


Naja Cardoso Pereira de Santana1; Jürg Hafner2; Martin Kägi3
Received on: 04/08/2019
Approved on: 18/12/2019
Financial support: None
Conflict of interests: None
Study conducted at the Zurich University Hospital (Universitätsspital Zürich), Zurich, Switzerland.
Desmoplastic melanoma (DM) represents less than 4% of cutaneous melanomas and is characterized by invasive proliferation of spindle cells in the dermis, often with neurotropism. The nonspecific clinical appearance and the absence of pigmentation usually lead to a clinical misdiagnosis. The authors report a case of DM located in a cutaneous field cancerization simulating actinic keratosis.
Keywords: Melanoma; Immunohistochemistry; Histology
Cutaneous melanoma is a malignant neoplasm that originates in melanocytes, cells derived from the neural crest, and located at the dermo-epidermal junction.1,2 A rare variant, desmoplastic melanoma (DM), constitutes less than 4% of cutaneous melanomas and still represents a diagnostic challenge due to the clinical and histological similarity with other fibrous tissue neoplasms.2,3
Desmoplastic melanoma, first described by Conley et al4 in 1971, is characterized by the invasive proliferation of spindle cells in the dermis, with frequent involvement of deeper parts and with variable deposition of collagen in the stroma (desmoplasia).1,2,5DM often presents neurotropism, with a growth pattern similar to neuroma.1,6
The authors report a case of DM located on the scalp of a patient who had received several previous treatments, including radiation therapy, in the currently affected area.
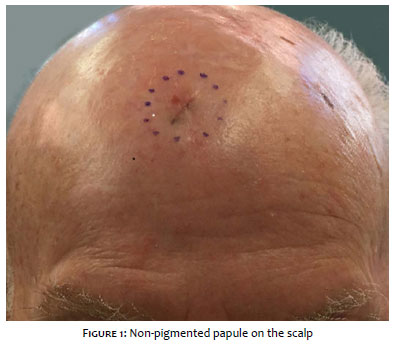
A 72-year-old white male patient attended the consultation for evaluation, with a two-month history of an asymptomatic, non-pigmented lesion on the scalp (Figure 1). The physical examination revealed a hard, poorly demarcated papule, measuring 7mm in diameter, located on the scalp, close to the frontal region.
The patient's clinical dermatological history is revealing. Four years ago, he was being followed up at the Dermatology Clinic due to multiple actinic keratoses, basal cell carcinomas, and Bowen's disease on the scalp. During this time, the patient underwent several therapies, including surgical procedure with total excision of basal cell carcinoma and Bowen's disease, treatment with ingenol mebutate gel, diclofenac sodium gel, CO2 laser, and photodynamic therapy. Also, he received radiotherapy sessions on the scalp five months before the lesion appeared. The total radiotherapy dose was 48 Gy (12 applications of 4 Gy) with 50Kv.
Recently, an incisional biopsy of the lesion had been performed, with an initial clinical diagnosis of actinic keratosis. Histopathological examination showed atypical spindle cells with invasion of the dermis and subcutaneous tissue, with immunohistochemical examination diffusely positive for S100, focally positive for HMB-45, and negative for Melan-A. The findings were suggestive of desmoplastic melanoma, and the patient was referred to the Department of Dermatology at the Zurich University Hospital.
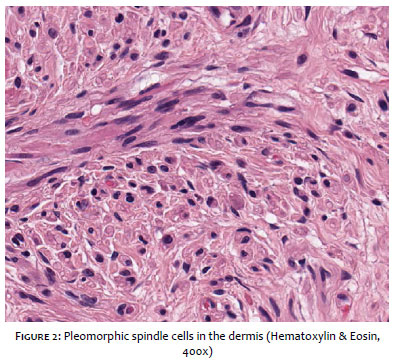
The patient was promptly submitted to emergency total excision with 8mm lateral margins. The new histopathological exam (Figure 2) confirmed the diagnosis of desmoplastic melanoma, with a Breslow index of 3.5mm, perineural invasion, and a surgical margin very close to the neoplastic involvement. The PET-CT conducted in the postoperative period did not show lymph node involvement or distant metastases. The patient underwent a new excision with a 2cm lateral margin and depth up to the periosteum, in addition to sentinel lymph node biopsy. Histopathological analysis showed no metastatic tumor in the sentinel lymph node. The patient remains under careful monitoring.
Most DMs present clinically as a firm nodule, papule, or painless plaque. Pigmentation is often rare or absent (between 44.3% and 73%).
The lesion is prevalent in elderly male individuals in areas with chronic sun exposure, particularly in the head and neck, and may also affect the mucous membranes and acral regions.2,3,5 DM presents a behavior different from other forms of melanoma, due to its tendency of local recurrence and lower rates of lymph node involvement.3,7 Our case is in line with the profile typically described in patients with DM.
