


Glaysson Tassara Tavares1; Carolina De Magalhães Ledsham2; Isabella Vieira De Oliveira2; Vanessa Martins Barcelos1
Received on: 24/01/2019
Approved on: 14/11/2019
Financial support: None
Conflict of interests: None
Research conducted at Hospital das Clínicas, Universidade Federal de Minas Gerais, Belo Horizonte (MG), Brazil.
A 77-year-old patient presents a case of primary cutaneous ductal eccrine carcinoma in the parietal region of the scalp. The biopsy showed a carcinoma with a ductal and infiltrative pattern, suggestive of metastatic neoplasia. An invasive carcinoma with eccrine tubular pattern was identified. The mastologist and oncologist did not detect primary lesions in other organs. Based on clinical and immunohistochemical analyses, the diagnosis was primary cutaneous eccrine carcinoma. Mohs micrographic surgery was performed with three phases to get a free margin. The tumor presented deep infiltration of the subcutaneous tissue and galea aponeurotica.
Keywords: Carcinoma, intraductal, noninfiltrating; Eccrine glands; Mohs Surgery
Sweat gland carcinomas (SGC) are rare tumors, accounting for approximately 0.05% of all cutaneous neoplasms 1, and are divided into apocrine and eccrine (more common).2 Ductal eccrine adenocarcinoma (DEC) affects individuals of both sexes from 50 to 80 years of age.2 It is generally described as an asymptomatic lesion with slow evolution. DEC presents great clinical variability and is located mainly on the scalp and cervical region. It presents metastases, in some 57% of cases3, to the regional lymph nodes, skin, lungs, and bones.2 Treatment is reported as excision with wide margins. Prognosis is reserved, with 70% recurrence3, while 10-year survival is 9% and 56% (whether lymph node positive or negative, respectively)4.
Ductal eccrine adenocarcinoma is clinically important due to the histological and immunohistochemical findings similar to secondary cutaneous metastases, especially from invasive ductal carcinoma of the breast, in addition to other adenocarcinomas, whose treatment and prognosis differ greatly. The differential diagnoses are squamous cell carcinoma, basal cell carcinoma, and Merkel cell carcinoma.5,6
This study reports a case of ductal eccrine carcinoma in which the differential diagnosis with cutaneous metastasis was challenging. Confirmation was only possible through the association of clinical, histological, and immunohistochemical data. The study further aims to demonstrate the importance of Mohs micrographic surgery (MMS) in this setting, since this neoplasm presents imprecise limits, a, factor that hinders obtaining free margins if treated with conventional surgery.
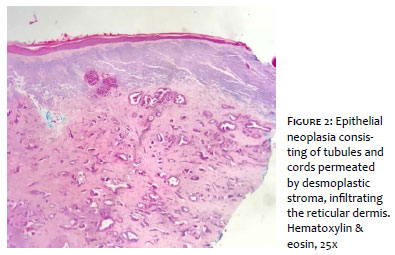
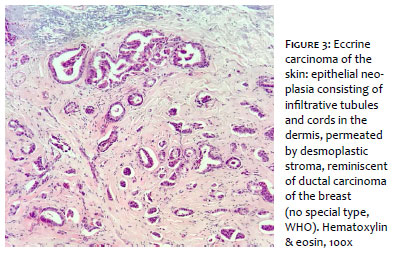
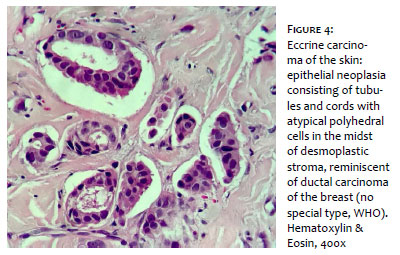
A 77-year-old male patient presented a history of an asymptomatic lesion on the scalp, which he had noticed 15 days before. Clinical examination revealed a subcutaneous nodule with alterations in the overlying skin, measuring 1.2 x 0.9cm in diameter, located on the right parietal region of the scalp (Figure 1). An incisional biopsy was performed, evidencing proliferation of atypical polyhedral cells with hyperchromatic/pleomorphic nuclei and evident nucleoli, forming niches, cords, and tubular arrangements in the midst of desmoplastic stroma (Figures 2, 3, and 4), suggestive of infiltrative ductal-pattern carcinoma, possibly metastatic neoplasia.
