


Rogério Nabor Kondo; Rubens Pontello Junior; Suellen Gonçalves dos Reis; Cássio Rafael Moreira
Received on: 16/05/2019
Approved on: 10/11/2019
Financial support: None
Conflict of interests: none
Research performed at the Dermatology Service of Hospital Universitário do Norte do Paraná, Universidade Estadual de Londrina, Londrina (PR), Brazil
INTRODUCTION: Ingrown toenail is the leading cause of nail surgery. Techniques have been described for better exposure of the nail matrix in Grade III treatment, such as block excision of the hypertrophic skin margins and the subcutaneous nail blade involved, removing a semi-elliptic wedge and or L-incision, both advocating closure by suturing the skin and the nail blade. Authors describe the application of an incision technique at the intersection of the lateral and proximal nail fold to expose the matrix and the performing of a wedge in the cutaneous hypertrophy. At the site of the nail blade removal a fragment is left by second intention.
OBJECTIVE: To assess the comfort and effectiveness of the new surgical technique for onychocryptosis.
METHODS: Observational and retrospective study through the analysis of 29 patients with onychocryptosis who underwent the new technique.
RESULTS: Of the 34 nail folds (5 patients had 2 affected nail folds) submitted to surgery using the new technique, only one patient had recurrence in one of the folds and underwent a new intervention. No complaints of postoperative discomfort or complications were observed.
CONCLUSIONS: The applied technique was satisfactory, with a low recurrence rate, and also easy to perform, presenting no discomfort complaints from patients.
Keywords: onychocryptosis; ingrown toenail; operative treatment; surgical technique
Subcutaneous onychocryptosis (SO), onychocryptosis, or ingrown toenail (IT) results from penetration of the nail blade into the underlying soft tissue.1,2 SO is prevalent in young and adult males (3:1), can present high morbidity, and may be disabling.2,3 The etiology is multifactorial, featuring: heredity, overly convex nail blade, disproportion between the width of the plate and the nail bed, chronic trauma, use of narrow-tipped or overly tight shoes, and inadequate trimming of toenails.1-3
Ingrown toenail can be classified by degree of severity (Heifetz, 1937):2,3 1) Grade I, presence of inflammatory signs (erythema, mild edema, and pain on compression of the lateral nail fold; 2) Grade II, when the inflammation increases with the emergence of exudate, secondary infection, and local drainage; 3) Grade III, with the formation of granulation tissue and lateral nail fold hypertrophy.1-3
The literature cites different forms of management for SO, both conservative and surgical. Conservative techniques are recommended in grade I, such as the use of bracing. In grades II and III, surgical treatment offers the best results. The techniques used are matricectomy, phenolization, nail blade excision,1-3 correction of hypertrophy in U,4 radiofrequency electrosurgery, and cryosurgery.2
In surgical matricectomy of grade III ingrown toenail, the literature cites the semi-spindle wedge and L-incision approach, which corrects the hypertrophies in the same incision.1 These techniques allow visualizing the nail matrix to be removed, but it is recommended to place sutures between the skin and the preserved nail blade for closure of the large open area.1,5
The monofilament nylon sutures are left in place until removal at about two weeks. During this time, the current authors heard reports from patients of both discomfort in the visualization of the sutures involving the nail blade and in removal of the stitches.
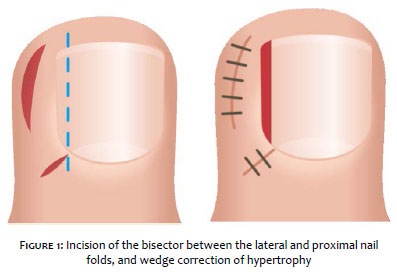
The authors propose a technique with the incision of the intersection of the lateral and proximal nail folds to expose the matrix, and a wedge in the middle of the hypertrophic skin (without removing it entirely), in the same surgical intervention. The site where the blade fragment is removed is allowed to heal by second intention, since it results in a small open strip. The advantage is a slightly less invasive treatment, without the negative sensation of seeing the blade sutured and the discomfort of removing the stitches from the toenail (Figure 1).
This was a retrospective observational study of patients over 12 years of age of both sexes who appeared spontaneously to the Clinical Specialties Outpatient Clinic (AHEC) of the State University of Londrina (UEL), Paraná State, Brazil, in the minor surgery clinic of the Dermatology Department on Tuesday afternoons, with diagnosis of onychocryptosis grades II and III. All cases were authorized by informed consent, including photographs of the cases (by parents or guardians in cases of minors), as part of the Department's protocol. The sample excluded cases with bilateral and anterior hypertrophy in the same patient (due to the need for correction in U), diabetes mellitus, peripheral artery disease, and coagulation disorders.