Histologically, DMs are characterized by atypical spindle cells that invade the dermis and subcutaneous tissue, arranged in a single infiltrate or organized fascicles. Tumor cells exhibit varying degrees of neurotropism, and fibrotic stromas have varying patterns of desmoplasia. Intratumoral lymphocytic aggregates are frequent.1,5
DM can appear in the context of a precursor lesion, such as lentigo maligna, in 42% of cases.3 The histopathological classification of DM includes two subtypes, based on the degree of desmoplasia: pure DM and mixed DM. Pure DM tends to contain less clinically evident pigmentation, in addition to presenting prominent desmoplasia throughout the tumor (>90%) and less lymph node involvement. Mixed DM is more associated with lentigo maligna.2
Immunohistochemical studies are often necessary to assess the tumor thickness of the DM and differentiate it from non-melanocytic simulators. The most sensitive antigen for the diagnosis of DM is the protein S100, diffusely positive in most cases, although it is not specific to this nosological entity. The S100 protein does not distinguish DM from Schwann cell tumors. Most of the time, melanocytic differentiation antigens (HMB-45, gp100, Melan-A/Mart-1, tyrosinase, and MITF) are negative.2,3 Recent immunohistochemical studies have demonstrated the expression of SOX10 in malignant melanomas, including DM.8
In the genetic profile, DM shows a decrease in the number of genes involved in melanin synthesis, which may explain the fact that many of these lesions are amelanotic.9 Neurofibromin-1 is the most frequently mutated gene in DM and results in non-functional proteins.10
Dermoscopy has limited use due to the clinical subtlety of DM and the lack of data on dermoscopic features.2 Debarbieux et al. assessed six patients with DM, only three of whom had melanocytic structures. As for amelanotic lesions, the authors concluded that the presence of unstructured areas with a white scar-like appearance and abnormal vascular patterns are the main predictive characteristics of DM.11
At the time of diagnosis, most DMs are between 2.0 and 6.5mm thick, with Clark levels IV and V,2 characteristics that agree with the findings in our clinical case. Controversy persists regarding the prognosis of DM, compared to non-desmoplastic melanomas.2,3Carlson et al. found a higher five-year survival rate in DM tumors thicker than 4mm, compared to non-DM tumors thicker than 4mm (72% versus 37- 48%).12 A large case series, including tumors of all thicknesses, found a DM overall survival similar to that of patients with other cutaneous melanomas.13 The difficulty of distinguishing between pure and mixed DM may explain the conflicting reports in the literature on the disease biological behavior.14
The first line of treatment for primary cutaneous melanoma is surgical management. For lesions 1-2mm thick, margins of 1cm to 2cm are recommended, while for lesions over 2mm, margins of 2cm are indicated.1,15 Chen et al. prefer margins of at least 2cm in DM due to its local recurrence and neurotropism.2
Many authors question the routine recommendation for sentinel lymph node biopsy in DM, due to the low risk of lymph node involvement and uncertain benefits in terms of survival. Some authors suggest that biopsy can be considered in patients with neurotropism, high mitotic index, and ulceration.1, 2
Systemic metastasis occurs in 7% to 44% of DM cases, and the lung is the most affected organ.1,2,16,17 Local recurrence and histopathological type of DM are associated with increased risk of distant metastasis.2, 17 Compared to pure DM, patients with mixed DM have a 3.5 times greater risk of death or metastasis.14
Current guidelines are unclear regarding the precise role of radiotherapy (RT) in patients with DM. Some studies claim that adjuvant RT can be valid in DM patients at high risk of local recurrence18 or with locally recurrent DM, large residual tumors, DM with perineural involvement, or with narrow surgical margins.2 Vongtama et al. recommend postoperative adjuvant radiotherapy as part of DM treatment.19 Recent data suggest that adjuvant RT improves local control in patients with adverse characteristics, although it has no significant impact on overall five-year survival.20 In our case, although the patient had received radiation therapy at the site of the lesion's appearance before the diagnosis, we cannot say that RT was a paradoxical risk factor for DM.
Recently, researchers have shown that patients with locally advanced or metastatic DM have a high response rate to immunotherapeutic agents such as anti-PD1 and/or anti-PD-L1. Compared to non-DM melanomas, a higher expression of PD-L1 was observed in DM.17 Unlike cutaneous melanoma, genetic mutations such as BRAFV600E and c-KIT are rarely found in DM. It is still unclear whether systemic treatments such as vemurafenib and ipilimumab result in therapeutic success in DM.2
DM still represents a diagnostic challenge due to its clinical presentation. There is still much controversy on prognosis and the best therapeutic approach in these patients, including the role of radiotherapy. Further studies are needed to understand this rare variant of melanoma better.
Naja Cardoso Pereira de Santana | 0000-0003-0978-0616
Study design and planning; preparation and writing of the manuscript; critical literature review; critical revision of the manuscript.
Jürg Hafner | 0000-0002-4571-1143
Approval of the final version of the manuscript; active participation in research orientation; intellectual participation in propaedeutic and/or therapeutic conduct of studied cases; critical revision of the manuscript.