Immunohistochemistry was CK7 positive, EMA positive, diffusely ER (estrogen receptor) positive, CK20 negative, and WT1 negative, and the report was invasive carcinoma originating in the breast. Patient was referred to a mastologist and oncologist, who did not find malignant neoplasms, either in the breasts or in other organs.
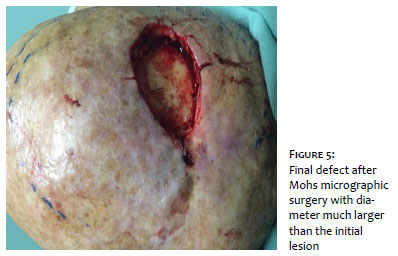
Excision of the lesion was performed with MMS. In the first stage, the initial margin was 5mm, and two more stages were necessary to obtain free margins (Figure 5). Histology showed ductal eccrine carcinoma, moderately differentiated, with deep infiltration of the subcutaneous tissue and galea aponeurotica, sparing the epidermis and superficial dermis.
Ductal eccrine adenocarcinoma presents findings on histology and immunohistochemistry that are quite similar to cutaneous metastases from adenocarcinomas, especially of the breast, making the differential diagnosis challenging.5,6
The clinical characteristics of these two entities are different: ductal eccrine adenocarcinoma presents as a single lesion, while metastasis from the breast commonly presents multiple lesions and association with history of breast cancer prior to the dermatological findings. Immunohistochemistry has been the focus of attention in recent studies to differentiate between SGC and cutaneous metastatic breast carcinoma.5,7
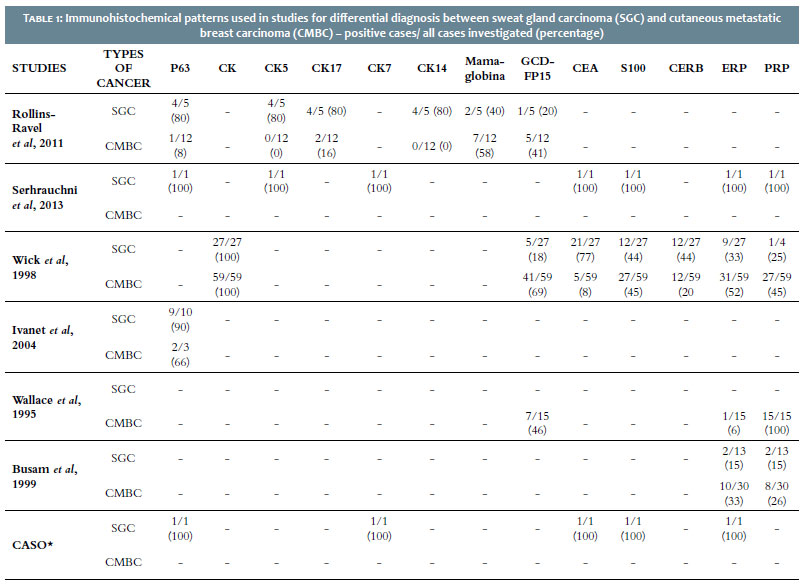
The diagnosis in this case was possible after ruling out an extracutaneous metastatic focus, by the presence of a single lesion on the scalp, associated with the immunohistochemical analysis. The findings in the two immunohistochemical studies were CK7+, P63+, CK18+, and CEA+. There is no evidence-based immunohistochemical pattern, given the tumor's rarity. However, in the existing studies, the presence of the above-mentioned markers favors a primary eccrine gland tumor and less frequently a cutaneous metastatic breast carcinoma, as shown in Table 1.
