we also found that treated scars (less hypertrophic) are prone to decreasing type I collagen expression.
Type VI collagen is a key regulator of dermal matrix assembly, composition, and fibroblast behavior and may play an important role in wound healing and tissue regeneration (28). Its distribution is similar to collagen types I and III, and it has been shown to be located in the upper dermis of keloids (29). Our study found stronger type VI collagen staining in the upper dermis of the scar. We also showed that untreated lesions displayed increased type VI collagen when compared to the same scar after treatment. Although our study was limited by the small number of patients, the decreased expression of type VI collagen appears to correlate with the overall improvement of the keloid (Figure 2). To our knowledge, the is the first study to date that has shown type VI collagen expression in untreated and treated scars using immunohistochemistry staining and confocal microscopy. New studies with larger numbers of patients are needed to confirm this result.
Variables that act as confounding factors in scar and keloid studies include: the lack of prospective, randomized study designs; subjective methods for scar evaluation; and the hetero-geneity of scars caused by different mechanisms of injury and in different anatomical regions, and that have been grouped together for comparison. Many of the studies include scars previously treated with drugs and methods with prolonged effects, such as corticosteroids, antineoplastic drugs, or radiotherapy (3, 11). The present study attempted to rule out such potential confounders by including only patients with pre-sternal scars, all caused by the same mechanism of injury (cardiac surgery). Patients who had received previous treatments were excluded. Because we aimed to adhere to very strict inclusion criteria, few patients were enrolled in the study, which we consider a limitation. However, we feel that the study will provide guidance for a future and much larger multicenter study. We call attention to the difficulties in obtaining larger groups of patients with scars caused by the same mechanism of injury and on the same body area, The motivated the creation of GREMCIQ- the Brazilian Group for Multicenter Studies of Keloids and Hypertrophic Scars. The group includes dermatologists from different regions of Brazil, with the main goal promoting collaboration in the development of multicenter studies to improve the understanding of treatments for keloids and hypertrophic scars in a highly mixed racial population, prone to the development of such lesions.
This study was made possible thanks to the efforts of Professor Bernardo Gontijo, MD, PhD, who implemented the Outpatient Clinic for the Treatment of Keloids and Hypertrophic Scars at the University Hospital, UFMG (accredited by the Brazilian Society of Dermatology), and to whom the authors owe the deepest gratitude and respect.
The study was conducted at the Dermatology Outpatient Clinic at the University Hospital of the Federal University of Minas Gerais (UFMG), initial home to the Outpatient Clinic for Treatment of Keloids and Hypertrophic Scars. The clinic has now moved to Hospital Mario Penna, Belo Horizonte, MG. Immunohistochemistry and confocal microscopy were performed at CEMEL (Electronic Microscopy Center) of the ICB (Institute of Biological Sciences), UFMG. The study did not receive any financial support.
Gisele Viana de Oliveira | 0000-0001-5101-7097
Principal investigator.
Lara Rodrigues de Morais Gambogi Alvarenga | 0000-0001-8727-4159
Data collection.
Petra Maria de Oliveira Duarte Stuhr | 0000-0002-8455-8372
Data collection.
Thiago A. Cantaruti | 0000-0001-7339-1581
Data collection, IHC and capture of confocal microscopy images.
Álida Rosária Silva Ferreira | 0000-0001-9972-1796
Statistical analysis.
Gregory Thomas Kitten | 0000-0002-4044-9932
Data collection, supervision of IHC and confocal microscopy.
1. Perkins K, Davey RB, Wallis KA. Silicone gel: a new treatment for burn scars and contractures. Burns Incl Therm Inj. 1983;9(3):201-4.
2. Ahn ST, Monafo WW, Mustoe TA. Topical silicone gel: a new treatment for hypertrophic scars. Surgery. 1989;106(4):781-6; discussion 786-7.
3. de Oliveira GV, Nunes TA, Magna LA, Cintra ML, Kitten GT, Zarpellon S, Raposo Do Amaral CM. Silicone versus non-silicone gel dressings: a controlled trial. Dermatol Surg. 2001;27(8):721-6.
4. Roques C, Téot L. The use of corticosteroids to treat keloids: a review. Int J Low Extrem Wounds. 2008;7(3): 137-45.
5. McGrouther DA. Hypertrophic or keloid scars? Eye (Lond). 1994;8( Pt 2):200-3.
6. Carney SA, Cason CG, Gowar JP, Stevenson JH, McNee J, Groves AR, Thomas SS, Hart NB, Auclair P. Cica-Care gel sheeting in the management of hypertrophic scarring.Burns. 1994;20(2):163-7.
7. Clugston PA, Vistnes MD, Perry LC, Maxwell GP, Fisher J. Evaluation of silicone- gel sheeting on early wound healing of linear incisions. Ann Plast Surg. 1995;34(1):12-5.
8. Ahn ST, Monafo WW, Mustoe TA. Topical silicone gel for the prevention and treatment of hypertrophic scar. Arch Surg. 1991;126(4):499-504.
