


Khairuddin Djawad1; Amelia Setiawati Soebyanto1; Airin R. Nurdin1; Siswanto Wahab2; Anis Irawan Anwar3
Received on: 05/11/2019
Approved on: 25/11/2019
Financial support: None
Conflict of interests: None
Study conducted at the Department of Dermatology and Venereology, Medical School, Universitas Hasanuddin, Makassar, Indonesia.
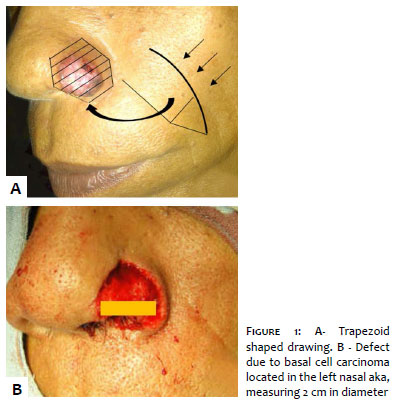
Reconstruction of the nasal area is a challenge due to its vascularization and abundance of fibrotic tissue. Graft in a large defect in the nasal area has a high risk of necrosis and often produces deformity and color mismatch. We report the case of a 65-year-old man with basal cell carcinoma in the left nasal ala. Mohs surgery was performed, obtaining free margin. The final defect measured 2 cm in diameter with partial loss of skin thickness. The combination of a melolabial interpolation flap and an ear cartilage graft was used, with excellent results. This combination led to good structural and aesthetic results.
Keywords: Surgical Flaps; Bone transplantation; Ear cartilage; Carcinoma, Basal cell
The nasal ala is a common area for skin cancer and often represents a challenge for cosmetic reconstruction after Mohs surgery.1 Frequently, the closure of a defect after the removal of a basal cell carcinoma in the nasal ala results in deformity due to the defect itself and/or invasion of the underlying tissue by tumor cells. Therefore, different techniques are needed to close the defect and preserve the anatomy of the nasal ala. One technique for maintaining the alar contour involves collecting auricular cartilage, which can to provide structural support for the nostril. The graft alone, to reconstruct a large defect in the nose, is not the treatment of choice, because it presents a high risk of necrosis,2 in addition to resulting in differences in pigmentation.3 Flaps are preferred, leading to more satisfactory results in terms of contour and colors.4 We report here a successful case of application of a melolabial interpolation flap in the reconstruction of a defect due to removal of basal cell carcinoma in the nasal ala.
A 65-year-old male patient, a farmer, was treated at the Dermatology Outpatient Clinic of Dr. Wahidin Sudirhusodo Hospital, South Sulawesi, Indonesia, with basal cell carcinoma confirmed by biopsy in the left nasal ala. The first step in the reconstructive surgery was the design of the nasolabial flap with a 4:1 length-to-width ratio. Aseptic and antiseptic procedures were performed under local anesthesia, and modified Mohs micrographic surgery was performed 5mm from the tumor margin, with a negative surgical margin. The final defect measured 2cm in diameter, with loss of the total thickness of the skin. We performed a medial interpolated flap in two stages, combined with an auricular cartilage graft used as an alar support structure.
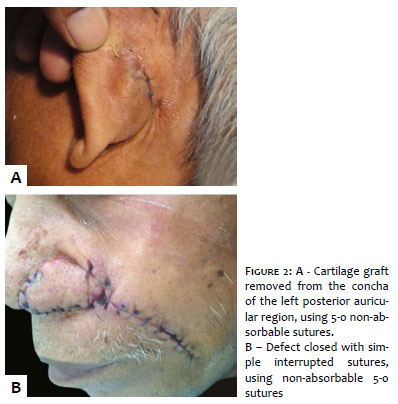
1st stage. Initially, the interpolation flap was designed, so the final suture was located in the melolabial groove. Two incisions were made up to the subcutaneous tissue, from the nasolabial fold to the tip of the previously demarcated flap. The lateral incision was made to leave a pedicle base of approximately 1.5cm, while the medial incision followed the nasolabial fold. The distal end of the flap was dissected to the base of the pedicle, with progressive depth, to separate it from the underlying fascia, ensuring generous vascularization, sufficient to supply the flap. The distal end should be less thick than the base of the pedicle, to compromise the vascularization. The pedicle was then rotated to cover the defect, with the border constituting the internal area of the nostril. Adequate transposition is required, and the pedicle should not be rotated more than 90 degrees to avoid affecting the nutrient vessels. The cartilage donor site was the left posterior auricular area (concha), measuring 0.7cm x 2cm, with sufficient auricular cartilage to provide structural support to the nasal ala and giving symmetry to the nostrils, in addition to a curvature similar to the nasal ala itself. The auricular cartilage was fixed with 5-0 mattress stitches (Figure 1). The flap was then rotated to cover the cartilage. After detaching the skin around the donor site, the two wounds (from the donor site and the reconstruction) were closed with simple 5-0 non-absorbable sutures (Figure 2). The sutures were removed from the nasal and ear wounds 10 days after surgery. The patient was then submitted to the second stage of surgery. The base of the flap was divided, and the defect was sutured with non-absorbable sutures. The proximal portion of the flap and the receiving area were gently trimmed before insertion. The flap was accommodated to fit the defect and then sutured. The success of the surgery was verified, with the symmetrical nasal ala and color similar to that of the neighboring tissue (Figure 3).