Other potential markers described in the literature for this distinction are GCDFP-15, EGFR, and podoplanin.8 Treatment with MMS proved essential due to the tumor's location in the deep dermis and subcutaneous tissue, the imprecise limits, and the absence of alterations in the epidermis and superficial dermis. At the end of MMS, the margin needed to obtain free margins was 9mm (three stages). Given the subclinical extent and the fact that this was a neoplasm with high relapse and metastasis rates, the Mohs surgical approach proved important to control the margins, thus reducing the risk of incomplete excision.
Glaysson Tassara Tavares | 0000-0002-1688-2955
Approval of the final version of the manuscript; conception and planning of the study; elaboration and writing of the manuscript; data collection, analysis, and interpretation; effective participation in the orientation of the study; intellectual participation in propaedeutic and/or therapeutic management of the cases; critical review of the literature; critical revision of the manuscript.
Carolina De Magalhães Ledsham | 0000-0003-4269-0049
Approval of the final version of the manuscript; elaboration and writing of the manuscript; data collection, analysis, and interpretation; critical review of the literature; critical revision of the manuscript.
Isabella Vieira De Oliveira | 0000-0002-0245-4941
Conception and planning of the study; elaboration and writing of the manuscript; critical review of the literature; critical revision of the manuscript.
Vanessa Martins Barcelos | 0000-0002-0087-271X
Conception and planning of the study; elaboration and writing of the manuscript; data collection, analysis, and interpretation; critical review of the literature.
1. Rollins-Raval M, Chivukula M, Tseng GC, Jukic D, Dabbs DJ. An immunohistochemical panel to differentiate metastatic breast carcinoma to skin from primary sweat gland carcinomas with a review of the literature. Arch Pathol Lab Med. 2011;135(8):975-83.
2. Leonhardt FD, Zanoni A, Ponce F, Haddad L, Scapulatempo Neto C, Cervantes O, Abrahao M. Carcinoma de glândula sudorípara écrino. Rev Bras Otorrinolaringol. 2007;73(2):286-7.
3. Matos D, Goulao J, Barreiros H, Bártolo E, Oliveira A, Sanches F, et al. Carcinoma Ductal Écrino. Rev Soc Portuguesa Dermatol Venereol. 2014;72(4):599-604.
4. McLean SR, Shousha S, Francis N, Lim A, Eccles S, Nathan M, et al. Metastatic ductal eccrine adenocarcinoma masquerading as an invasive ductal carcinoma of the male breast. J Cutan Pathol. 2007;34(12):934-8.
5. Wick MR, Ockner DM, Mills SE, Ritter JH, Swanson PE. Homologous carcinomas of the breasts, skin, and salivary glands. A histologic and immunohistochemical comparison of ductal mammary carcinoma, ductal sweat gland carcinoma, and salivary duct carcinoma. Am J Clin Pathol. 1998;109(1):75-84.
6. Brichkov I, Daskalakis T, Rankin L, Divino C. Sweat gland carcinoma. Am Surg. 2004;70(1):63-6.
7. Zehr KJ, Rubin M, Ratner L. Apocrine adenocarcinoma presenting as a large ulcerated axillary mass. Dermatol Surg. 1997;23(7):585-7.
8. DeVita Jr VT, Hellman S, Rosenberg SA. Cancer - Principles & Practice of Oncology. 7th Ed. Lippincott: Williams & Wilkins; 2000.
 All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773
All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773



 Read in Portuguese
Read in Portuguese
 Portuguese PDF
Portuguese PDF
 Print
Print
 Send this article by email
Send this article by email
 How to cite this article
How to cite this article
 Submit a comment
Submit a comment
 Mendeley
Mendeley
 Pocket
Pocket
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}