


Giovana Binda1; Raíssa Rigo Garbin1; Fernando Eibs Cafrune2
Received on: 10/06/2018
Approved on: 02/12/2019
Financial support: None
Conflict of interests: None
Research conducted at Complexo Hospitalar Santa Casa de Misericórdia de Porto Alegre, Porto Alegre (RS), Brazil.
The Keystone flap is a versatile and reliable option for the reconstruction of major defects, especially those located in the lower limbs. With its use, there is a low risk of necrosis, being a way to avoid the use of a graft. We report the case of a 92-year-old female patient who was submitted to the Keystone flap after Mohs surgery for pre-tibial Bowen's disease treatment, with good evolution. The Keystone flap is based on musculocutaneous and fasciocutaneous perforators, has high flap survival rates, low risk of complications, reduced pain and morbidity of the donor site, in addition to rapid patient recovery
Keywords: Perforator flap; Mohs surgery; Lower extremity
The repair of defects in the lower limbs is still challenging, since such defects often affect elderly patients with peripheral vascular insufficiency and lack of tissue laxity, which poses greater risk of necrose. This anatomical characteristic and frequent exposure of bone and tendon hinder graft viability. Primary or second-intention closure is recommended whenever possible, but when not possible, grafts and flaps are an option. Conventional muscle flaps were thus gradually replaced by perforator flaps, with less morbidity in the donor site.1 Keystone flap is a relatively new technique, described for the first time by Behan in 2003,2 providing an interesting option with a high success rate in these reconstructions. The name refers to the curving trapezoidal keystone shape in Roman arches. It is a fasciocutaneous flap with vascularization from perforating arterioles of muscle, useful for reconstructions in areas with poorly distensible skin such as the limbs and back.3
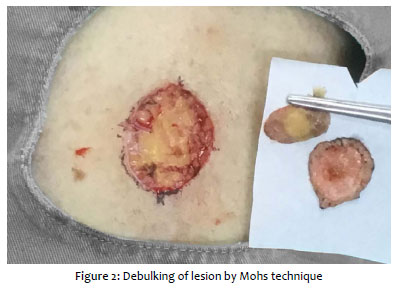
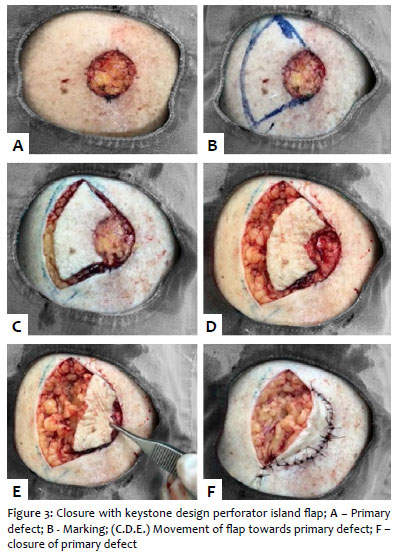
Female patient, 92 years, presented a hyperkeratotic nodular lesion measuring approximately 2cm in the largest diameter on the anterior aspect of the left leg, with biopsy showing in situ squamous cell carcinoma (Figure 1), without prior treatments. Patient was submitted to Mohs micrographic surgery and was tumor-free in the first stage (Figure 2). Primary closure used the keystone technique, with a curved strip the same width as the defect and with 90º angles at the corners of the tumor excision area. Advancing the flap on the primary defect results in a secondary defect that is longer and narrower. Perpendicular to the flap's advancement, the two peripheral edges were advanced in V-Y and the strip was advanced over the defect and sutured with 4.0 nylon (Figures 3 and 4).
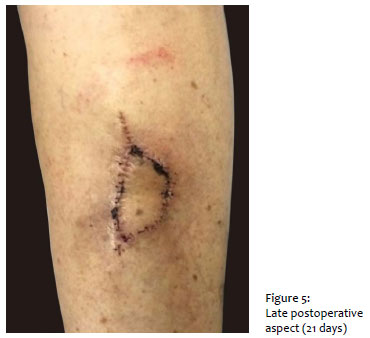
The patient presented good evolution, with no postoperative complications (Figure 5).
Keystone design perforator island flap (KDPIF) is an elliptical flap based on perforator vessels. It acts as a multi-perforator advancement flap requiring tissue laxity for the advancement.
The defect is closed directly, and the midline is the area with the greatest tension, and through the V-Y advancement of each extremity of the flap, the "island" strip fills the defect, allowing closure of the secondary defect on the opposite side.2 Its longitudinal orientation preserves the perforator arterioles and lymphatics, reducing the risk of distal lymphedema.4 The importance of blunt dissection is emphasized in raising these perforator island flaps, since it preserves the vascular integrity of the musculocutaneous and fasciocutaneous perforators, together with the venous and neural connections.5 Four types of this flap have been described: type I (direct closure), type II (with or without grafting), type III (double-island flap technique); and type IV (rotation and advancement with or without grafting).2 The keystone flap minimizes the need for skin grafting in the majority of cases and produces excellent aesthetic and functional results, with less postoperative pain and early mobilization.5 Therefore, this is a simple and effective method for surgical closure in situations that would otherwise require a more complex technique or skin graft. l
Giovana Binda | 0000-0002-9127-6736
Elaboration and writing of the manuscript; data collection, analysis, and interpretation; critical review of the literature.
Raíssa Rigo Garbin | 0000-0002-9771-1209
Elaboration and writing of the manuscript.
Fernando Eibs Cafrune | 0000-0002-6645-0122
Data collection, analysis, and interpretation; effective participation in the orientation of the study; critical revision of the manuscript.
1. Huang J, Yu N, Long X, Wang X. A systematic review of the keystone design perforator island. Flap in lower extremity defects. Medicine(Baltimore). 2017;96(21):e6842.
2. Behan FC. The keystone design perforator island flap in reconstructive surgery. ANZ J Surg. 2003;73(3):112-20.
3. Aragón-Miguel R, Gutiérrez-Pascual M, Sánchez-Gilo A, Sanz-Bueno, Vicente-Martin FJ. Aplicación del colgajo de keystone em dermatologia. Experiencia clínica em 18 pacientes. Actas Dermosifiliogr. 2018;109(6):515-520.
4. Abraham JT, Santi-Cyr M. Keystone and Pedicle Perforator Flaps in Reconstructive Surgery New Modifications an Applications. Clin Plastic Surg. 2017;44(2):385-402.
5. Hu M, Bordeaux JS. The keystone flap for the lower extremity defects. Dermatol Surg. 2012;38(3):490-3.
 All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773
All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773



 Read in Portuguese
Read in Portuguese
 Portuguese PDF
Portuguese PDF
 Print
Print
 Send this article by email
Send this article by email
 How to cite this article
How to cite this article
 Submit a comment
Submit a comment
 Mendeley
Mendeley
 Pocket
Pocket
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}