


John Verrinder Veasey
Received on: 01/04/2019
Approved on: 25/10/2019
Financial support: None
Conflict of interests: None
Study conducted at private clinic , São Paulo (SP), Brazil.
Warts are the most frequent periungual tumors presented in dermatological consultations. They are caused by several types of human papillomavirus (HPV), and some of these lesions evolve to a spontaneous cure. However, there are lesions that do not regress without a therapeutic approach, and some of them are resistant to several therapies. I present a case of a 14-year-old patient with disseminated periungual warts in both hands, resistant to several previous therapies, and who evolved with cure after the use of occlusive imiquimod.
Keywords: Warts; Nails; Drug therapy; Drug therapy, combination; Immunotherapy; Immunotherapy, active; Neoadjuvant therapy
Viral warts are highly prevalent dermatoses in the population, usually affecting the extremities of the limbs. They arise from infection by human papillomavirus (HPV) types 1, 2, 4, 27 and 57.1,2 Its diagnosis is generally clinical, and an analysis can be performed using dermoscopy to reveal the digitiform projections and capillary dilations1,3 or even histopathological examination for diagnostic confirmation and exclusion of differential diagnoses such as squamous cell carcinoma (SCC).4,5 Considered as the most common nail tum or, they can occur around the nail plate, being called periungual warts, while those occurring below the nail are referred to as subungual warts.1
Warts can persist for years with little or no sign of inflammation. The spontaneous elimination of the infection can occur at any time, starting with a reduction in the size of the lesion and then progressing to its disappearance, a process that can last from a few months to years. Spontaneous healing in children can occur after just a few months, while in adults, the process can be much slower, with persistence for five to 10 years.5,6
The approach to treating warts encompasses three main forms: destructive treatments, use of antiproliferative agents, and immunological therapies.1,2,5,7,8,9 Destructive treatments are the most performed and those with the highest level of recommendation, and include the use of chemicals such as acid solutions, interventions such as cryotherapy, as well as the use of laser, electrofulguration, and surgical excision.1,6 Use of podophyllin,7 5-fluorouracil, and intradermotherapy with bleomycin2 exemplify treatments with antiproliferative agents. Treatments using immunological therapies can be performed systemically, such as oral administration of cimetidine, levamisole or zinc sulfate;10 intralesional application of several immunostimulatory antigens, such as Propionibacterium acnes;11 and using topical products applied on the sensitizing lesions, such as diphencyprone, or immunomodulators such as imiquimod (IQM).9
Topical imiquimod stimulates the immune response of the epithelium, both innate and adaptive, inducing the production of cytokines and migration of Langerhans cells.12,13 This allows its use for the treatment of a wide variety of benign and malignant skin conditions due to its potential antiviral, anti-tumor, and immunoregulatory effects.12 Currently, the regulatory agencies of the United States (Food and Drug Administration - FDA) and Brazil (Brazilian Health Regulatory Agency - ANVISA) approved topical imiquimod for the treatment of anogenital warts, actinic keratosis, and superficial basal cell carcinomas. However, several studies demonstrate its beneficial effect on the treatment of many other skin diseases, among them periungual warts. 5,12,14,15,16
I present the case of a 14-year-old immunocompetent patient with disseminated periungual warts on the fingers of both hands, resistant to several standard treatments, which evolved with an excellent response after the introduction of topical imiquimod.
We report a case of an atopic, immunocompetent, 14-year-old patient with lesions for two years. He refers to onychotillomania, which is why the lesions spread to all the fingers, and he has already undergone treatments during this period with cryotherapy, chemocautery, and electrocauterizations, without success.
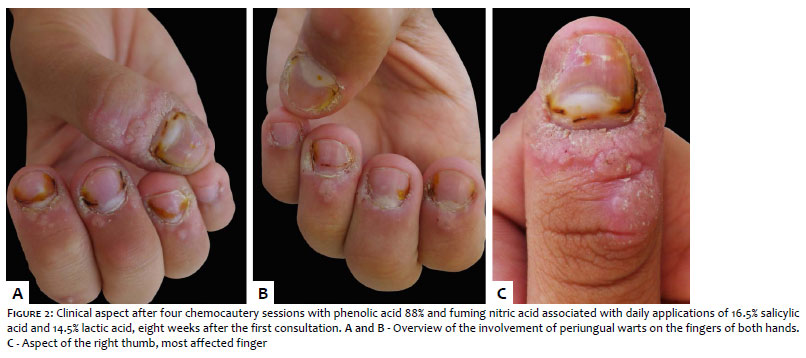
In his first consultation, he presented multiple periungual lesions in all fingers of both hands, with more exuberant involvement of the right thumb (Figure 1). A destructive treatment was proposed, with the application of phenol 88% in the clinic followed by application of fuming nitric acid in weekly sessions, associated with daily home use of a commercial solution of 16.5% salicylic acid and 14.5% lactic acid (SA+ LA). The patient did not attend the sessions regularly as planned, but maintained the home use of the solution, completing four sessions of application of the acids in eight weeks. Despite noticing a partial improvement in his condition, he reported a high impact on his quality of life due to the dark yellowish aspect that chemocautery left on his fingers, and requested changes in therapy (Figure 2).
