


Manuela da Silva1; Alexandre de Almeida Filippo2; Paula Regazzi de Gusmão1
Received on: 12/01/2019
Approved on: 09/11/2019
Financial support: None
Conflict of interests: None
Research conducted at the Institute of Dermatology Professor Rubem David Azulay, Santa Casa de Misericórdia do Rio de Janeiro, Rio de Janeiro (RJ), Brazil
INTRODUCTION: The treatment of hypochromic scars is challenging, and the techniques used so far show unsatisfactory results. Bimatoprost, an analog of prostaglandin F2-alpha, has been used as a topical pigment agent, and its application as drug delivery can optimize its delivery to the dermis and potentiate pigmentation.
OBJECTIVE: To evaluate the safety and efficacy of Ablative Fractional Laser (AFL) treatment associated with bimatoprost 0.03% drug delivery in hypopigmented scars.
METHODS: The patients were submitted to the AFL, followed by the application of bimatoprost 0.03% in 4 sessions with biweekly intervals. Clinical evaluations and standardized photographs were performed. Patients’ satisfaction was assessed using a 5-question questionnaire.
RESULTS: All patients had clinical improvement in the treated areas. The degree of patient satisfaction agreed with the clinical evaluation and photographic records.
CONCLUSION: The application of AFL associated with bimatoprost 0.03% drug delivery can be a potentially effective and safe treatment for hypochromic scars.
Keywords: Lasers; Hypopigmentation; Laser Therapy
Hypochromic scars are common complications in patients undergoing deep exfoliative surgical procedures and after traumatic wounds or burns.1,2 Treatment of hypochromia is challenging, and none of the methods described in the literature has proven completely effective thus far.
Bimatoprost has been used in a growing number of studies with the objective of promoting pigmentation of hypochromic lesions of various etiologies. Thus, like latanoprost and travoprost, bimatoprost is an analog of prostaglandin F2-alpha (PGF2-alpha). PGF2-alpha analogs are used in the treatment of glaucoma, and their dermatological importance lies in one of their principal side effects: skin hyperpigmentation.3,4,5,6,7,8,9,10
The mechanism by which hyperpigmentation occurs has not been completely elucidated, but it is inferred to occur through a process similar to that caused by ultraviolet radiation and inflammation. Both induce the production of prostaglandins, which act by stimulating dermal melanocytes.11 Anbar et al. further suggest that activation of prostaglandin receptors can promote dendritic proliferation in melanocytes and increase tyrosinase expression, factors that purportedly contribute to increasing skin pigmentation.3,12,13,14 Prostaglandin analogs have been used especially to treat vitiligo, and various case series and clinical trials have been published with promising results3,4,5,13,15,16
The use of bimatoprost in the treatment of hypochromia is limited basically to its topical application on the intact skin or in the form of drug delivery associated with different types of technologies.17.18
Ablative fractional laser (AFL) increases the penetrative capacity of drugs applied in the form of drug delivery.19,20 Clinical trials have shown that the channels produced by AFL provide successful delivery of small particles in the dermis, whether hydrophilic or lipophilic.21 The technology breaks the skin barrier and creates vertical channels in the treated tissue, surround by zones of healthy tissue. Such channels facilitate the penetration and absorption of active ingredients in skin, besides allowing rapid reepithelization due to the adjacent zones of healthy skin.
This pilot studies assesses the safety and efficacy of treatment of hypopigmented scars using AFL associated with drug delivery of bimatoprost 0,03% in four patients.
Four patients (from 16 to 53 years of age, Fitzpatrick skin types II-V) with hypochromic scars were submitted to treatment with AFL (2940nm, Plataforma Etherea® -Vydence Medical Brazil, São Carlos, SP, Brazil), followed by application of bimatoprost 0,03% in the form of drug delivery.
Patients underwent the treatment after signing an informed consent form. The research project was approved by the Institutional Review Board of Souza Marques Technical Educational Foundation (CAAE: 90753218.8.0000.5239).
Case 1 (Figure 1) presents a hypochromic scar on the neck following a burn with an electric wire. Case 2 (Figure 2) displays hypochromic scars on the face after a CO2 laser resurfacing procedure. Case 3 (Figure 3) shows a hypochromic scar on the neckline following surgical removal of an epidermal cyst. Case 4 (Figure 4) shows a hypochromic scar on the malar region after a burn from Nd:YAG (1064nm) long pulse laser for treatment of facial telangiectasias. All the respective scars had a history of more than a year of evolution.
Patients were submitted to treatment with AFL followed by application of 0,03% bimatoprost solution with local massage. The parameters were: energy: 12,5mj; pulse: 300 microseconds; tip 100mtz/cm². The substance was maintained on the treatment site for a minimum of six hours, and was removed with local washing with water. Four sessions were performed, at two-week intervals.