The nasal ala reconstruction has been a challenge for cosmetic repair due to the peculiar anatomy and the lack of skin tension in the area.5 Most of the nasal structure consists of connective tissue and sebaceous glands, but subcutaneous fat is lacking.6 Any defect in this area can seriously affect facial features. Geriatric patients have enough redundant malar tissue to allow the reconstruction of a nasal defect left by malignant cutaneous neoplasia up to 2.5cm wide. The choosing of the flap design is essential to minimize alar distortion.7
The nasolabial transposition flap is an excellent choice to close the defect, particularly in nasal ala 1.5-2.0cm in diameter.8 The melolabial region comprises the melolabial groove, from the nasal ala to the labial commissure, and the redundant malar tissue. Eventually, the flap is called "nasolabial", but the term "melolabial" is more anatomically accurate.9 The melolabial groove has skin that is sufficiently flaccid to cover the nasal ala, and the underlying fat has a strong tendency to contract.8 The location of the donor site, close to the surgical defect, supports the interpolated flap. It consists of a pediculated skin flap, based on the rotation of a skin fragment that ensures the irrigation. It is indicated for a defect in an area where there is insufficient skin that can be moved for closure or with lack of vascularization, particularly on cartilaginous or bone surfaces.10
The interpolated flap of the melolabial groove has a rich vascularization, including the angular artery, superior labial artery, infraorbital artery, and dorsal nasal artery. The rich vascularization, the mobility of the malar skin tissue, and the low risk of ischemic failure make this technique preferred for defects with less than 2.5cm in diameter.7 Melolabial interpolated flaps have good cosmetic results since the scar is hidden in the anatomical perinasal fold. The technique can be used in combination with local cartilaginous grafts to provide structural support and permeability of the nasal airways.7
The contraction of the wound may occur at the defect site, so the donor site must be smaller than the primary defect. This minimizes the so-called trapdoor effect during the healing phase.11
The most frequent cause of flap failure is the torsion of the pedicle, which can happen accidentally during surgery. 12,13 Correct transfer and placement of the flap are critical in the apposition of the flap with the adjacent tissue. Pedicle torsion may also occur during flap transfer, leading to reduced vascularization.13 The increased resistance of the vascular wall due to torsion of the pedicle leads to a slowing of blood flow, causing endothelial damage and finally resulting in the formation of a thrombus.14-17
The auricular cartilage graft is flexible, and presents similar characteristics in terms of curvature, therefore providing ideal structural support for the nostril. This combined treatment, a nasolabial flap with composite auricular graft, has been widely used, with several advantages. The combined technique is relatively easy to learn. It allows the reconstruction of larger defects, up to 2.0cm x 2.5cm, and gives better compatibility in terms of contour and coloring with the original tissue. The composite auricular graft is richly vascularized, which ensures a quicker grip and optimal graft survival.18 The cartilaginous graft is not restorative, but only provides structural support, including the maintenance of the nasal airway and the contour, also preventing tissue contraction.19 However, due to the malar tissue's turgor, cartilage graft may not be necessary, even in more substantial defects, except when the alar defect appears to be more prone to collapse.20
The melolabial interpolation flap is one of the preferred techniques for closing the defect due to basal cell carcinoma in the nasal ala. The combination with auricular cartilage graft improves the cosmetic result. Careful planning and meticulous reconstruction techniques are necessary for the outpatient setting.
The authors thank the patient for participating in the study.
Khairuddin Djawad | 0000-0002-4569-6385
Approval of the final version of the manuscript; study design and planning; preparation and writing of the manuscript; critical revision of the manuscript.
Amelia Setiawati Soebyanto | 0000-0003-3812-671X
Approval of the final version of the manuscript; study design and planning; preparation and writing of the manuscript; critical revision of the manuscript.