The data were analyzed and processed with the GraphPadInstat package and Excel 2007. Statistical significance was analyzed with the chi-square test with significance set at 5% (p<0,05), applied to compare sex and relapses. A convenience sample was used (all patients with onychocryptosis who underwent the surgery according to the Department's technique from January 1, 2011, to November 30, 2018, were followed during the study period).
Patients kept the dressing in place for 24 hours. The following medications were prescribed: common analgesics (paracetamol or dipyrone), azithromycin 500mg for three days or sulfamethoxazole and trimethoprim 400/80mg, two pills every 12 hours for ten days, according to the Department's protocol.
Patients were reassessed on the 3rd day post-op and on the 14th day, when the sutures were removed. Patients were assessed for history of pain, discomfort, annoyance with the stiches, bleeding, and/or secretions during the postoperative period, and clinical assessment of the operatory wound was performed in the same session. In addition to the preoperative photos, photos were taken in the postoperative period (day 3, day14, three months, and six months) and used to compare improvement after the procedure.
1. Patient in horizontal supine position with leg flexed over the thigh on the side of the affected toe;
2. Marking with methylene blue or surgical pen;
3. Antisepsis with 10% topical polyvinyl iodine;
4. Placement of surgical drapes;
5. Trunk block anesthesia with 2% lidocaine, without vasoconstrictor;
6. Tourniquet at the base of the toenail;
7. Incision at the bisector between the lateral and proximal nail folds (diagonal incision) for better visualization of the matrix;
8. Excision of granulation tissue via linear incision from proximal nail fold to anterior edge (about 3mm of blade width);
9. Undermining of the nail plate from the free edge to the matrix;
10. Sectioning of the nail plate from the free edge to the lateral horn of the matrix;
11. Removal of the nail plate;
12. Curettage of the lateral nail bed;
13. Suturing of the diagonal incision with simple 4.0 monofilament nylon stitches;
14. Wedge incision in the center of the lateral skin hypertrophy, maintaining the edges of the hypertrophy;
15. Removal of the hypertrophic wedge;
16. Suturing of the wedge with simple 4.0 monofilament nylon stitches;
17. Removal of tourniquet;
18. Occlusive dressing.
The sample included 29 patients with 34 affected nail folds (five patients presented two affected sites). Of these folds, seven had undergone some form of prior treatment (patients were unable to report what kind of surgery had been performed), with no improvement.
There were 17 men (59%) and 12 women (41%), but without statistical significance in the distribution by sex (p=1.0). Age ranged from 12 to 65 years, with a mean of 31,86 years.
All the affected nail folds were on halluces (34/34), statistically significant when compared to the other toes (0/34), p=0.0001. There were 15 folds on the right hallux and 19 on the left hallux, with no statistically significant difference between the two sides (p=0.88).
The sutures were removed at two weeks, during which time the patients were excused from their daily work or school activities. The patient charts showed no reports of local infection, bleeding, or intense pain during the postoperative period, major discomfort with the stitches during this period, or relevant pain during removal of the stitches. The surgical sites were described as having a good appearance, and there were also postoperative photographs.
Although we obtained no information on the previous techniques used, the patients with the seven prior surgeries (relapsed onychocryptosis) reported less discomfort with the technique applied in the current study.
The initially recommended follow-up was 12 months, but the patients abandoned follow-up after six months, for undisclosed reasons. However, this did not result in their exclusion from the study, since they were all clinically well.
One patient who had two affected nail folds on her left hallux had to undergo a procedure on the medial fold due to relapse (1/34 folds or 2.9% relapse rate), three months after the first surgery at our clinic.
Ingrown toenail is a painful condition with relevant morbidity, a frequent cause of work absenteeism.2 Conservative treatment is still recommended for grade I, with bracing, orientation on filing lateral nail edges, and use of comfortable footwear. However, grades II and III show better results with surgical treatment.2,3
The pain and inflammation result from penetration by the nail blade into the adjacent tissue, causing a foreign body reaction. Partial or total removal of the blade is necessary. 2
The literature also cites matricectomy (surgical or chemical), together with partial removal of the nail blade, to avoid relapses.1,6,7,8-10 Wedge and L-incisions are used to improve visualization of the matrix. However, the open defect is large, requiring closure with suturing between the skin and the remaining blade. This may cause patients some discomfort, including when removing their shoes.