9. Baryza MJ, Baryza GA. The Vancouver Scar Scale: an administration tool and its interrater reliability. J Burn Care Rehabil. 1995;16(5):535-8.
10. Yeong EK, Mann R, Engrav LH, et al. Improved burn scar assessment with use of a new scar-rating scale. J Burn Care Rehabil. 1997;18(4):353- 5; discussion 352.
11. Oliveira GV, Chinkes D, Mitchell C, Oliveras G, Hawkins HK, Herndon DN. Objective assessment of burn scar vascularity, erythema, pliability, thickness, and planimetry. Dermatol Surg. 2005;31(1):48-58.
12. de Oliveira GV, Sanford AP, Murphy KD, de Oliveira HM, Wilkins JP, Wu X, Hawkins HK, Kitten G, Chinkes DL, Barrow RE, Herndon DN. Growth hormone effects on hypertrophic scar formation: a randomized controlled trial of 62 burned children. Wound Repair Regen. 2004;12(4):404- 11.
13. Fulton JE Jr. Silicone gel sheeting for the prevention and management of evolving hypertrophic and keloid scars. Dermatol Surg. 1995;21(11):947-51.
14. Hirshowitz B, Lindenbaum E, Har-Shai Y, Feitelberg L, Tendler M, Katz D.Static-electric field induction by a silicone cushion for the treatment of hypertrophic and keloid scars. Plast Reconstr Surg. 1998;101(5):1173-83.
15. Kavanagh GM, Page P, Hanna MM. Silicone gel treatment of extensive hypertrophic scarring following toxic epidermal necrolysis. Br J Dermatol. 1994;130(4):540-1.
16. Aköz T, Erdogan B, Görgü M, Deren O. Combined approach to the treatment of earlobe keloids. Plast Reconstr Surg. 1998;101(3):857-8.
17. Cruz-Korchin NI. Effectiveness of silicone sheets in the prevention of hypertrophic breast scars. Ann Plast Surg. 1996;37(4):345-8.
18. Ogawa R. The most current algorithms for the treatment and prevention of hypertrophic scars and keloids. Plast Reconstr Surg. 2010;125(2):557–568.
19. Berman B, Perez OA, Konda S, Kohut BE, Viera MH, Delgado S, et al. A review of the biologic effects, clinical efficacy, and safety of silicone elastomer sheeting for hypertrophic and keloid scar treatment and management. Dermatol Surg. 2007;33(11):1291–1302
20. Gauglitz GG, Korting HC, Pavicic T, Ruzicka T, Jeschke MG. Hypertrophic scarring and keloids: pathomechanisms and current and emerging treatment strategies. Mol Med. 2011;17(1-2):113-25. Epub 2010 Oct 5. Review.
21. Niessen FB, Spauwen PH, Schalkwijk J, Kon M. On the nature of hypertrophic scars and keloids: a review. Plast Reconstr Surg. 1999;104(5):1435-58.
22. Mustoe TA, Cooter RD, Gold MH, Hobbs FD, Ramelet AA, Shakespeare PG, et al. International clinical recommendations on scar management. Plast Reconstr Surg. 2002;110(2):560-71.
23. Robles DT, Moore E, Draznin M, Berg D. Keloids: pathophysiology and management. Dermatol Online J. 2007;13(3):9.
24. Wong TS, Li JZ, Chen S, Chan JY, Gao W. The Efficacy of Triamcinolone Acetonide in Keloid Treatment: A Systematic Review and Meta-analysis. Front Med (Lausanne). 2016;3:71.
25. Aghassi D, Monoson T, Braverman I. Reproducible measurements to quantify cutaneous involvement in scleroderma. Arch Dermatol. 1995;131(10):1160-6.
26. Seyger MM, van den Hoogen FH, de Boo T, de Jong EM. Reliability of two methods to assess morphea: skin scoring and the use of a durometer. J Am Acad Dermatol. 1997; 37:793–6.
27. Oliveira GV, Hawkins HK, Chinkes D, Burke A, Tavares AL, Ramos-e-Silva M, Albrecht TB, Kitten GT, Herndon DN. Hypertrophic versus non hypertrophic scars compared by immunohistochemistry and laser confocal microscopy: type I and III collagens. Int Wound J. 2009;6(6):445-52.
28. Theocharidis G, Drymoussi Z, Kao AP, Barber AH, Lee DA, Braun KM, Connelly JT. Type VI Collagen Regulates Dermal Matrix Assembly and Fibroblast Motility. J Invest Dermatol. 2016;136(1):74-83.
29. Zhang LQ, Laato M, Muona P, Kalimo H, Peltonen J. Normal and hypertrophic scars: quantification and localization of messenger RNAs for type I, III and VI collagens. Br J Dermatol. 1994;130(4):453-9.
 All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773
All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773



 Read in Portuguese
Read in Portuguese
 Portuguese PDF
Portuguese PDF
 Print
Print
 Send this article by email
Send this article by email
 How to cite this article
How to cite this article
 Submit a comment
Submit a comment
 Mendeley
Mendeley
 Pocket
Pocket
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}