Martin Kägi | 0000-0002-5526-3145
Approval of the final version of the manuscript; study design and planning; active participation in research orientation; intellectual participation in propaedeutic and/or therapeutic conduct of studied cases.
1. Ferreira FR, Ferrari B, Acedo LMS, Ujihara JED, Lira MLA, Mandelbaum SH. Desmoplastic melanoma: a diagnostic challenge. Surg Cosmet Dermatol. 2015;7(2):184-7.
2. Chen LL, Jaimes N, Barker CA, Busam KJ, Marghoob AA. Desmoplastic melanoma: A review. J Am Acad Dermatol. 2013;68(5):825-33.
3. Paschoal FM, Yamada VL, Enokihara MMSS, Machado Filho CDS. Desmoplastic melanoma. Surg Cosmet Dermatol. 2012;4(1):1-7.
4. Conley J, Latterly R, Orr W. Desmoplastic malignant melanoma (a rare variant of spindle cell melanoma). Cancer. 1971;28(4):914-36.
5. Godoy GP, Gomes DQC, Pereira JV, Figueiredo RLQ, Nonaka CF, Miguel MCC. Desmoplastic melanoma of the lower lip: a case report. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 2009;108(5):e64-9.
6. Reed JG, Leonard DD. Neurotropic melanoma: a variant of desmoplastic melanoma. Am J Surg Pathol. 1979;3(4):301-11.
7. Jaroswewski DE, Pockaj BA, DiGaudo DJ, Bite U. The clinical behavior of desmoplastic melanoma. Am J Surg. 2001;182(6):590-5.
8. Tacha D, Qi W, Ra S, Bremer R, Yu C, Chu J, et al. A newly developed mouse monoclonal SOX10 antibody is a highly sensitive and specific marker for malignant melanoma, including spindle cell and desmoplastic melanomas. Arch Pathol Lab Med. 2015;139(4):530-6.
9. Busam K, Zhao H, Coit DG, Kucukgol D, Jungbluth AA, Nobrega J, et al. Distinction of desmoplastic melanoma from non - desmoplastic melanoma by gene expression profiling. J Invest Dermatol. 2005;124(2):412-8.
10. Wiesner T, Kiuru M, Scott SN, Arcila M, Halpern AC, Hollmann T, et al. NF1 Mutations Are Common in Desmoplastic Melanoma. Am J Surg Pathol. 2015;39(10):1357-62.
11. Debarbieux S, Ronger-Salve S, Dalle S, Balme B, Thomas L. Dermoscopy of desmoplastic melanoma: report of six cases. Br J Dermatol. 2008;159(2):360-3.
12. Carlson JA, Dickersin GR, Sober AJ, Barnhill RL. Desmoplastic neurotropic melanoma. A clinicopathologic analysis of 28 cases. Cancer. 1995;75(2):478-94.
13. Quinn MJ, Crotty KA, Thompson JF, Coates AS, O'Brien CJ, McCarthy WH. Desmoplastic and desmoplastic neurotropic melanoma: experience with 280 patients. Cancer. 1998;83(6):1128-35.
14. Busam KJ, Mujumdar U, Hummer AJ, Nobrega J. Hawkins WG, Coit DG, et al. Cutaneous desmoplastic melanoma: reappraisal of morphologic heterogeneity and prognostic factors. Am J SurgPathol. 2004;28(11):1518-25.
15. Bichakjian CK, Halpern AC, Johnson TM, Hood AF, Grichnik JM, Swetter SM, et al. Guidelines of care for the management of primary cutaneous melanoma. J Am Acad Dermatol. 2011;65(5):1032-47.
16. Lens MB, Newton-Bishop JA, Boon AP. Desmoplastic malignant melanoma: a systematic review. Br J Dermatol. 2005;152(4):673-8.
17. Ochoa EC, Joseph RW. Desmoplastic melanoma: a brief review and the efficacy of immunotherapy. Expert Rev Anticancer Ther. 2019;19(3):205-7.
18. Foote MC, Burmeister B, Burmeister E, Baley G, Smithers M. Desmoplastic melanoma: The role of radiotherapy in improving local control. ANZ J Surg. 2008;78(4):273-6.
19. Vongtama R, Safa A, Gallardo D, Calcaterra T, Juillard G. Efficacy of radiation therapy in the local control of desmoplastic malignant melanoma. Head Neck. 2003; 25(6):423-8.
20. Oliver DE, Patel KR, Switchenko J, Parker D, Lawson DH, Delman KA, et al. Roles of adjuvant and salvage radiotherapy for desmoplastic melanoma. Melanoma Res. 2016;26(1):35-41.
 All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773
All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773



 Read in Portuguese
Read in Portuguese
 Portuguese PDF
Portuguese PDF
 Print
Print
 Send this article by email
Send this article by email
 How to cite this article
How to cite this article
 Submit a comment
Submit a comment
 Mendeley
Mendeley
 Pocket
Pocket
{kind=link}
{kind=link}