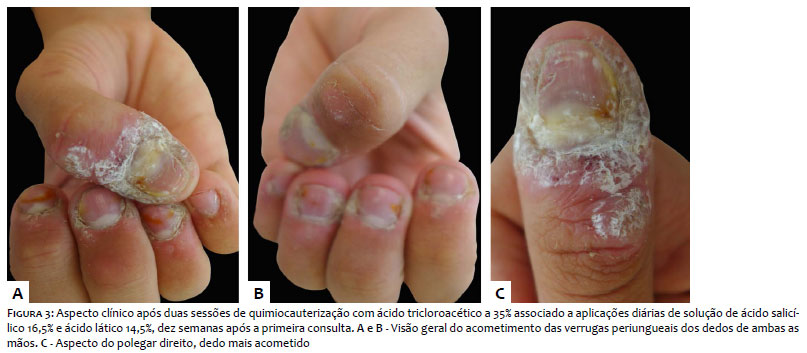
We opted to maintain a destructive approach, this time with weekly applications in the clinic of trichloroacetic acid 35% associated with the use of SA + LA daily at home. After two weekly sessions, he again reported discomfort due to the whitish aspect that the warts keratin presented (Figure 3); thus, it was decided to change the therapy again. Due to the history of using various destructive treatments previously and before his first consultation, during the ten-week follow-up at the clinic, we decided to change the approach to an immunostimulatory. He was instructed to keep using SA + LA daily in the morning and imiquimod 5% cream in occlusion at night for five consecutive days a week. The patient applied the cream and occluded it with a bandage from Monday to Friday; on Saturday and Sunday, he only used morning SA + LA.
After four weeks of using SA + LA every morning and occlusive IQM on five consecutive nights a week, the patient showed complete regression of the condition, with no impact on quality of life during treatment due to color changes as previously reported in other approaches, without complaints of pain, irritation or ulceration of the lesions (Figure 4).
The use of IQM to treat periungual warts has been described with different results. An open trial assessed the efficacy, safety, and tolerability of imiquimod 5% topical cream in 15 patients with resistant and recurrent periungual and subungual warts over 16 weeks. Twelve patients (80%) completed the therapy, presenting complete resolution after a mean of three weeks and with no recurrences after six months. 16 On the other hand, an evidence-based review conducted by Cochrane on the effectiveness of IQM in the treatment of extragenital warts showed a rate ranging from 27% to 89% of patients who achieved a complete response.15
The frequency and application of the product varied considerably from study to study, with authors who used it only three times a week to others who prescribed it five times a week, occlusive, and associated with keratolytics.5 Another review on the use of IQM in extragenital warts concluded, based on small case series and case reports, that its combination with destructive or keratolytic treatments can improve the penetration of the topical IQM and lead to better clinical outcomes.5 We opted for this more aggressive dosage in the case presented, given the chronicity and exuberance of the lesions, seeking a more significant immune mobilization of the patient and a higher chance of obtaining a satisfactory response. It is noteworthy that due to the mechanism of action of the drug is based on a stimulus of the skin immune response, cases of warts in patients with immunosuppression or using immunomodulatory drugs tend not to have a satisfactory response.5,12,13,15
Another aspect that favors the use of IQM is its tolerability with few adverse events when compared to other commonly used modalities.16 In the case presented, one of the reasons for the patient's low adherence to the several treatments was precisely the adverse event caused by traditional therapies, which did not occur with the topical immunostimulator.
More randomized controlled studies are needed to determine the efficacy of the IQM, assessing the frequency of dose and application as well as its ideal combination with other therapeutic measures in the treatment of periungual warts. However, the knowledge of successful cases such as the one presented here becomes valid to have an alternative treatment option in cases resistant to standard treatments.