Airin R. Nurdin | 0000-0001-8277-2511
Approval of the final version of the manuscript; preparation and writing of the manuscript; data collection, analysis, and interpretation; critical revision of the manuscript.
Siswanto Wahab | 0000-0001-6952-6578
Approval of the final version of the manuscript; study design and planning; active participation in research orientation; critical revision of the manuscript.
Anis Irawan Anwar | 0000-0002-1830-5617
Approval of the final version of the manuscript; study design and planning; critical literature review; critical revision of the manuscript.
1. Cook JL. The lateral ala's volume and position are critical determinants of aesthetically successful nasal reconstruction: a photographic case series. Dermatol Surg. 2009;35(4):667-73.
2. Collins SC, Dufresne Jr RG, Jellinek NJ. The bilobed transposition flap for single-staged repair of large surgical defects involving the nasal ala. Dermatol Surg. 2008;34(10):1379-86.
3. Rahman H, Razib SFA, Azad MAK, Mannan, Bahar AA, Uddin M. Local flap for reconstruction of nasal defect following excision of basal cell carcinoma of nose. Bangabandhu Sheikh Mujib Med Univer J. 2016;9(4):208-11.
4. Burget GC. Aesthetic restoration of the nose. Clin Plastic Surg. 1985;12(3):463-80.
5. Wald J, Tinklepaugh A, Husain Z, Ciocon D. Alar Reconstruction After Failure of an Interpolated Melolabial Flap. Dermatol Surg. 2018;44(12):1623-6.
6. Summers BK, Siegle RJ. Facial cutaneous reconstructive surgery: facial flaps. J Am Acad Dermatol. 1993;29(6):917-41.
7. Lindsey WH. Reliability of the melolabial flap for alar reconstruction. Arch Facial Plast Surg. 2001;3(1):33-7.
8. Salgarelli AC, Bellini P, Multinu A, Magnoni C, Francomano M, Fantini F, et al. Reconstruction of nasal skin cancer defects with local flaps. J skin cancer. 2011;2011:181093.
9. Younger R. The versatile melolabial flap. Otolaryngol Head Neck Surg. 1992;107(6 part 1):721-6.
10. Mellette JR, Ho DQ. Interpolation flaps. Dermatol Clin. 2005;23(1):87-112.
11. Pharis DB, Papadopoulos DJ. Superiorly based nasolabial interpolation flap for repair of complex nasal tip defects. Dermatol Surg. 2000;26(1):19-24.
12. Chang C-H, Lim S-Y, Pyon J-K, Bang S-I, Oh K-S, Mun G-H. The influence of pedicle length on the viability of twisted perforator flaps in rats. J Reconst Microsurg. 2009;25(09):533-8.
13. Demir A, Acar M, Yldz L, Karacalar A. The effect of twisting on perforator flap viability: an experimental study in rats. An Plast Surg. 2006;56(2):186-9.
14. Salgarello M, Lahoud P, Selvaggi G, Gentileshci S, Sturla M, Farallo E. The effect of twisting on microanastomotic patency of arteries and veins in a rat model. An Plast Surg. 2001;47(6):643-6.
15. Topalan M, Bilgin SS, Ip WY, Chow SP. Effect of torsion on microarterial anastomosis patency. Microsurgery. 2003;23(1):56-9.
16. Acland R. Thrombus formation in microvascular surgery: an experimental study of the effects of surgical trauma. Surgery. 1973;73(5):766-71.
17. Ozbek MR, Deune EG, Cooley BC, Khouri RK. Experimental reproduction of free flap errors: a new model of thrombosis. An Plast Surg. 1994;32(5):474-7.
18. Qian C, Yaodong X, Xiaoming H, Shaochong F, Yiqing Z. Repair of full - thickness alar defects. Dermatol Surg. 2012;38(10):1639-44.
19. Nguyen T. Staged interpolation flaps. In: Roher T, Cook J, Nguyen T, editors. Flaps and grafts in dermatologic surgery. New York: Elsevier; 2007. p. 91-105.
20. Goldman GD, Dzubow LM, Yelverton CB. Facial Flap Surgery. McGraw-Hill; 2013.
 All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773
All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773



 Read in Portuguese
Read in Portuguese
 Portuguese PDF
Portuguese PDF
 Print
Print
 Send this article by email
Send this article by email
 How to cite this article
How to cite this article
 Submit a comment
Submit a comment
 Mendeley
Mendeley
 Pocket
Pocket
{kind=link}
{kind=link}
{kind=link}