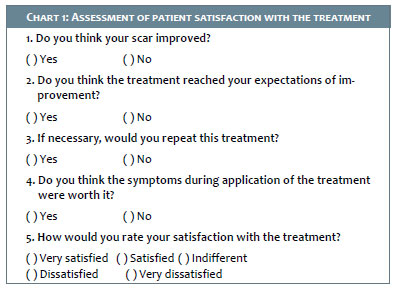
Photographs were taken in the same setting before the treatment and 30 days after the last session. Patient satisfaction with the treatment was assessed with a five-item questionnaire (Chart 1).
Follow-up examination at four weeks after the last session showed that all the patients obtained clinical improvement in the treated areas. Patient satisfaction coincided with our clinical evaluation and with the photographic records. Two patients were satisfied with the results and two others were very satisfied. All four answered “yes” to the other questions, except for one female patient who responded that the treatment had not reached her expectations of improvement, although she was satisfied. Figures 1, 2, 3, and 4 show the results.
Besides AFL, the treatment modalities used thus far include cosmetic tattooing, medium-depth chemical peels, dermabrasion, skin graft, cosmetic camouflage, and various forms of phototherapy and other laser therapies.2 AFL has been the technology of choice for promoting drug delivery in the majority of the recently published studies. The break in the stratum corneum with the formation of microchannels surrounded by a coagulation zone allows the active ingredients’ effective and relatively controlled penetration. Waibel et al. assume that the area of denatured tissue surrounding the microchannels can function as a barrier that maintains the active ingredients in the dermis, thus reducing their systemic absorption and consequently making the procedure safer.22
The low density and low fluency used in this case are consistent with the settings described in the literature.22,23,24 Such settings are based on a study by Bachhav et al.., showing that there is a minimum density of channels needed to reach maximum penetration of the active ingredients, and there is no improvement in delivery when these values are increased. Meanwhile, low fluencies ensure a favorable thermal damage zone and produce microchannels with adequate depth to maintain the active ingredients in the dermis.22,23,25 The efficacy of the use of bimatoprost in the treatment of hypochromic lesions was assessed by Massaki et al. and Regis et al. in recently published studies.17,18 In both, the authors used bimatoprost in the form of drug delivery in association with topical application at the patient’s home. In the current case series, bimatoprost was only used in the form of drug delivery, which allowed evaluating this method’s efficacy alone, which had not been described previously in the literature. All four patients obtained improvement in the treated areas and expressed satisfaction with the procedure. Still, we hypothesize that maintaining the treatment sessions and home application of bimatoprost on the treated areas can help obtain superior results to those observed here.
This pilot study shows that the application of AFL associated with drug delivery of bimatoprost 0,03% can be a potentially safe and effect treatment of hypochromic scars.
Long-term follow-up is recommended to measure the sustainability of this response. Controlled studies with larger patient samples are necessary to assess the role of AFL and bimatoprost in the pigmentation of hypochromic scars. Still the current results demonstrate that this can be a promising treatment.
Manuela da Silva | 0000-0003-4419-6722
Approval of the final version of the manuscript; conception and planning of the study; elaboration and writing of the manuscript; data collection, analysis, and interpretation; effective participation in the orientation of the research; intellectual participation in the propaedeutic and/or therapeutic management of the study cases; critical review of the literature; critical revision of the manuscript.
Alexandre de Almeida Filippo | 0000-0001-9550-5156
Approval of the final version of the manuscript; conception and planning of the study; effective participation in the orientation of the research; intellectual participation in the propaedeutic and/or therapeutic management of the study cases; critical review of the literature; critical revision of the manuscript.
Paula Regazzi de Gusmão | 0000-0002-7060-6062
Approval of the final version of the manuscript; critical revision of the manuscript.evisão crítica do manuscrito.
1. Massaki AB, Fabi SG, Fitzpatrick R. Repigmentation of hypopigmented scars using an erbium-doped 1,550-nm fractionated laser and topical bimatoprost. Dermatol Surg. 2012;38(7 Pt 1):995-1001.
2. Goodman GJ. An automated autologous cell transplantation method for the treatment of hypopigmented scarring. Dermatol Surg. 2008;34(4):578-81.
3. Anbar TS, El-Ammawi TS, Abdel-Rahman AT, Hanna MR. The effect of latanoprost on vitiligo: a preliminary comparative study. Int J Dermatol. 2015;54(5):587-93.
4. Jha AK, Prasad S, Sinha R. Bimatoprost in vitiligo. Clin Exp Dermatol. 2016;41(7):821-2.
5. Choi YM, Diehl J, Levins PC. Promising alternative clinical uses of prostaglandin F2a analogs: beyond the eyelashes. J Am Acad Dermatol. 2015;72(4):712-6.