The present report demonstrates that the treatment of periungual warts with topical immunotherapy using imiquimod seems to be a valid therapeutic option, especially when associated with keratolytics such as the formulation of lactic acid and topical salicylic acid.
John Verrinder Veasey | 0000-0002-4256-5734
Approval of the final version of the manuscript; study design and planning; preparation and writing of the manuscript; data collection, analysis, and interpretation; active participation in research orientation; intellectual participation in propaedeutic and/or therapeutic conduct of studied cases; critical literature review; critical revision of the manuscript.
1. Herschthal J, McLeod MP, Zaiac M. Management of ungual warts. Dermatol Ther. 2012;25(6):545-50.
2. Noriega LF, Valandro LS, Di Chiacchio NG, Vieira ML, Di Chiacchio N. Treatment of viral warts with intralesional bleomycin. Surg Cosmet Dermatol. 2018;10(1):16-20.
3. Veasey JV, Framil VMS, Nadal SR, Marta AC, Lellis RF. Genital warts: comparing clinical findings to dermatoscopic aspects, in vivo reflectance confocal features and histopathologic exam. An Bras Dermatol. 2014;89(1):137-40.
4. Riddel C, Rashid R, Thomas V. Ungual and periungual human papillomavirus-associated squamous cell carcinoma: a review. J Am Acad Dermatol. 2011;64(6):1147-53.
5. Ahn CS, Huang WW. Imiquimod in the treatment of cutaneous warts: an evidence-based review. Am J Clin Dermatol. 2014;15(5):387-99.
6. Sterling JC, Gibbs S, Haque Hussain SS, Mohd Mustapa MF, Handfield-Jones SE. British Association of Dermatologists' guidelines for the management of cutaneous warts 2014. Br J Dermatol. 2014;171(4):696-712.
7. Veasey JV, Dall'Antonia M, Miguel BAF, Mayor SAS, Campaner ABC, Manzione TS. Anogenital condylomas in children: descriptive analysis of 20 cases. Surg Cosmet Dermatol 2017;9(2):127-9.
8. Nofal A, Nofal E, Yosef A, Nofal H. Treatment of recalcitrant warts with intralesional measles, mumps, and rubella vaccine: a promising approach. Int J Dermatol. 2015;54(6):667-71.
9. Nofal A, Salah E, Nofal E, Yosef A. Intralesional antigen immunotherapy for the treatment of warts: current concepts and future prospects. Am J Clin Dermatol. 2013;14(4):253-60.
10. Stefani M, Bottino G, Fontenelle E, Azulay DR. Efficacy comparison between cimetidine and zinc sulphate in the treatment of multiple and recalcitrant warts. An Bras Dermatol. 2009;84(1):23-9.
11. Nasser N. Treatment of common warts with the immune stimulant Propionium bacterium parvum. An Bras Dermatol. 2012;87(4):585-9.
12. Hanna E, Abadi R, Abbas O. Imiquimod in dermatology: an overview. Int J Dermatol. 2016;55(8):831-44.
13. Suzuki H, Wang B, Shivji GM, Toto P, Amerio P, Tomai MA, Miller RL, Sauder DN. Imiquimod, a topical immune response modifier, induces migration of Langerhans cells. J Invest Dermatol. 2000;114(1):135-41.
14. Veasey JV, Miguel BAF, Campaner AB, Manzione TS. Imiquimod use for the treatment of extramammary Paget disease: series of four cases. Surg Cosmet Dermatol. 2018;10(4):309-13.
15. Kwok CS, Gibbs S, Bennett C, Holland R, Abbott R. Topical treatments for cutaneous warts. Cochrane Database Syst Rev. 2012;(9):CD001781.
16. Micali G, Dall'Oglio F, Nasca MR. An open label evaluation of the efficacy of imiquimod 5% cream in the treatment of recalcitrant subungual and periungual cutaneous warts. J Dermatolog Treat. 2003;14(4):233-6.
 All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773
All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773



 Read in Portuguese
Read in Portuguese
 Portuguese PDF
Portuguese PDF
 Print
Print
 Send this article by email
Send this article by email
 How to cite this article
How to cite this article
 Submit a comment
Submit a comment
 Mendeley
Mendeley
 Pocket
Pocket
{kind=link}
{kind=link}
{kind=link}
{kind=link}