The current study found that the condition was more prevalent in males, and that the hallux toenail was the most frequently affected, in agreement with the literature.2,3 Postoperative pain was well tolerated with common analgesics, as with other techniques,2,3,7 but with satisfactory results (without infection or bleeding, for example) and a low relapse rate (2.9%), although the study sample was small.
Although various techniques for suturing the surgical wound have been described,3,5,8-10 the new technique proposed here has the following advantages:
a) simple to perform;
b) for better visualization of the matrix, an incision is made at the bisector between the lateral and proximal nail folds (diagonal incision), where the open area is smaller;
c) only a thin strip of the nail blade (about 3mm) is removed from one of the folds;
d) Adjacent tissue is spared, since a wedge is removed from the center of the hypertrophic area, without removing everything, which also leaves less open area;
e) not suturing the blade produces less negative sensation for the patient, both in the postoperative period and when removing the stitches.
Although the number of patients is small, the results show that the technique is easy to perform, low-cost, well-tolerated by patients, and with good cosmetic results (Figures 3, 4, and 5).
Rogério Nabor Kondo | 0000-0003-1848-3314
Approval of the final version of the manuscript; conception and planning of the study; elaboration and writing of the manuscript; data collection, analysis, and interpretation; effective participation in the orientation of the research; intellectual participation in the propaedeutic and/or therapeutic management of the study cases; critical review of the literature; critical revision of the manuscript.
Rubens Pontello Junior | 0000-0002-2101-9080
Approval of the final version of the manuscript; elaboration and writing of the manuscript; critical review of the literature; critical revision of the manuscript.
Suellen Gonçalves dos Reis | 0000-0001-9307-4065
Elaboration and writing of the manuscript; intellectual participation in the propaedeutic and/or therapeutic management of the study cases; critical review of the literature; critical revision of the manuscript.
Cássio Rafael Moreira | 0000-0002-8781-1505
Elaboration and writing of the manuscript; intellectual participation in the propaedeutic and/or therapeutic management of the study cases; critical review of the literature; critical revision of the manuscript.
1. Di Chiacchio N. Manejo da Onicocriptose (Unha Encravada) e Ablação da Unha. In: Gadelha AR, Costa IMC, editors. Cirurgia Dermatológica em Consultório. São Paulo: Atheneu; 2002. p.223-34.
2. Reis CMS, Reis Filho EGM. Radioelectrosurgery and cryosurgery in ingrown nails. Surg Cosmet Dermatol. 2010;2(3):180-3.
3. Lucares DO, Rodriguez JJ, Leverone A, Nakamura RC. Benefits of the alpha stitch technique in surgical closure in onychocryptosis. Surg Cosmet Dermatol. 2012;4(4):310-4.
4. Sánchez-Regaña M. Super U Technique for Ingrown Nails. Actas Dermosifiliogr. 2017;108(5):393.
5. Eirís Salvado N, Rodríguez Prieto MA. Suturing the nail plate during matricectomy. J Am Acad Dermatol. 2016;75(3):e107.
6. Chiacchio N, Belda Júnior W, Chiacchio NG, Gabriel FVK, Farias DC. Nail matrix phenolization for treatment of ingrowing nail: technique report and recurrence rate of 267 surgeries. Dermatol Surg. 2010;36(4):534-7.
7. Vaccari S, Dika E, Balestri R, Rech G, Piraccini BM, Fanti PA. Partial excision of matrix and phenolic ablation for the treatment of ingrowing toenail: a 36-month follow-up of 197 treated patients. Dermatol Surg. 2010;36(8):1288-93.
8. Mousavi SR, Khoshnevis J. A new surgical technique for ingrown toenail. ISRN Surg. 2012; 2012(2):1-4.
9. Uygur E, Çarkçi E, Şenel A, Kemah B, Turhan Y. A new and simple suturing technique applied after surgery to correct ingrown toenails may improve clinical outcomes: A randomized controlled trial. Int J Surg. 2016;34:1-5.
10. Camurcu Y, Sofu H, Issin A, Kockara N, Saygili H. Operative Treatment of the Ingrown Toenail With a Less-Invasive Technique: Flashback to the Original Winograd Technique. Foot Ankle Spec. 2018;11(2):138-141.
 All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773
All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773



 Read in Portuguese
Read in Portuguese
 Portuguese PDF
Portuguese PDF
 Print
Print
 Send this article by email
Send this article by email
 How to cite this article
How to cite this article
 Submit a comment
Submit a comment
 Mendeley
Mendeley
 Pocket
Pocket
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}