6. Patil AJ, Vajaranant TS, Edward DP. Bimatoprost - a review. Expert Opin Pharmacother. 2009;10(16):2759-68.
7. Doshi M, Edward DP, Osmanovic S. Clinical course of bimatoprost- induced periocular skin changes in Caucasians. Ophthalmology. 2006;113(11):1961-7.
8. Priluck JC, Fu S. Latisse-Induced Periocular Skin Hyperpigmentation. Arch Ophthalmol. 2010;128(6):792-3.
9. Inoue K, Shiokawa M, Higa R, Sugahara M, Soga T, Wakakura M, et al. Adverse periocular reactions to five types of prostaglandin analogs. Eye (Lond). 2012;26(11):1465-72.
10. Sharpe ED, Reynolds AC, Skuta GL, Jenkins JN, Stewart WC. The clinical impact and incidence of periocular pigmentation associated with either latanoprost or bimatoprost therapy. Curr Eye Res. 2007;32(12):1037-43.
11. 11.Kapur R, Osmanovic S, Toyran S, Edward DP. Bimatoprost-induced periocular skin hyperpigmentation: histopathological study. Arch Ophthalmol. 2005;123(11):1541-6.
12. Scott G, Leopardi S, Printup S, Malhi N, Seiberg M, Lapoint R. Proteinase- Activated Receptor-2 Stimulates Prostaglandin Production in Keratinocytes: Analysis of Prostaglandin Receptors on Human Melanocytes and Effects of PGE2 and PGF2a on Melanocyte Dendricity. J Invest Dermatol. 2004;122(5):1214-24.
13. Parsad D, Pandhi R, Dogra S, Kumar B. Topical prostaglandin analog (PGE2) in vitiligo-a preliminary study. Int J Dermatol. 2002;41(12):942-5.
14. Prota G, Vincensi MR, Napolitano A, Selen G, Stjernschantz J. Latanoprost stimulates eumelanogenesis in iridial melanocytes of cynomolgus monkeys. Pigment Cell Res. 2000;13(3):147-50.
15. Jha AK, Sinha R, Prasad S, Nandan N. Bimatoprost in periorbital vitiligo: a ray of hope or dilemma. J Eur Acad Dermatol Venereol. 2016;30(7):1247-8.
16. Kapoor R, Phiske MM, Jerajani HR. Evaluation of safety and efficacy of topical prostaglandin E2 in treatment of vitiligo. Br J Dermatol. 2009;160(4):861-3.
17. Regis A, MacGregor J, Chapas A. Fractional Resurfacing and Topical Bimatoprost for the Treatment of Laser Induced Postinflammatory Hypopigmentation on the Lower Extremities. Dermatol Surg. 2018;44(6):883-6.
18. Massaki AB, Fabi SG, Fitzpatrick R. Repigmentation of hypopigmented scars using an erbium-doped 1,550-nm fractionated laser and topical bimatoprost. Dermatol Surg. 2012;38(7 Pt 1):995-1001.
19. Ali FR, Al-Niaimi F. Laser-assisted drug delivery in dermatology: from animal models to clinical practice. Lasers Med Sci. 2016;31(2):373-81.
20. Issa MC, Kassuga LE, Chevrand NS, Pires MT. Topical delivery of triamcinolone via skin pretreated with ablative radiofrequency: a new method in hypertrophic scar treatment. Int J Dermatol. 2013;52(3):367-70.
21. Banzhaf CA, Thaysen-Petersen D, Bay C, Philipsen PA, Mogensen M, Prow T, et al. Fractional laser-assisted drug uptake: Impact of time-related topical application to achieve enhanced delivery. Lasers Surg Med. 2017;49(4):348-54.
22. Waibel JS, Rudnick A, Shagalov DR, Nicolazzo DM. Update of Ablative Fractionated Lasers to Enhance Cutaneous Topical Drug Delivery. Adv Ther. 2017;34(8):1840-9.
23. Bloom BS, Brauer JA, Geronemus RG. Ablative fractional resurfacing in topical drug delivery: an update and outlook. Dermatol Surg. 2013;39(6):839-48.
24. Braun SA, Schrumpf H, Buhren BA, Homey B, Gerber PA. Laser assisted drug delivery: mode of action and use in daily clinical practice. J Dtsch Dermatol Ges. 2016;14(5):480-8.
25. Bachhav YG, Summer S, Heinrich A, Bragagna T, Böhler C, Kalia YN. Effect of controlled laser microporation on drug transport kinetics into and across the skin. J Control Release. 2010;146(1):31-6.
 All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773
All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773



 Read in Portuguese
Read in Portuguese
 Portuguese PDF
Portuguese PDF
 Print
Print
 Send this article by email
Send this article by email
 How to cite this article
How to cite this article
 Submit a comment
Submit a comment
 Mendeley
Mendeley
 Pocket
Pocket
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}